EXISTENCE-OK
History
of all Medicine
Natural
History of Medicine
Integrative
Medicine
Review Edited and
Compiled Histories of Medicines by
Oko Offoboche
April 2022
existence-ok.com
Abstract: This is the History of every Medicine from the indigenes point of
view and not another race or tribe smearing the other for dominance in Nature
from the period of paradise through the time of good and evil, to correct the
fall of the health of humankind back to the tree of life that is living with an
addition of spirit instead of living carnally with soul alone. Humans become
smarter when they live in their spirit that is all knowing to become true human
beings. Read the Medicines traditional or/ and complementary to you.
Brief about the reviewser/ author/s:
Oko Offoboche was nominated as Head of
Department by an Institute and University in the United States before he was
awarded a Professorship in Philosophy of Metaphysics by a United States
University; before then he had a Doctorate degree in Philosophy of Metaphysics,
a Doctorate of Science in Information Systems, a Master of Science in
Information Systems Management and bachelor degree in Information Systems and Metaphysics.
Professor Offoboche has a degree in Acupuncture from a Nigerian College and an
International diploma in Acupuncture from a University in Siri Lanka, an
Advanced Certificate in Traditional Chinese Medicine in a Tianjin University in
China, Diplomas in Natural Medicine from one of the old Academy in Lagos.
Professor Oko Offoboche had a max CGPA. He is in many associations covering his
disciplines internationally and locally. He was given professor status by the
All Certified Professionals of Traditional, Complementary and Alternative
Medicine, African University of Natural Medicine in view that is a branch of
Nigerian Council of Physicians. He is a Fellow in many bodies including; Fellow
of Association of Integrative Medicine Practitoners, Fellow of Institute
Information Management, Fellow of Information Management Consultants. His late
father was a medical doctor who specialized as a gyaenecologists with doctorate
degree and his late grandfather was a revered native doctor.
Metaphysicians
at a high level see what was already there before physical records were kept; that
is why it was better for humankind that I compile all records of medicine for
easy use by future generations. I implore the authors that it is better for
students not to search for different parts of medicine, but be pleased their
works were chosen to be like the bible (that was compiled) for medicine.
Why the author was proficient to write this?
met�a�phys�ics [m�ttə
f�zziks]
noun
1. philosophy of being: the
branch of philosophy concerned with the study of the nature of being and
beings, existence, time and space, and causality (takes a singular verb)
2. underlying principles:
the ultimate underlying principles or theories that form the basis of a
particular field of knowledge (takes a plural verb)
�Symmetry is part of the
metaphysics of quantum mechanics.
3. abstract thinking:
abstract discussion or thinking (takes a singular verb)� c
Authors and works added by reviewer:
1. Dr. B. L. Dickson; The Black Race; DNA And Why!?
2. Rochelle Forrester; The History of Medicine
3. Wagner; The Origins and History of Medicine and Medical Practiced
4. History of use of Traditional Herbal Medicines
5. H. J. O'D. Burke-Gaffney; The history of medicine in the African
countries
6.
Ekeopara, Chike Augustine Ph.D1, Rev. Ugoha, Azubuike; The Contributions of African
Traditional Medicine to Nigeria�s Health Care Delivery System; Origins of
Traditional Medicine
7. WHO; Traditional and Modern Medicine: Harmonizing the Two Approaches
8. Caloriesmix; Daily Nutrition Fact
9. Thomas Nelson; A History of Medicine
10.
Microsoft� Encarta� 2009. � 1993-2008 Microsoft Corporation: Circulation of the
Blood, Physicians, Medical Ethics
11.Dr. Jenny Scutcliffe and Nanacy Duin; A History of Medcined
12.Tarik
Catic, Ivona Oborovic, Edina Redzic, Aziz Sukalo, Armin Skrbo, Izet Masic; Traditional
Chinese Medicine - an Overview
13. Ravishankar, B and Shukla, V.J.; INDIAN SYSTEMS OF MEDICINE: A
BRIEF PROFILE
14. Yogacharya Dr Ananda Balayogi Bhavanani; YOGA THERAPY: AN OVERVIEW
15.
Paolo Bellavite, Anita Conforti, Valeria Piasere and Riccardo Ortolani;
Immunology and Homeopathy. 1. Historical Background
16. Urs Ha�feli; The History of Magnetism in Medicine
17. Florida Academy; The History of Massage Therapy
18. A van Tubergen, S van der Linden; A brief history of spa therapy
19. Jaime Schultz; A History of Kinesiology
20. Abb� Mermet; Radiesthesia History
21. Roy Porter, The Cambridge Illustrated History of Medicine
22. A Brief History of Aromatherapy
23. Music Therapy in Traditional African Societies: Origin, Basis and
Application in Nigeria
24.
Dariush Moza arian and David S. Ludwig, The 2015 US Dietary Guidelines � Ending
the 35% Limit on Total Dietary Fat
25.
Peter Whoriskey of Washignton Post, The U.S. government is poised to withdraw
longstanding warnings about cholesterol - The Washington Post
26.
Dr. Robert F. Stern and Mitchell Bebel Stargrove; The History of Naturopathic
Medicine
27.
Wikipedia; Asahi Health, Thalassotherapy, Imhotep, History of Acupuncture,
Reflexology, Shiatsu, Traditional Tibetan medicine, Traditional Korean medicine,
Indian Systems of Medicine: A Brief Profile, Siddha system of medicine, Unani
system of medicine, List of forms of alternative medicine, Feng shui, Qigong,
History of Use of Traditional Herbal Medicines, Herbal Medicine, Medicinal
Plants, Origin of Traditional Medicine, Traditional Medicine, Traditional
African Medicine, Alternative Medicine, Health in Nigeria, Healthcare in
Nigeria, Siddha medicine, Crystal Healing is Metaphysics, The History of
Physical Therapy, Electrohomeopathy, The Autogenic Training Method,
Anthroposophy, Apitherapy, Bibliotherapy, Chelation therapy, Thai Massage,
Japan Kampo, Reiki, Rolfing, Biodanza, Speleotherapy, Arab medicine, Unanai
Medicine, Traditional Mongolian medicine, Herbal Medicine, Medicinal Plants,
Traditional Medicine, Alternative Medicine, Health in Nigeria, A History of
Metaphysics, Spiritual Medicine, Osteopathic Philosophy and History,
Craniosacral therapy, Origins and History of Chiropractic, Electrohomeopathy,
Bioresonance Therapy, Anthroposophic medicine, The Autogenic Training Method,
Alexander Technique Science, Apitherapy, Aquatic therapy, Chromotherapy, Energy
medicine, Feldenkrais Method, Horticultural therapy, Myofascial release,
Hydrotherapy, Numerology, Orthopathy, Radionics, Urine therapy, Wellness
(alternative medicine), A Brief History of Aromatherapy, Paraherbalism.
28. Oko Offoboche;
existence-ok.com
Forward
Most Natural Medicine
Professional Members have more than one discipline; Integrative Medicine is
more than one form of Medicine by a practitioner of Medicine: it can be
conventional (allopathic) medicine and complementary or traditional medicine.
Many Natural Medicine Practitioners have qualifications to the highest level of
scientific and arts degrees; that they know how to measure on ground in a way
that it is the exact measure in the sky or depth of the sea by understanding
gravity pressure on matter. Medicine starts from native medicine to traditional
medicine to become complementary medicine. Conventional medicine is
complementary to traditional medicine.
In Nigeria, Natural Medicine has
scientists who have reached the top of their scientific field that came
together to rescue African Traditional Medicine from extinction by allopathic
physicians who allowed western influence dissuade them from their ancestral
medicine, yet they need it more to have masters and PhD training status in
Nigeria; contrary to their activities, pharmacists because of their masters
that is pharmacognosy have aided in the development of traditional medicine. Although
it was the professors of Medicine as Federal Ministers that agreed to all in
TCAM that exists in Federal Ministry of Health in Nigeria which was because of
their training requirements. When there was Ebola (another form of Lassa fever)
in Lagos Nigeria, government physicians went on strike, private hospitals were
open and natural medicine practitioners came to the rescue. As they are
physicians with more than one form of medical background.
Most natural medicine
practitioners produce remedies, but most allopathic physicians cannot produce
drugs unlike their occidental or oriental colleagues that can produce medicinal
substances to prove the name medicine. Bachelor degree medical practitioners
are allowed to be called doctors because of continuous programme development
(CPD) that makes them resident doctors until they have a PhD to be consultants.
The purpose of this compilation
review work is not to mock the authors of the various works compiled here for
easy use by medical students and professionals, the purpose of this work is to
review the history of medicine from the point of the indigenes and/ or
practitioners of the history written by adding the spiritual insight of the
people of Africa at the time from thought forms that the conventional colonial
medicine removed the spiritual part of medicine that was part of the way of the
first practioners of science and medicine called alchemy, which is now
dispirited as chemistry etc. Nothing written by the author was altered out of
place, only those in the beginning on African had italic additions only from
the point of the dark skinned Africans at the time, but for some all parts were
not taken out, as the references on their work can only be on their work,
because they were not required for the information to be reviewed. I thank the
authors of all the works and I want them to know that I informed Copyright
Clearance Centre and sent a message to every author that required it, if not
all used here were referred to under the heading of their work and the reference
here with the pagingnation superscripted after the title of the work in
reference.
Prof. O. Offoboche
Preamble
Genesis 3:13-15 and Genesis 4:13-17
The Black Race; DNA
And Why!? u
Summary:
"The white society needs Black people believing that we came from
nothing more than slaves in order to maintain their dominance over us"!
Are you aware that DNA analysis
performed upon mummies of several Egyptian Pharaohs in 2012 by DNA-tribes, an
American based DNA analysis company, scientifically proven that the ancient
Egyptians were in fact Africans?� Carbon
date testings have also scientifically proven that the ancient kingdom was
built by Africans thousands of years long before the Arabs and Europeans
arrived theirs during the 7th century.
These scientific findings have
been suppressed from mainstream media circulation to uphold the white society�s
lies that the ancient Egyptians of Africa were ridiculously Europeans, and to
conceal the fact that Africans were living in Pyramids while Europeans were
still living in caves. White historians whitewashed ancient history to
propagate the myth of white racial superiority over Black people. The white
society needs Black people believing that our history is inferior to theirs in
order to maintain their dominance over us. The practice is known as Orwellian
propaganda. They therefore conceal the fact that Africans educated Greece�s
first scholars, and civilized Europe; this included introducing science,
mathematics, philosophy, art, agriculture and even the daily bath to Europeans.
�Those that know must teach.� -
African Proverb
In 2012 and 2013 DNA tribes, an
American company that specializes in DNA analysis, conducted testing on the
mummies of Pharaoh Tutankhamen, Ramses III, Ramses IV and several others
scientifically proven that the ancient Egyptians were in fact Africans. Their
DNA matches proved that they belonged to human Y chromosome group E1b1a. This
is the Y chromosome group of Black Sub Saharan Africans as pictured below.
Another group of mummies from the
Amarna period of Egyptian pharaohs were also tested by DNA Tribes, in 2013. The
conclusion of those testing were that those mummies autosomal profiles were
also Africans. Their DNA profiles matches the present day populations of the
African Great Lakes region and Southern Africa. Subsequent analysis of the
autosomal profile of the mummy of Pharaoh Rameses III also concluded that his
matched the genetic profiles of the population of the Great Lakes region
Africans as well. These findings were reported in the DNA Tribe�s digest on
February 2013. Carbon date testings have also scientifically proven that the
ancient kingdom was built by Africans thousands of years long before the Arabs
and Europeans arrived theirs during the 7th century. These scientific findings
have been suppressed from mainstream media circulation to uphold the white
society�s lies that the ancient Egyptians of Africa were ridiculously
Europeans, and to conceal the fact that Africans were living in Pyramids while
Europeans were still living in caves. White historians whitewashed ancient
history to propagate the myth of white racial superiority over Black people.
They conceal the fact that Africans educated Greece�s first scholars, and
civilized Europe; this included introducing science, mathematics, philosophy,
art, agriculture and even the daily bath to Europeans.
Although Egypt is located in
Africa, and all of its Pyramids, and the Great Sphinx, were built by Africans
thousands of years long before the Greeks and Arabs arrived there in the 7th
century - this has been proven by carbon dating testings- the white society
nonetheless will not acknowledge the ancient Egyptians of Africa were in fact
Africans. This isn't because they don't know. White historians are well
educated. They attend prestigious universities and are most certainly taught,
within them that all of the great monuments of Africa�s ancient Egypt were
already built, thousands of years, long before the arrivals of the Greeks and
Arabs in the 7th century. Modern Egyptians are merely descendants from Arabs
who whitened the population. In fact, the pyramids and the Sphinx were built
thousands of years long before the arrival of any non-Africans into Africa.
White historians know that the true and original Egyptians were in fact
Africans, but conceals this fact from the public. Because they�ve deliberately
stolen Africa�s glorious history of Egypt and falsely portrays it as being
theirs. The practice is known as Orwellian propaganda.
Orwellian propaganda are societal
conditions created and sustained by misinformation, distortions of facts,
denial of truth, and even the manipulation of the past to falsely exalt the
white society. White historians justifies these unethical practices as being
merely the spoils of war; thus saying that it's customary for conquerors to
distort facts and re-write history to favor themselves. However, the true
reason it�s being done is much more nefarious and self-serving of the white
society.
The true reason it�s being done
is because white social scientists theorizes that a people�s future is
predestined by the history they�re taught to believe about themselves.
According to their theory a aspiring history is necessary to acquire a aspiring
future because people references their future capabilities based upon their
past achievements. It�s the process of imparting information which best enable
people to realize their highest potential. People reference messages about
their particular group to acquire their self-images and assess their potential
and capabilities in relation to these messages. Also according to the theory,
truth is not important to inspire a people�s future, what�s only important is
what�s perceived as true. Because people function based upon their perceptions
of what�s true rather than what�s actually is. Therefore, to give their racial
group a past that inspires their future, white social scientists and white
historians whitewashed the past. More specifically, they�ve made their racial
group appear more significant throughout history than they truly were. Therefore,
the collective self-esteems of Caucasians have been falsely bolstered at the
expense of Africans.
Case Point and Proof:
Do you know that there exists
substantial proof that the Great Sphinx of Giza is a sculpted head of an Black
person?
There exist a reputable
historian's eye witness account, written testimony and an artist rendering
proving that the Great Sphinx is a sculpted head of an African Man? These are
the types of evidence that a person might take to court to win their case. However,
the system of white supremacy has always suppressed all evidence that
contradicts the myth of white superiority and falsehood of Black inferiority.
This includes hiding all evidence that the Sphinx is the sculpted head of a
Black African.
Most of us have heard the story
that when Napoleon's army arrive in Egypt on July 1 1798, he ordered that
cannons be used to deface the Negroid face of the Great Sphinx of Giza. However,
most people are not aware that there does exist substantial evidence proving that
the face of the Sphinx was in fact an African Negroid man before it was
defaced.
During the French invasion into
Egyptian Napoleon was accompanied by a French diplomat, author, archaeologist
and artist named Dominique Vivant Baron Denon.
Before the defacing of the
Sphinx, Baron Denon asked Napoleon to allow him to first draw an illustration
of the massive Sphinx of Giza before its face was destroyed. Napoleon agreed to
the request and allowed Denon to draw a picture of the Sphinx before its
defacement.�
Soon after Vivant�s sketch was
complete Napoleon ordered the nose and lips shot off the Sphinx! Napoleon's
objective for defacing the Sphinx was to remove the negro features. However,
the true features of the Sphinx survived in the Vivant Denon drawing. This
attached drawing of the Sphinx's is a true copy of that original sketch drawn
by Denon. It's given signed completion date is July 1 1798. This date affirms
that it was drawn shortly after the French invasion into Egypt. Vivant clearly
captured the facial features of the Sphinx and they are clearly Negroid as
stated by the eye witness Herodotus. The drawing shows that the Sphinx's
features were clearly that of a Negroid African before it was damaged. Seeing
the Sphinx with distinct negroid features also establishes that the ancient
Egyptians were in fact a black culture.
This drawing was later published
in the 1803 in an issue of Universal Magazine. Vivant Denon described the
Sphinx as an African woman.
Here is also the written account
about the Sphinx of Giza in Denon's own words:
��
"...Though its proportions are colossal, the outline is pure and
graceful; the expression of the head is mild, gracious, and tranquil; the
character is clearly African, but the mouth, and lips of which are thick as
most Negroes, has a softness and delicacy of execution truly admirable; it
seems real life and flesh.�� Art must
have been at a high pitch when this monument was executed; for, if the head
wants what is called style, that is the say, the straight and bold lines which
give expression to the figures under which the Greeks have designated their
deities, yet sufficient justice has been rendered to the fine simplicity and
character of nature which is displayed in this figure..."
����������� -- The Sphinx of Giza image (above)
is from the Freeman Institute Black History Collection
Vivian Denon was a well-respected
diplomat. He was appointed as the first Director of the Louvre French museum by
Napoleon after the Egyptian campaign of 1798�1801, and his drawing of the Sphinx
displaying its original Negroid features are commemorated in the Denon Wing of
the modern museum.
He also wrote in his two-volume
Voyage dans la basse et la haute Egypte ("Journey in Lower and Upper
Egypt") published in 1802, that the original Egyptians were Black skin
Negroes and that the sculpted face of the Sphinx was of the same Negro racial
type before it was defaced by Napoleon's army.
�Dominique Vivant Baron Denon
continued to insist up until his
death on 27 April 1825 that that the original face of the Sphinx was that of an
African Negro before Napoleon had it was destroyed by cannon fire. In 1787,
French orientalist Count Constantine de Volney travelled to Egypt and also
described the population as "black with woolly hair", and "true
Negroes of the same type as all native-born Africans". The reason why most
Black people are unaware that there exist a reputable eye witness account,
written testimony and an artist rendering affirming that the colossal Great
Sphinx is in fact that of a Black African is because this information has been
intentionally suppressed from the public distribution by the ruling elites.
When history's proven most
nefariously deceitful and racist group controls the information, narratives,
imageries that the world receives and perceives as true, they will naturally
always manipulate and distort facts, and even history, to favor themselves.
It's simply who they are, and the way they've always been. They have
manipulated the entire world to see thing their way through Orwellian
propaganda.
THE ORIGINAL NEFERTITI BUST IS A
PROVEN FAKE. IT WAS CREATED BY A EUROPEAN ARTIST AND USED TO PROPAGATE THE
FALSEHOOD THAT THE ANCIENT EGYPTIANS WERE EUROPEANS. THIS NEW BUST PROPAGATES
THE SAME FALSEHOOD!
The original Bust of Nefertiti,
from which this newly revealed bust is modeled after, has been proven to be an
Egyptology Fraud created by an artist commissioned by Ludwig Borchardt. It was
a deliberate attempt to make her look European.
According to a Swiss art
historian, the bust is less than 100 years old. Henri Stierlin has said the
stunning work that will later this year be the showpiece of the city's reborn
Neues Museum was created by an artist commissioned by Ludwig Borchardt, the
German archaeologist credited with digging Nefertiti out of the sands of the
ancient settlement of Amarna, 90 miles south of Cairo, in 1912.
In his book, Le Buste de
Nefertiti � une Imposture de l'Egyptologie? (The Bust of Nefertiti � an
Egyptology Fraud?), Stierlin has claimed that the bust was created to test
ancient pigments. But after it was admired by a Prussian prince, Johann Georg,
who was beguiled by Nefertiti's beauty, Borchardt, said Stierlin, "didn't
have the nerve to make his guest look stupid" and pretended it was
genuine.
Berlin author and historian
Edrogan Ercivan has added his weight to the row with his book Missing Link in
Archaeology, published last week, in which he has also called Nefertiti a fake,
modelled by an artist on Borchardt's statuesque wife.
Public and political enthusiasm
about the find at the time gave the artefact its "own dynamic" and
led to Borchardt ensuring it was kept out of the public gaze until 1924, the
authors have argued.
He kept it in his living room for
the next 11 years before handing it over to a Berlin museum, since when it has
been one of the city's main tourist attractions.
The statue was famously admired
by Adolf Hitler, who referred to it as "a unique masterpiece, an ornament,
a true treasure".
THE NEFERTITI BUST IS FAKE
The archaeologist who claimed to
have found the bust was actually going to reproduce a new sculptor of the Queen
wearing a necklace he knew she had owned. He was also experimenting with colour
tests with ancient pigments found at the digs. After completing the bust in
1912, the copy was admired so much by a German Prince; the Archaeologist
couldn't sum up the courage to tell the Prince it was a fake.
THE SCIENTIFIC COMMUNITY KNEW
THERE WERE HUGE ANOMALIES WITH THE BUST
'�The bust has no left eye and
was never crafted to have one. This is an insult for an ancient Egyptian who
believed the statue was the person themselves..." He also said the
shoulders were cut vertically in the style practised since the 19th century
while, "Egyptians cut shoulders horizontally" and that the features
were accentuated in a manner recalling that of Art Nouveau. It was impossible
to scientifically establish the date of the bust because it was made of stone
covered in plaster, he said. "..The pigments, which can be dated, are
really ancient.." he added.
ARCHAEOLOGIST AT THE TIME NEVER
MENTIONED THE FIND AT THE SITE - IT WAS NEVER LISTED UNTIL 11 YEARS AFTER THE
APPARENT DISCOVERY - THE ARCHAEOLOGIST DIDN'T EVEN SUPPLY A DESCRIPTION
Stierlin also listed problems he
noted during the discovery and shipment to Germany as well as in scientific
reports of the time. French Archaeologists present at the site never mentioned
the finding and neither did written accounts of the digs. The earliest detailed
scientific report appeared in 1923, 11 years after the discovery. The
archaeologist "..didn't even bother to supply a description, which is
amazing for an exceptional work found intact..". Borchardt 'knew it was a
fake', Stierlin said. "..He left the piece for 10 years in his sponsor's
sitting-room. It's as if he'd left Tutankhamen's mask in his own
sitting-room.." .
Apart from anything else, the
bust looks nothing like the 'real' Nefertiti images, it's as if someone has
attempted to make her look European. The other pictured artifacts are true
authenticated images of Nefertiti showing she's Black.
There is a relief depicting of
Nefertiti that is carved from Limestone displaying her with prominent African
features. It's kept at the Ashmolean Museum, Oxford
Archeologists also found a
statute of the body of Queen Nefertiti from the Kingdom, Dynasty, reign of
Amenophis IV-Akhenaten, BC Quartzite. The body of Nefertiti has a body shape
that is clearly an Africans. It's kept at the Louvre Museum | Paris
There's also many more carvings
and paintings depicting Nefertiti with her husband and children that are also
all depicted as Africans. We've been bamboozled by whites. They've stolen our
ancient African history and portrays it as theirs.
The white society sits upon a
throne of white exalting lies created and sustained by Orwellian propaganda.
Case, Point, and Proof:
The white society teaches us that
the world�s first scholars were the Greeks and that it was they that civilized
the world. However, all of Europe�s Greek scholars received their formal
education in Africa�s ancient Egypt. The Greeks openly admitted that their
knowledge originated from Africa. When Isocrates wrote of his studies in the
book Busirus, he said that �I studied philosophy and medicine in Africa�s
Egypt.�
The white society teaches us that
the father of medicine was a Greek named Hippocrates. However, the true father
of medicine was an African named Imhotep. Imhotep was practicing medicine and
writing on the subject 2,200 years before Hippocrates, the so called father of
modern medicine, was even born. Imhotep is the author of an Egyptian medical
text written on Papyrus, which contains almost 100 anatomical terms and
describes 48 injuries and their treatment.
The history we�ve been taught
also distorts many facts in order to give themselves credit for most inventions
made by Black people.
Case Point and Proof:
White historians teach us that
Thomas Edison is responsible for lighting up the world. But here are the facts
to the contrary:
Thomas Edison and Lewis Latimer
were both each simultaneously working on inventing their lightbulbs. Edison
merely rushed to have his lightbulb patented first. However once Edison
patented his lightbulb, NO companies purchased, nor mass produced it. Because
it was deemed not efficient enough. It light very dimly and only lasted a few
minutes. When Lewis Latimer patented his lightbulb it was deemed significantly
more proficient, therefore it was purchased and mass produced. Lewis Latimer
was also dispatched around the world to oversee the installations of his
lightbulbs. Therefore, it was in fact Lewis Latimer that actually lit up the
entire world. But because Latimer was Black, our racist whitewashed history
books falsely claims that it was Edison that light up the world.
White historians also teach us
that Henry Ford invented the first automobile. It was actually a African
American inventor and carriage company entrepreneur named Charles Richard
Patterson that built the first automobile. The C.R Patterson & son�s company
starting out as a carriage building firm in 1873. In the early 1900�s Patterson
and his son converted the company from a carriage business to a automobile
manufacturer. It was released in 1905 and sold for $850. It had a four-cylinder
Continental engine. C.R Patterson began making automobiles before Henry Ford
and his automobiles were considered more sophisticated. C.R. Patterson and Sons
were forced out of business by Henry Ford. In 1939, the company closed its big
wooden doors.
But because Paterson was Black,
our racist whitewashed history books falsely claims that it was Ford that
invented the first automobile.
The hidden reality is that in
spite of cultural traumas wrought by the injustices of white racism and slavery
most inventions that have revolutionized the world were in fact either invented
by a Black person, or were inspired by an earlier invention by a Black person.
It�s actually the genius minds of Black people that moves the entire world
forward.
�When a well-packaged web of lies
has been sold gradually to the masses over generations, the truth will seem
utterly preposterous and its speaker a raving lunatic.� -Dresden James.
I know that for some of you that
declaration may be a hard pill to swallow, given how negatively Black people
are depicted within the white society. We are constantly portrayed as the
Blacks leeches of white society that benefits from the genius of white minds.
However, the reality is the exact opposite from what the white society has
manipulated so many to believe.
Here�s a relevant fact that they
exclude from their whitewashed history books:
After slavery was abolished in
the U.S. in 1865, beginning from 1870 and 1940, African Americans filed 726
invention patents. For a people to go directly from being enslaved - were they
were denied an education - to then producing so much inventions in such a short
time span is astounding. Furthermore, those numbers of patent applications
submitted by African Americans more than doubled those submitted by whites
during the same time frame. Even while being enslaved many Africans invented
many things, but the patent rights were awarded to their white slave owners.
As stated earlier: Most
inventions that have revolutionized the world were in fact either invented by a
Black person, or were inspired by an earlier invention by a Black person.
Case, Point, and Proof:
If you enjoy using the internet
thank
Philip Emeagwali, a Nigerian
computer scientist, is regarded by many as being the father of the Internet. He
invented the super computer in 1987. It was his formula that used 65,000
separate computer processors to perform 3.1 billion calculations per second in
1989. That feat led to computer scientists comprehending the capabilities of
supercomputers and the practical applications of creating a system that allowed
multiple computers to communicate. Philip Emeagwali also invented the accurate
weather forecasting system in 1990. He also used his mathematical and computer
expertise to develop methods for extracting more petroleum from oil fields.
If you enjoy sending emails thank
a African American name Emmit McHenry. McHenry created a complex computer code
whereby ordinary people can now surf the web or have e-mails without studying
computer science. He created what we know today simply as .com.
If you enjoy your digital
cellphone thank an African American name Jesse Eugene Russell.� He is an inventor and electrical engineer
that invented digital cellular technology. He pioneered the field of digital
cellular communication in the 1980s through the use of high power linear
amplification and low bit rate voice encoding technologies and received a
patent in 1992 (US patent #5,084,869) for digital cellular base station design.
Jesse Russell holds several patents and is a key person to the invention of the
modern cell phone.
�
If you enjoy using your PC monitor thank an African American named Dr.
Mark Dean. Dean is the Inventor/Computer scientist and engineer responsible for
developing a number of landmark technologies, including the modern color PC
monitor, the Industry Standard in 1981. In 1999, Dean also led a team of
programmers to develop one of the stepping stones of modern day computer
technology� the first gigahertz chip. The CMOS microprocessor chip is
remarkable because it processed a billion calculations and large amounts of
data in a second. Dean hold 20 individual patents.
If you enjoy using your GPS thank
Gladys Mae West - an African American mathematician known for her contributions
to the mathematical modeling of the shape of the Earth, and her work on the
development of the satellite geodesy models that were eventually incorporated
into the Global Positioning System (GPS).
Without Black people there would
not exist skyscrapers. This is because Black people invented the elevator, the
air conditioning, and central heating. Alexander Miles invented the Elevator,
Fredrick Jones invented the air condition, and Alice Parker, a Black woman,
invented the heating furnace in 1919 which provided central heating.
Dr. Thomas O. Mensah is a Ghanaian
born chemical engineer and inventor. Is the inventor of fiber optics and
nanotechnology. He was awarded 7 USA and worldwide patents in fiber optics. In
all, he has some 14 patents.
Dr. Patricia Bath, an African
American scientist invented, and patented in 1988 the cataract laserphaco probe
that help save the eye sight of millions. Millions of people around the world
unknowingly owes their eyes sight to this Black woman.
Mark Hannah developed the 3D
graphics technology that now used in many major Hollywood movies
Shirley Ann Jackson made several
telecommunications breakthroughs which led to the touch-tone phone, caller I.D.
and call waiting.
Marie Van Brittan Brown invented
the home surveillance security system.
Henry Sampson invented the non-digital
cellular phone in 1983.
Did you know that the Sanitary
Pad was developed by a Black woman name Mary Beatrice Davidson. Until sanitary
pads were created, women used all kinds of reusable fabrics to absorb menstrual
flows.
Mary's invention was initially
rejected. The first company that showed interest rejected it because of racial
discrimination. The world had no choice, her invention was too important to be
ignored. It was later accepted in 1956, 30 years later. She received five
patents for her inventions. One of her other inventions is the bathroom tissue
holder, which she co-invented with her sister. The patent number was US
4354643.
There is more:
Gerald A Lawson invented the
first home video game system with inter changeable cartridges.
Percy L. Julian invented the
process of synthesis which led to the birth control pill and improvement in
cortisone production.
There is more:
Matthew A. Cherry, is the
inventor of the tricycle. In May 1888, Cherry received his patent for the
tricycle.
G.T. Sampson invented the clothes
drier in 1892.
George R. Carruthers invented the
ultra-violent camera spectrograph�
In1885, two Black inventors, L S.
Burridge and N.R. Marsham, invented the typewriter
J. Gregory invented the motor
Six African Americans scientists
were essential in the making of the first atomic bomb. One was J. Ernest
Wilkins, one of the world�s leading mathematicians who earned his PhD at the
age of seventeen.
Alexander Miles invented the
Elevator and safety devices for elevator.
Patent no 371,207
Alice Parker, a Black woman, is
credited with inventing the heating furnace in 1919 which provided central
heating.
Garret A. Morgan invented the
automatic traffic signal and the gas mask.
Edmond Berger invented the spark
plug.
J.B. Winters invented the fire
escape ladder.
John L. Love invented the Pencil
sharpener 23- 11-189 Patent # 594114.
Fredrick Jones invented the air
conditioner.
John A. Johnson invented the
wrench
John Standard invented the
refrigerator
Lewis Howard Latimer invented the
electric lamp and the filament for the light bulbs.
The small Pox Inoculation method
was brought from Africa by African named Onesimus
Phillip Downing invented the
letter drop mail box 10-27-1892
John Burr invented the Lawn mower
Marjorie Joyner holds the patent
for the permanent hair wave machine.
Lloyd Hall created the chemical
compound that preserves meat
S.H. Love invented improvements
to military guns 22-4-1919
S.H. Love invented improvements
to the vending machine 1-21-1933��
�W.A. Lovette invented the advanced printing
press
Thomas J. Martin invented the
fire extinguisher 3-261872
W.D. Davis invented the riding
saddle 10-6-1895
There is more:
Do you know that the first
successful open heart surgery on this planet was performed by a Black surgeon within
a Black owned Hospital?
Dr. Daniel Hale Williams
(1856-1931) founded Provident
Hospital and Training School for Nurses (the first black-owned hospital in
America) in 1891.
And he performed the first
successful open heart surgery in 1893. Following the surgery white surgeons
from around the country and the world came to learn from Dr Williams. Many
white surgeon had attempted the surgery early but their patients died.
In 1940, Dr. Charles Drew,
another African American doctor achieved yet another medical pioneering break
through. In his short life of only 46 years, Charles revolutionized blood
storage. His refrigerated �blood mobiles� stored blood at a temperature to
prolong its shelf life. This further revolutionized blood storage and plasma
banks for WWII.
WHILE INSPIRING THEIR RACIAL
GROUP THEY DO THE OPPOSITE TO BLACK PEOPLE BY TEACHING US THAT AFRICANS WERE
UNCIVILIZED AND ILLITERATE BEFORE THE EUROPEANS INVADED, AND THEREFORE HAS NO
SIGNIFICANT HISTORY:
But here are the facts to the
contrary:
The first being that the world�s
oldest university is located in Africa.
Timbuktu University:
The Timbuktu University (in Mali,
Africa) and its library are older than any of those found within the Western
world. It was composed of three schools, namely the Masajid of Djinguereber,
the Masajid of Sidi Yahya, and the Masajid of Sankore. During the 12th century,
the university had an enrollment of around 25,000 students from Africa. In
Timbuktu, there are about 700,000 surviving books. They are written in Mande,
Suqi, Fulani, Timbuctu, and Sudani. The contents of the manuscripts include
math, medicine, poetry, law and astronomy. This work was the first encyclopedia
in the 14th century before the Europeans got the idea later in the 18th
century, 4 centuries later.
Furthermore, long before the
Europeans invaded Africa, it was Africans- when we called ourselves Moors -
that civilized Europe. This included introducing science, math, philosophy, and
even the daily bath to Europeans.� Queen
Isabella of Spain bragged that she had only bathed twice in her whole life.
Queen Elizabeth I, claimed that she was the cleanest woman in all of Europe,
for reportedly bathing once a month.
There�s More:
Africa is also the cradle of
mathematics.
The world�s oldest mathematical
tools were discovered in Africa.
The Ishango Mathematic Tool.
The Ishango Mathematical Tool was
invented by Africans dating as far back as 22000 years ago, in the Upper
Paleolithic era. The Ishango tool is an attestation of the practice of
arithmetic in ancient Africa.
There was also discovered in
Africa another mathematical tool.
The Lebombo Mathematical Tool.
The Lebombo Tool is indeed the
oldest known mathematical artifact in the world. It is even older than the
Ishango bone. Discovered in the 1970s in Border Cave, a rock shelter on the
western scarp of the Lebombo Mountains in an area near the border of South
Africa and Swaziland (now Eswatini).
Great Zimbabwe:
Great Zimbabwe is an ancient city
in the south-eastern hills of Zimbabwe near Lake Mutirikwe and the town of
Masvingo - originally called the Shona civilization. The stone city spans an
area of 7.22 square kilometres (2.79 square miles) which, at its peak, could
have housed up to 18,000 people.
These gigantic brick buildings
and walls were erected nearly 2000 years ago. It is recognized as a World
Heritage site by UNESCO.
The world�s largest man made
structure was built by Africans:
There exist in Africa within the
ancient Nigerian city of Benin the ruins of a Great Wall four time larger than
the Great Wall of China.
The Great Wall of Benin in Edo
state Nigeria was the largest man made structure in the history of the world.
The walls are four times longer than the Great Wall of China and consumed 100
times more materials than the pyramid of Giza. The walls extended for some
16,000 kilometers in all and covered a space of 6,500 square miles. It is
estimated that it took over 150 million hours of digging to construct and were
all built by the Edo people.
In all, they are four times
longer than the Great Wall of China, and consumed a hundred times more material
than the Great Pyramid of Cheops. It�s perhaps the largest single
archaeological phenomenon on the planet.� Source: Wikipedia, Architecture of
Africa.� Fred Pearce the New Scientist 11/09/99.
Even before the full extent of
the city walling had become apparent the Guinness Book of Records carried an
entry in the 1974 edition that described the city as: �The largest earthworks
in the world carried out prior to the mechanical era.� � Excerpt from �The
Invisible Empire�, PD Lawton, African Historical Ruins.
Sadly, in 1897, Benin City and
its Great Wall was destroyed by British forces under Admiral Harry Rawson - in
what has come to be called the Punitive expedition. The city was looted, blown
up and burnt to the ground. This expedition destroyed about 1,100 years of
Benin history and one of the evidence of African civilization. The
expeditionary force was made up of 1,200 British soldiers.
It brought an end to the great
Benin Kingdom and led to the looting numerous Benin historical artefacts. A
collection of the famous Benin Bronzes are now in the British Museum in London.
Part of the 700 stolen bronzes by the British troops were sold back to Nigeria
in 1972.
The monumental building
achievements of Africa�s ancient Egyptians also proves that Africans were not
illiterate nor uncivilized.
All that we learn from the
oppressors are lies that falsely exalts themselves and falsely marginalizes us.
The collective self-esteems of the white masses have been falsely bolstered at
the expense of the collective self-esteems of the Black masses.
The white educational system�s
failure to adequately provide Black students with a racially affirming
curriculum as it routinely does for White students is actually essential for
maintaining white dominance. Because for a ruling class to maintain its
position of social dominance over its oppressed population, they must condition
the oppressed from a very early age to accept their own subordinate status and
to adhere to the authority of the dominant society.
To do so, the education given to
the oppressed, from the time that their minds are young and most
impressionable, must be the type that denies them of a racially and culturally
affirming curriculum. When the oppressed population is denied a fully racially
and culturally affirming education, even the brightest among them may have
little, if any, hope of mentally extracting themselves from their assigned low,
dominated position in life.
Dr. B. L. Dickson
Metaphysics/ Spirituality
Contents������������������������������������������������������������������������������������������������������������������� � �����
Abstract
Author/s
(Reviewer)...........................................................................................................................................................................
Forward................................................................................................................................................................................................
Preamble...........................................................................................................................................................................................
Content............................................................................................................................................................................................
1.0
History of
Medicine..............................................................................................................................................................
������� 1.1.0
Learning
Objectives...........................................................................................................................................................
������� 1.1.0.1
List of forms
of alternative medicine....................................................................................................................
������� 1.1.0.2
Introduction...............................................................................................................................................................
������� 1.1.0.3
Post Colonial
Medicine error..................................................................................................................................
1.2.0
Medicine in
Africa
...............................................................................................................................................................
������� 1.2.0.1
Eden............................................................................................................................................................................
������� 1.2.0.2
Egypt.................................................................................................................................................................................
������� 1.2.0.3
Imhotep......................................................................................................................................................................
������� 1.2.0.4
Colonial
Medicine Influence...................................................................................................................................
1.2.1
Mesopotamian...........................................................................................................................................................................
1.2.2
Israeli/ Palestinian.....................................................................................................................................................................
������� 1.2.2.1
Thalassotherapy..............................................................................................................................................................
1.2.3
Chinese Medicine..............................................................................................................................................................
������� 1.2.3.1
Traditional
Chinese Medicine - an Overview.......................................................................................................
������� 1.2.3.2
History of
Acupuncture...........................................................................................................................................
������� 1.2.3.3
Feng shui....................................................................................................................................................................
������� 1.2.3.4
Qigong......................................................................................................................................................................
������� 1.2.3.5
Reflexology............................................................................................................................................................
������� 1.2.3.6
Shiatsu....................................................................................................................................................................
1.2.4
Traditional
Tibetan medicine........................................................................................................................................
1.2.5
Traditional
Korean medicine.........................................................................................................................................
1.2.6
Indian Medicine...............................................................................................................................................................
������� 1.2.6.1
Indian Systems of
Medicine: A Brief Profile....................................................................................................
������� 1.2.6.2
Siddha system of
medicine................................................................................................................................
������� 1.2.6.3
Unani system of
medicine..................................................................................................................................
������� 1.2.6.4
Yoga Therapy: An Overview...............................................................................................................................
������� 1.2.6.5
Siddha medicine...................................................................................................................................................
1.2.7
Thai Massage...................................................................................................................................................................
1.2.8
Japan Kampo....................................................................................................................................................................
������� 1.2.8.1
Reiki........................................................................................................................................................................
1.2.9
Rolfing...............................................................................................................................................................................
1.2.10
Greco-Roman
Medicine...............................................................................................................................................
������� 1.2.10.1
Asahi Health........................................................................................................................................................
������� 1.2.10.2
Biodanza......................................................................................................................................................................
������� 1.2.10.3
Speleotherapy....................................................................................................................................................
1.2.10.1
Dark Ages....................................................................................................................................................................
1.2.10.2
Arab medicine
...........................................................................................................................................................
������� 1.2.10.2.1
Unanai Medicine
...........................................................................................................................................
1.2.10.3.1
Medieval
European medicine
.............................................................................................................................
1.2.10.3.2
Traditional
Mongolian medicine.........................................................................................................................
1.3.0
The Renaissance..............................................................................................................................................................
������� 1.3.1
Circulation of the Blood.........................................................................................................................................
������� 1.3.2
Jenner and vaccination...........................................................................................................................................
������� 1.3.3
The discovery of
anaesthesia
...............................................................................................................................
������� 1.3.4
The Germ Theory
of Disease.................................................................................................................................
������� 1.3.5
Antiseptics................................................................................................................................................................
������� 1.3.6
Antibiotics.................................................................................................................................................................
������� 1.3.7
Medical Statistics.....................................................................................................................................................
������� 1.3.8
Diagnostic
Technology...........................................................................................................................................
������� 1.3.9
Modern Surgery.......................................................................................................................................................
2.0
Analysis of
the order of discovery in the history of medicine
...................................................................................
2.1 ��The
Origins & History of Medical Practice & Fundamentals of Medical Practice
Management................
������� 2.2 ��History
of Use of Traditional Herbal Medicines .................................................................................................
������� 2.3 ��Herbal Medicine.......................................................................................................................................................
������� 2.4 ���Paraherbal Medicine...............................................................................................................................................
������� 2.5 ���Medicinal Plants.......................................................................................................................................................
������� 2.6 ���Origin of Traditional Medicine
.............................................................................................................................
������� 2.7 ���Contributions
of Traditional Medicine to Healthcare Development ............................................................
������� 2.8 ���Traditional Medicine...............................................................................................................................................
������� 2.8.1
Traditional
African Medicine.................................................................................................................................
������� 2.9 ���Traditional and Modern Medicine: harmonizing
the two approaches(Summary)......................................
3.0
Alternative
Medicine.........................................................................................................................................................
������� 3.1
Health in Nigeria.........................................................................................................................................................
������� 3.2
Healthcare in Nigeria.................................................................................................................................................
4.0
Traditional
and Modern Medicine: harmonizing the two approaches(Meeting)...................................................
������� 4.1 ���A History of Metaphysics.......................................................................................................................................
������� 4.1.1
Spiritual Medicine...................................................................................................................................................
������� 4.1.2
Crystal
Healing is a Metaphysics Diploma course......................................................................................................
������� 4.2 ��The History of Naturopathic Medicine.................................................................................................................
������� 4.3 ��The history of Naprapathy..............................................................................................................................................
������� 4.4 ��The History of Physical Therapy.............................................................................................................................
������� 4.5 ��Osteopathic Philosophy and History.....................................................................................................................
������� 4.6 ��Craniosacral therapy................................................................................................................................................
������� 4.7 ��Origins and History of Chiropractic.......................................................................................................................
������� 4.8 ��Immunology and Homeopathy..............................................................................................................................
������� 4.9 ��Electrohomeopathy..................................................................................................................................................
������� 4.10
The History
of Magnetism in Medicine................................................................................................................
������� 4.11
A Brief History of Aromatherapy...........................................................................................................................
������� 4.12
The History of
Massage Therapy...........................................................................................................................
������� 4.13
A brief history
of spa therapy.................................................................................................................................
������� 4.14
A History of Kinesiology..........................................................................................................................................
������� 4.15
Radiesthesia
History................................................................................................................................................
������� 4.16
Bioresonance
Therapy.............................................................................................................................................
������� 4.17
Anthroposophic
medicine.......................................................................................................................................
������� 4.18
The Autogenic
Training Method..........................................................................................................................
������� 4.19
A
Historical Look at Rudolf Steiner, Anthroposophy, and Waldorf Education..............................................
������� 4.20
Music
Therapy in Traditional African Societies.............................................................................................
������� 4.21
Alexander
Technique Science................................................................................................................................
������� 4.22
Apitherapy.................................................................................................................................................................
������� 4.23
Aquatic therapy........................................................................................................................................................
������� 4.24
Bibliotherapy.............................................................................................................................................................
������� 4.25
Chelation therapy.....................................................................................................................................................
������� 4.26
Chromotherapy.........................................................................................................................................................
������� 4.27
Energy medicine.......................................................................................................................................................
������� 4.28
Feldenkrais Method.................................................................................................................................................
������� 4.29
Horticultural
therapy...............................................................................................................................................
������� 4.30
Hydrotherapy............................................................................................................................................................
������� 4.31
Myofascial release....................................................................................................................................................
������� 4.32
Numerology...............................................................................................................................................................
������� 4.33
Orthopathy................................................................................................................................................................
������� 4.34
Radionics....................................................................................................................................................................
������� 4.35
Urine therapy............................................................................................................................................................
������� 4.36
Wellness (alternative medicine)............................................................................................................................
������� 4.37
History of Reflexology.............................................................................................................................................
5.0
History of
Natural Medicine
............................................................................................................................................
6.0
Physicians.............................................................................................................................................................................
������� 6.1
Clinical Trials........................................................................................................................................................................
������� 6.2
Medical Ethics.............................................................................................................................................................
7.0
References...........................................................................................................................................................................
�������
Art of reviewer
1.0 History of
Medicine z
Medicine (Latin medicus, �physician�), the science and art of
diagnosing, treating, and preventing disease and injury. c
Natural Medicine begins after paradise, when good and evil began. But
to understand why natural medicine is of nature, we have to go all the way to
when paradise began that caused creation; which allowed the immunity of
humanity to weaken because of carnal living instead of spiritual living that
came because the way to life (that is spirit) was cut off after the fall of the
first man to attain spiritual completion. This made man prone to diseases.� The Universe has viruses that are formed by
the reaction of particles in space that falls into our atmosphere around
800,000,000 (eight hundred million) a day, in which plants that are always
outside make direct contact with them and the most effective plant amongst them
to overcome anyone of them is the very plant used to treat the sick.
1.1.0 Learning Objectives d:
➤
Appreciate natural medicine and medical practice history.
➤
Explore the domains of natural medicine and medical practice management.
➤
Understand the natural forces of change affecting natural medicine practice.
➤
Develop natural perception on changes affecting natural medical practice.
➤
Comprehend the significance of the natural medical practitioner.
1.1.0.1 List of forms of alternative medicine w (although WHO has dropped alternative, it is used because
of the author)
Some with history and origin in the list of articles
covering alternative medicine topics are used.
A
Activated
charcoal cleanse
Acupressure
Acupuncture
Affirmative
prayer
Alexander
technique
Alternative
cancer treatments
Animal-Assisted
Therapy
Anthroposophical
medicine
Apitherapy
Applied
kinesiology
Aquatherapy
Aromatherapy
Art Therapy
Asahi Health
Astrology
Attachment
therapy
Auriculotherapy
Autogenic
training
Autosuggestion
Ayurveda
B
Bach flower
therapy
Balneotherapy
Bates method
Bibliotherapy
Biodanza
Bioresonance
therapy
Blood
irradiation therapies
Body-based
manipulative therapies
Body work
(alternative medicine) or Massage therapy
C
Chelation
therapy
Chinese food
therapy
Chinese
herbology
Chinese
martial arts
Chinese
medicine
Chinese pulse
diagnosis
Chakra
Chiropractic
Chromotherapy
(color therapy, colorpuncture)
Cinema
therapy
Coding
(therapy)
Coin rubbing
Colloidal
silver therapy
Colon
cleansing
Colon
hydrotherapy (Enema)
Craniosacral
therapy
Creative
visualization
Crystal
healing
Cupping
D
Dance therapy
Detoxification
Detoxification
foot baths
Dietary
supplements
Dowsing
E
Ear candling
Earthing
Eclectic
medicine
Electromagnetic
therapy
Electrohomeopathy
Equine-assisted
therapy
Energy
medicine
��������������� Magnet therapy
��������������� Reiki
��������������� Qigong
��������������� Shiatsu
��������������� Therapeutic touch
��������������� Energy psychology
F
Faith healing
Fasting
Feldenkrais
Method
Feng shui
Five elements
Flower
essence therapy
Functional
medicine
G
German New
Medicine
Grahamism
Grinberg
Method
Gua sha
Graphology
H
Hair analysis
(alternative medicine)
Hatha yoga
Havening
Hawaiian
massage
Herbalism
��������������� Herbal therapy
��������������� Herbology
Hijama
Holistic
living
Holistic
medicine
Homeopathy
Home remedies
Horticultural
therapy
Hydrotherapy
Hypnosis
Hypnotherapy
I
Introspection
rundown
Iridology
Isolation
tank
Isopathy
J
Jilly Juice
L
Laughter
therapy
Light therapy
M
Macrobiotic
lifestyle
Magnetic
healing
Manipulative
therapy
Manual
lymphatic drainage
Martial arts
Massage
therapy
Massage
Medical
intuition
Meditation
��������������� Mindfulness meditation
��������������� Transcendental meditation
��������������� Vipassana
Meridian
(Chinese medicine)
Mega-vitamin
therapy
Mind�body
intervention
��������������� Alexander technique
��������������� Aromatherapy
��������������� Autogenic training
��������������� Autosuggestion
��������������� Bach flower therapy
��������������� Feldenkrais method
��������������� Hatha yoga
��������������� Hypnotherapy
Moxibustion
Myofascial
release
N
Naprapathy
Natural
Health
Natural
therapies
Naturopathic
medicine
New thought
Neuro-linguistic
programming
Nutritional
healing
Nutritional
supplements
Numerology
O
Orthopathy
Osteopathy
P
Pilates
Postural Integration
Pranic
healing
Prayer
Psychic
surgery
Prokarin
Paula method
healing exercises
Q
Qi
Qigong
Quantum
healing
R
Radionics
Rebirthing
Recreational
Therapy
Reflexology
Reiki
Rolfing
Structural Integration
Rosen Method
S
Salt Therapy
Self-hypnosis
Shiatsu
Siddha
medicine
Sonopuncture
Sound therapy
Spiritual
mind treatment
Structural
Integration
Support
groups
T
T'ai chi
ch'uan
Tantra
massage
Tao yin
Thai massage
Thalassotherapy
Therapeutic
horseback riding
Therapeutic
touch
Tibetan eye
chart
Traditional
Chinese medicine
History of
traditional Chinese medicine
Traditional
Korean medicine
Traditional
Japanese medicine
Traditional
Mongolian medicine
Traditional
Tibetan medicine
Trager
approach
Transcendental
meditation
Trigger point
Tui na
U
Unani
medicine
Urine therapy
Uropathy
V
Vaginal
steaming
Vegetotherapy
Visualization
(cam)
Visualization
W
Water cure
(therapy)
Wellness
(alternative medicine)
Wuxing
(Chinese philosophy)
Y
Yoga
��������������� Ashtanga yoga
��������������� Amrit yoga
��������������� Ashtanga vinyasa yoga
��������������� Bikram yoga
��������������� Hatha yoga
��������������� Iyengar yoga
��������������� Kundalini yoga
��������������� Siddha yoga
��������������� Sivananda yoga
��������������� Tantric yoga
��������������� Viniyoga
��������������� Vinyasa yoga
��������������� Yoga Therapy
��������������� Daoyin Taoist Yoga
Z
Zang fu
(back to content)
1.1.0.2
Introduction m
Illness and injury are as old as fallen humankind. Though, true humanity should normally not be measured by human
remains but by artifact, because human
beings were not dying until humankind�s fall; Stone Age human remains show
evidence of diseases such as arthritis, tuberculosis, inflammations, dental
problems, leprosy bone tumours, scurvy, spinal tuberculosis, cleft spine,
osteomyelitis, sinusitis and various congenital abnormalities and injuries.
These illnesses show in human skeletal remains and if more complete human
remains were available, it is likely a much greater span of diseases would be
apparent. Agreed that human beings do not like pain, death and suffering there
was a clear need to try and find a cure for diseases and injuries.
The curing and prevention of
disease usually involves an explanation of the cause of the disease. In the
absence of knowledge of germs (bacteria and viruses) and of human anatomy and
physiology stone age humans ascribed disease, injuries and death to
supernatural forces, just as other inexplicable events such as storms,
earthquakes and volcanic eruptions were considered to be caused by supernatural
forces. This lead to the need for a method of influencing the supernatural
forces which required a person with knowledge of the supernatural world who
could communicate with and placate the gods or spirits that caused the disease
and injury. Priests, shamans, witch doctors and medicine men were often
responsible for protecting the health of Stone Age humans by means of appropriate
rituals and spells. A cave painting of what is considered to be a Stone Age
medicine man dating from around 15,000 BCE is on the cave walls of the Les Trois Freres cave in the Pyrenees.
 d
d
Stone Age medicine men would most
likely have supplemented their spells and rituals with the use of various
herbs, roots, leaves and animal parts and other medicines. Given the body�s
natural tendency to heal itself and placebo effects, to the non-spiritual they will think it would have been difficult
for pre-historic healers to work out whether their spells and herbs were
actually working, but in truth, by their
spirit they knew. Colonial medicine taught that only in recent times with
modern written records, statistical techniques and double blind studies
involving control groups, can it be reasonably clear if a particular medicine
is working.
The earliest clear example of a
surgical operation is trepanning which involves boring a hole into the skull.
This operation was first carried out in Neolithic times using stone tools. Some
of the patients survived as shown by healing around the holes and some skulls
even had several holes bored in them, indicating repeated operations. It is not
clear why such a painful operation was carried out, but it may have been to
allow evil spirits that were causing migraines, epilepsy or madness to escape
from the patient�s skull. It is also likely other surgical operations, such as
the lancing of abscesses and the sewing up of wounds with bone or flint
needles, were performed, but there is no clear evidence of this.
�
��


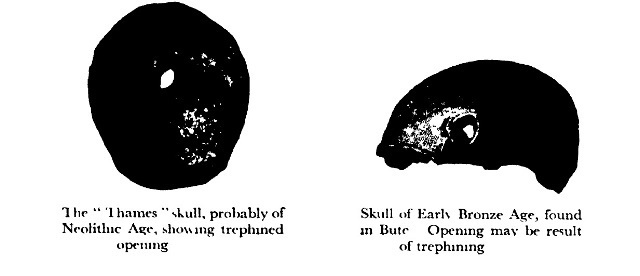
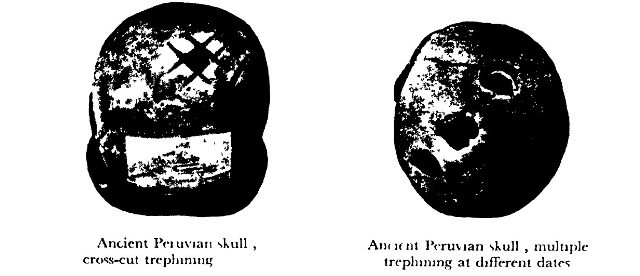 b
b
 c
c
Trepanned Skull C
Trepanning, the procedure of cutting a
hole in the skull, is the earliest known medical operation. Some
anthropologists believe that trepanning was performed on people with mental
illnesses to drive out evil spirits from their heads. This skull dates from the
Inca civilization.
Daniele
Pellegrini/Photo Researchers, Inc.
When nomadic hunter-gatherers
first began to settle in permanent villages, which grew into towns and then
cities, new health problems arose. Large numbers of people concentrated in
small areas meant disease would quickly spread through populations.� The domestication of animals resulted in many
diseases spreading from animals to humans such as measles, smallpox and
tuberculosis from cattle and flu from pigs and dogs. However, a further result
from living in cities was the development of writing which allowed a more
organized medical profession and the possibility of accurate recording of
symptoms and remedies.
Writing began in Mesopotamia
before 3,000 BCE when it was invented by the ancient Sumerians. The Sumerians
wrote on clay tablets and one such tablet contains lists of drugs, chemical
substances and plants used for medical purposes. Magic and religion however
played a major role in Mesopotamian medicine as injury and disease were
considered to be caused by gods, demons, evil spirits and witchcraft. Numerous
magic spells, incantations and sacrifices were available to combat particular
diseases and correct recitation was necessary for an effective cure. Whether a
patient would survive or not could be divined by examining the liver of a
sacrificed sheep or goat. The Code of Hammurabi, a law code made by a
Babylonian King, sets out medical fees for various services and penalties for
errors made by the doctor. Services referred to involved, the opening of an
abscess, the treatment of broken limbs, eyes and intestinal complaints.
(back
to content)
1.1.0.3 Post-Colonial Medicine Error
They also made mistakes with a
lot of fatalities with their industrialization, but such mistakes are not put
in simple history, but only when you choose to study more. But for medicines in
Africa, they stigmatized them in history, forgetting that you do not insult the
place of your fore father's that your ancestors migrated from, because it
backfires. It is not true that post-colonial medicine is the best medication,
because nature that is original, produces the best medicine that complements
the harm of the treatment that synthetic medicine does not do.
Modern medicine or better put, post-colonial
medicine (because the medical practices was for their economic colonization of
the minds of other races), also made terrible mistakes that were not physically
done on the scull but were physically done on the body of the person by their
dietary guidelines mistakes:
The U.S. government is poised to withdraw longstanding warnings about
cholesterol x
The nation�s top nutrition
advisory panel has decided to drop its caution about eating cholesterol-laden
food, a move that could undo almost 40 years of government warnings about its
consumption.
The group�s finding that
cholesterol in the diet need no longer be considered a �nutrient of concern�
stands in contrast to the committee�s findings five years ago, the
last time it convened. During those proceedings, as in previous years, the
panel deemed the issue of excess cholesterol in the American diet a public
health concern.
The finding follows an
evolution of thinking among many nutritionists who now believe that, for
healthy adults, eating foods high
in cholesterol may not significantly affect the level of cholesterol in
the blood or increase the risk of heart disease.
The greater danger in this
regard, these experts believe, lies not in products such as eggs, shrimp or
lobster, which are high in cholesterol, but in too many servings of foods heavy
with saturated fats, such as fatty meats, whole milk, and butter.
[Scientists have figured out
what makes Indian food so delicious]
The new view on cholesterol in
food does not reverse warnings about high levels of �bad� cholesterol in the
blood, which have been linked to heart disease. Moreover, some experts warned
that people with particular health problems, such as diabetes, should continue
to avoid cholesterol-rich diets.
While Americans may be accustomed
to conflicting dietary advice, the change on cholesterol comes from the
influential Dietary Guidelines Advisory Committee, the group that
provides the scientific basis for the �Dietary Guidelines.� That federal
publication has broad effects on the American diet, helping to determine the
content of school lunches, affecting how food manufacturers advertise their
wares, and serving as the foundation for reams of diet advice.
The panel laid out the
cholesterol decision in December, at its last meeting before it writes a report
that will serve as the basis for the next version of the guidelines. A video of
the meeting was later posted online and a person with direct knowledge of the
proceedings said the cholesterol finding would make it to the group�s
final report, which is due within weeks.
After Marian Neuhouser, chair of
the relevant subcommittee, announced the decision to the panel at the December
meeting, one panelist appeared to bridle.
�So we�re not making a
[cholesterol] recommendation?� panel member Miriam Nelson, a Tufts University
professor, said at the meeting as if trying to absorb the thought. �Okay ...
Bummer.�
Members of the panel, called the
Dietary Guidelines Advisory Committee, said they would not comment until the
publication of their report, which will be filed with the Department of
Health and Human Services and the Department of Agriculture.
[Here�s what the government�s
dietary guidelines should really say]
While those agencies could ignore
the committee�s recommendations, major deviations are not common, experts said.
Five years ago, �I don�t think
the Dietary Guidelines diverged from the committee�s report,� said Naomi K.
Fukagawa, a University of Vermont professor who served as the committee�s vice
chair in 2010. Fukagawa said she supports the change on cholesterol.
Walter Willett, chair of the
nutrition department at the Harvard School of Public Health, also called the
turnaround on cholesterol a �reasonable move.�
�There�s been a shift of
thinking,� he said.
But the change on dietary
cholesterol also shows how the complexity of nutrition science and the lack of
definitive research can contribute to confusion for Americans who, while
seeking guidance on what to eat, often find themselves afloat in
conflicting advice.
Cholesterol has been a
fixture in dietary warnings in the United States at least since 1961,
when it appeared in guidelines developed by the American Heart Association.
Later adopted by the federal government, such warnings helped shift eating
habits -- per capita egg consumption dropped about 30 percent -- and harmed egg
farmers.
Yet even today, after more than a
century of scientific inquiry, scientists are divided.
Some nutritionists said lifting
the cholesterol warning is long overdue, noting that the United States is
out-of-step with other countries, where diet guidelines do not single out
cholesterol. Others support maintaining a warning.
The forthcoming version of the
Dietary Guidelines -- the document is revised every five years -- is
expected to navigate myriad similar controversies. Among them: salt, red meat,
sugar, saturated fats and the latest darling of food-makers, Omega-3s.
As with cholesterol, the dietary
panel�s advice on these issues will be used by the federal bureaucrats to draft
the new guidelines, which offer Americans clear instructions -- and sometimes
very specific, down- to-the-milligram prescriptions. But such precision
can mask sometimes tumultuous debates about nutrition.
�Almost every single nutrient
imaginable has peer reviewed publications associating it with almost any
outcome,� John P.A. Ioannidis, a professor of medicine and statistics at
Stanford and one of the harshest critics of nutritional science, has written.
�In this literature of epidemic proportions, how many results are correct?�
Now comes the shift on
cholesterol.
Even as contrary evidence has
emerged over the years, the campaign against dietary cholesterol has continued.
In 1994, food-makers were required to report cholesterol values on the
nutrition label. In
2010, with the publication of the
most recent �Dietary Guidelines,� the experts again focused on the problem of
"excess dietary cholesterol."
Yet many have viewed the evidence
against cholesterol as weak, at best. As late as 2013, a task force arranged by
the American College of Cardiology and the American Heart Association looked at
the dietary cholesterol studies. The group found that there was
�insufficient evidence� to make a recommendation. Many of the studies that
had been done, the task force said, were too broad to single out cholesterol.
�Looking back at the literature,
we just couldn�t see the kind of science that would support dietary
restrictions,� said Robert Eckel, the co-chair of the task force and a medical
professor at the University of Colorado.
The current U.S. guidelines call
for restricting cholesterol intake to 300 milligrams daily. American adult men
on average ingest about 340 milligrams of cholesterol a day, according to
federal figures. That recommended figure of 300 milligrams, Eckel
said, is " just one of those things that gets carried forward and carried
forward even though the evidence is minimal.�
"We just don't know,"
he said.
Other major studies have
indicated that eating an egg a day does not raise a healthy person�s risk of
heart disease, though diabetic patients may be at more risk.
�The U.S. is the last country in
the world to set a specific limit on dietary cholesterol,� said David
Klurfeld, a nutrition scientist
at the U.S. Department of Agriculture. �Some of it is scientific
inertia.�
The persistence of the
cholesterol fear may arise, in part, from the plausibility of its danger.
As far back as the 19th century,
scientists recognized that the plaque that clogged arteries consisted, in part,
of cholesterol, according to historians.
It would have seemed logical,
then, that a diet that is high in cholesterol would wind up clogging arteries.
In 1913, Niokolai Anitschkov and
his colleagues at the Czar�s Military Medicine Institute in St. Petersburg,
decided to try it out in rabbits. The group fed cholesterol to rabbits for
about four to eight weeks and saw that the cholesterol diet harmed them. They
figured they were on to something big.
�It often happens in the history
of science that researchers ... obtain results which require us to view
scientific questions in a new light,� he and a colleague wrote in their
1913 paper.
But it wasn�t until the 1940s,
when heart disease was rising in the United States, that the dangers of a
cholesterol diet for humans would come more sharply into focus.
Experiments in biology, as well
as other studies that followed the diets of large populations, seemed to link
high cholesterol diets to heart disease.
Public warnings soon followed. In
1961, the American Heart Association recommended that people reduce cholesterol
consumption and eventually set a limit of 300 milligrams a day. (For
comparison, the yolk of a single egg has about 200 milligrams.)
Eventually, the idea that
cholesterol is harmful so permeated the country's consciousness that marketers
advertised their foods on the basis of "no cholesterol."
What Anitschkov and the other
early scientists may not have foreseen is how complicated the science of
cholesterol and heart disease could turn out: that the body creates cholesterol
in amounts much larger than their diet provides, that the body regulates how
much is in the blood and that there is both �good� and �bad� cholesterol.
Adding to the complexity, the way
people process cholesterol differs. Scientists say some people � about 25
percent -- appear to be more vulnerable to cholesterol-rich diets.
�It�s turned out to be more
complicated than anyone could have known,� said Lawrence Rudel, a professor at
the Wake Forest University School of Medicine.
As a graduate student at the
University of Arkansas in the late 1960s, Rudel came across Anitschkov�s paper
and decided to focus on understanding one of its curiosities. In passing, the
paper noted that while the cholesterol diet harmed rabbits, it had no effect on
white rats. In fact, if Anitschkov had focused on any other animal besides the
rabbit, the effects wouldn't have been so clear -- rabbits are unusually
vulnerable to the high-cholesterol diet.
�The reason for the difference --
why does one animal fall apart on the cholesterol diet -- seemed like something
that could be figured out,� Rudel said. �That was 40 or so years ago. We
still don�t know what explains the difference.�
In truth, scientists have made
some progress. Rudel and his colleagues have been able to breed squirrel
monkeys that are more vulnerable to the cholesterol diet. That and other
evidence leads to their belief that for some people -- as for the squirrel
monkeys -- genetics are to blame.
Rudel said that Americans should
still be warned about cholesterol.
�Eggs are a nearly perfect food,
but cholesterol is a potential bad guy,� he said. �Eating too much a day won�t
harm everyone, but it will harm some people.�
Scientists have estimated that,
even without counting the toll from obesity, disease related to poor eating
habits kills more than half a million people every year. That toll is often
used as an argument for more research in nutrition.
Currently, the National
Institutes of Health spends about $1.5 billion annually on nutrition research,
an amount that represents about 5 percent of its total budget.
The turnaround on cholesterol,
some critics say, is just more evidence that nutrition science needs more
investment. Others, however, say the reversal might be seen as a sign of
progress.
�These reversals in the
field do make us wonder and scratch our heads,� said David Allison, a
public health professor at the University of Alabama at Birmingham. �But in
science, change is normal and expected.�
When our view of the cosmos
shifted from Ptolemy to Copernicus to Newton and Einstein, Allison said, �the
reaction was not to say, �Oh my gosh, something is wrong with physics!� We say,
�Oh my gosh, isn�t this cool?� �
Allison said the problem in
nutrition stems from the arrogance that sometimes accompanies dietary advice. A
little humility could go a long way.
�Where nutrition has some
trouble,� he said, �is all the confidence and vitriol and moralism that
goes along with our recommendations.�
The 2015 US Dietary Guidelines � Ending the 35% Limit on Total Dietary
Fat y
Every 5 years, the US Departments
of Agriculture and Health and Human Services jointly release the Dietary
Guidelines for Americans. These guidelines have far-reaching influences
across the food supply, including for schools, government cafeterias, the military,
food assistance programs, agricultural production, restaurant recipes, and
industry food formulations. An accurate revision of the Dietary Guidelines is crucial to the health of millions
of people. Integral to this process is the Dietary Guidelines Advisory
Committee (DGAC) report, just released, prepared by appointed scientists who
systematically review the literature and provide evidence-based recommendations
to the Secretaries of Agriculture and Health and Human Services. In the coming
months, the Secretaries will review the DGAC recommendations; consider comments
from the public, academics, advocacy groups, and industry; and finalize
the Dietary Guidelines.
In the new DGAC report, one
widely noticed revision was the dropping of dietary cholesterol as a �nutrient
of concern.� This surprised the public, but is concordant with scientific
evidence demonstrating no appreciable relationship between dietary cholesterol
and serum cholesterol or clinical cardiovascular events in general populations.
The DGAC should be commended for this evidence-based change.
A far less noticed, but more
momentous, change was the new absence of any limitation on total fat
consumption. The DGAC neither listed total fat as a nutrient of concern, nor
proposed any limitation on its consumption. Rather, they concluded, �Reducing
total fat (replacing total fat with overall carbohydrates) does not lower CVD
risk Dietary advice should put the emphasis on optimizing types of dietary fat
and not reducing total fat.� Limiting total fat was also not recommended for
obesity prevention; instead, the emphasis was on evidence-based healthful
food-based diet patterns higher in vegetables, fruits, whole grains, seafood,
legumes, and dairy products; and lower in meats, sugar-sweetened foods and drinks,
and refined grains.
With these quiet statements, the
DGAC boldly reversed nearly 4 decades of focus on reducing total fat. Starting
in 1980, the Dietary Guidelines emphasized limiting dietary fat, initially to
<30% of calories and then, in 2005, to between 20�35% of calories.
Throughout, the main rationale was to lower saturated fat and dietary
cholesterol, rather than any clear evidence for direct harms of total fat. This
reasoning overlooked the complex lipid and lipoprotein effects of saturated fat,
including minimal effects on Apo-B in comparison to carbohydrate; this explains
why substitution of saturated fat with carbohydrate does not lower
cardiovascular risk. Moreover, a global limit on total fat inevitably lowers
intake of unsaturated fats, among which nuts, vegetable oils, and fish
are particularly healthful. Most relevantly, this limitation did not account
for harms of starches and sugars, the most common replacement when dietary fat
is reduced. Indeed, the 1980 Dietary Guidelines recommended that intake of �complex carbohydrates� be increased,
largely based on theoretical considerations (carbohydrate contains fewer
calories per gram than does fat) instead of evidence for health benefits.
As with other scientific
fields from physics to clinical medicine, nutritional science has
advanced dramatically in recent decades. The 2015 DGAC report, for the
first time, is consistent with the accumulated evidence for lack of
efficacy of recommending high-carbohydrate, low-fat diets to the general
population for any major endpoint, including heart disease, stroke, cancer,
diabetes, or obesity.
Related to this, the 2015 DGAC
renews the 2005 and 2010 Dietary Guidelines call to restrict both added sugars
and refined grains. For decades, complex carbohydrates were considered a
foundation of a healthful diet, e.g. as evidenced by the Food Guide Pyramid
base. This was revised in 2005, based on consistent evidence for harms of
starches and sugar. Yet, refined grains continue to represent the largest
category of calories in the US food supply, including white bread, white rice,
and most chips, crackers, cereals, and bakery desserts. Both industry and
consumers have been unsuccessful in meaningfully reducing refined
carbohydrates, a failure likely exacerbated by decades of focus on lowering
total dietary fat. Recognizing this harmful confusion, the 2015 DGAC
specifically concludes that, �consumption of �low-fat� or �nonfat�
products with high amounts of refined grains and added sugars should be
discouraged.� Yet, more than 70% of Americans continue to exceed the optimal
amount of refined grain consumption. Dropping the limitation on total fat
should make it easier for industry, restaurants, and the public to increase
healthful fats and proteins while reducing refined grains and added
sugars.
The US Departments of Agriculture
and Health and Human Services should follow the evidence-based,
scientifically sound DGAC report and remove any limit on total fat
consumption in the final 2015 Dietary Guidelines. Yet, this represent
only one policy tool to influence American diets, and others should
follow suit. For example, the Nutrition Facts Panel, separately regulated by
the US Food and Drug Administration, lists % daily values for several key
nutrients on packaged foods. Remarkably, this Panel still has not been updated
to revise the outdated 30% limit on dietary fat, obselete for almost 15 years.
The Nutrition Facts Panel should now be revised to drop total fat, as well as
dietary cholesterol, from among the listed nutrients, while adding contents of
both refined grains and added sugars. Notably, only adding added sugars,
a current proposed change, insufficiently acknowledges the harms of � and
implicitly encourages � the intake of refined grains. The US Department
of Agriculture should also modernize its Smart Snacks in School standards,
removing the 35% restriction on total fat from the criteria. The Institute of
Medicine should also update its report, now nearly 15 years old, on dietary
reference intakes for energy, total fat, and other macronutrients.
The current restriction on total
fat affects virtually all aspects of the American diet, including school meals
(which currently ban whole milk, but allow sugar-sweetened non-fat milk),
government procurement for offices and the military, meals for the elderly,
and guidelines for food assistance programs that together provide 1 in 4 meals
consumed in the US. The restriction on fat also drives food industry
formulations and marketing, as evidenced by the heavy promotion of fat-reduced
desserts, snacks, salad dressings, processed meats and other products of
questionable nutritional value. Not surprisingly, a majority of Americans are
still actively trying to avoid dietary fat, which is typically replaced by
refined carbohydrates including highly processed grains, potato products,
and added sugars. The limit on total fat presents an impediment to public
health, promoting harmful low-fat foods, encouraging high intakes of starch and
sugar, and discouraging the restaurant and food industry from providing
products and meals high in healthful fats. Based on the accumulated new
scientific evidence, the Dietary Guidelines for Americans, Nutrition
Facts Panel, Smart Snacks in School standards, and Institute of Medicine should
remove the 35% limit on total dietary fat. This scientifically sound
change will have major positive influences on the US food supply, food
industry formulations and marketing, and public perception and understanding of
evidence-based dietary priorities.
(back
to content)
1.2.0
Medicine in Africa (Eden extension)
Eden (most of it is in Nigeria and then most of Cameroon as the center
and extending to other countries around Africa)
The place of language and migration origin is the origin of humanity.
That is where you can trace the true origin of Medicine, which is why it
started that was to complement the fall of humans from life that is spirit that
did everything. Nigeria is clearly the most cursed land on Earth that shows
from the failed state of governance to the waste of human capital because of
indigenes that want to stick to their status quo; Nigerians are the most
educated group in the USA, yet in the most educated state in Nigeria that every
family has a professor, they are the most poor in unutilized potential.
After which people were driven to the east as stated in religious
scriptures, in which Sumerians began the physical way of living with the
hardship of the curse. Any Occidental disputing this should ask the skilled
orients where most of their techniques originated from that the Orientals
perfected.
 �c
�c
Bantu Migration
Today, close to 100 million people across the southern half
of Africa speak related languages, collectively known as Bantu languages.
Linguistic evidence shows that the root Bantu language emerged in what is now
Nigeria and Cameroon by 2000 bc. By 1000 bc, in a series of migrations, Bantu
speakers had spread south to the savanna lands of Angola and east to the Lake
Victoria region. Over the next 1500 years they scattered throughout central and
southern Africa, interacting with and absorbing indigenous populations as they
spread.
� Microsoft Corporation. All Rights Reserved.
Microsoft � Encarta � 2009. � 1993-2008 Microsoft
Corporation. All rights reserved.
� �C
�C
Ancient Routes of Migration
Physical barriers, including deserts, mountain ranges, and
bodies of water, inhibited ancient people�s migrations. In addition, migrating
groups tended to seek a habitat similar to the ones they had left.
� Microsoft Corporation. All Rights Reserved.
Microsoft � Encarta � 2009. � 1993-2008 Microsoft
Corporation. All rights reserved.
The dark Africans that remained in the heat that caused the Sahara
Desert to separate the rest of the world from sub-Saharan Africa, learnt better
hygiene like brushing, washing and bathing that they taught the occidentals
when the dark skinned Africans were called the Moors. Now, online, the moors
have been manipulated to be the Arabs only; the question everyone should think
about is how can there be mud in the Middle East. Mud is in the swampy areas
that are a lot in West Africa and Central Africa where the Moors were. Most of
the idols of gods are seen with wooly hair and big broad nose in Scotland,
Mexico etc. Even the bible has the Ethiopian teaching what Jesus (Prophet Isa)
meant n the Acts of the Apostles. Also the independence of Nigeria has been manipulated
online from the original eleven names of ten men and one woman.
Health Care: -
1. Brushing: brush the front of the teeth up and down, brush the crown,
brush the back of the teeth outwards, and then brush your tongue looking at the
mirror. Then, pull on the mucus and phlegm in the throat to remove bad breath.
The villagers in sub-Saharan Africa always used water to rinse their mouth
after eating. Brush the back of the tongue to remove mouth ordour and
uncomfortable feeling in the mouth.
2. Shaving: shave downwards, clean-shave (shave downwards then,
upwards) for those that don't develop bumps (hair growing inwards)
3. Cutting hair: it is best to trim the hair than to shave-off the hair
around the body or the head, your hair is for a purpose. The style of cutting
the side of the hair lower than the rest of the hair by the whites was done by
the dark skinned Africans when they were looked up to by the Arcadians.
4. Bathing: wash your face twice with soap as you bathe if you have
oily skin, once for dry skin, bathe twice or thrice a day. Always scrub the
soles of your feet at least once a week. Wash your hair with a lot of soap to
lather and there will be no dandruff. Use sponge to scrub of dead old skin to
prevent body odor. Blow your nostrils with water while bathing or after a dusty
environment. Dropping castor oil at night before you sleep clears worms etc.
from the eyes after about six months.
5. If the urge to go to toilet comes in uncomfortable circumstances,
lay down with your belly facing upwards and it will subside the feeling; but if
your stomach is troubling you, lay with your stomach downwards and it will
reduce. Which delays you until the right circumstances to use the toilet or the
person getting the medication are available.
6. When you sleep and in your dreams, you are always caught or you do
not win, straighten your legs and you will always win and will never be caught.
7. When eating an orange cut twice, giving four parts, bite the center
of the fruit and pull your teeth to the central part of the fruit that was cut
to take out all the seeds, then you can enjoy the seedless fruit.
The colonialist humiliation of the dark skinned as not able to have
developed any structure, is the loss of their knowledge about the sprit and
soul treatment, as they only treat the body, so their psychology cannot treat
the mind effectively but suppress the information when the spirit should have
been let to treat the mind. Those who left from Africa to stay abroad do not
know the knowledge of the spirit like their traditional rulers that are not
allowed to leave the thrown to stay abroad because the knowledge is passed down
to the leaders. Everyone in the village is trained by their family to be a
native doctor by showing them the plants in their native dialect and their
medicinal value to keep them always well, where those who know more than others
that pass down that knowledge to their descendants (either by prayer or laying
of hands as it was with Abraham to Jacob in the Bible or Koran) are regarded as
the native doctor of the village that knows more; those without western
civilization do not know sickness until something alien enters their community,
because of the herbs they eat in their food that has usually all the required
nutrients and medication they need with assorted meats from water, land and
air. Which is contrary to the colonialists� false information that they passed
to their government to allow colonization and use of the human resources that
coveted their neighbours goods. Yet science proves that Homo Sapiens are those
that left from Africa as Bible Enoch etc. to populate the rest of the world by
inter breeding with other species.
(back
to content)
1.2.0.1
Egypt m
Our knowledge of ancient Egyptian
medicine comes from certain medical papyri and from the embalming of Egyptsian
dead. The papyri contain various descriptions of magic spells designed to drive
out the demon causing a particular disease and of various prescriptions,
including the dosage for particular diseases. Drugs used included castor oil,
hartshorn, bile and fat from animals and copper sulphate. Treatment was
prescribed for wounds and bruises and surgical instruments appear to have been
used and broken bones were treated with splints. The ancient Egyptians made shoes for each foot, one for the left and
the right, based on spiritual insight; contrary to the colonialist shoe making
that was designed for both legs that are usually not the same.
The Egyptian practice of
embalming and the favourable conditions of Egypt for the natural preservation
of bodies shows us some of the diseases the Egyptians suffered from. Arthritis
and inflammation of the periosteum and osteomyelitis were common. Spinal
deformations and spinal tuberculosis, gout and virulent osteomas have been
found in Egyptian mummies. Tooth decay was as common as in modern times and
there is good evidence of kidney stones and gall stones, appendicitis and
stomach and intestinal troubles. The lower classes in particular suffered from
infectious diseases such as plague, smallpox, typhus, leprosy, malaria, amoebic
dysentery and cholera and various parasitic diseases. The Egyptian embalming is based on the idea of them returning to their
alien leaders.
Egyptian physician�s knowledge of
anatomy was not extensive despite the practice of embalming. This is because
embalming was carried out by specialist technicians and not by physicians.
Knowledge of internal organs was largely limited to an awareness of their
outward appearance.
1.2.0.3
Imhotep w
Imhotep (/ɪmˈhoʊtɛp/; Ancient Egyptian: ỉỉ-m-ḥtp
"the one who comes in peace"; fl. late
27th century BCE) was an Egyptian chancellor to the Pharaoh Djoser,
possible architect of
Djoser's step pyramid, and high priest of the sun god Ra at Heliopolis.
Very little is known of
Imhotep as a historical figure, but in the 3,000 years following
his death, he was gradually
glorified and deified.
|
Imhotep
|
|
Ancient Egyptian: Jj m ḥtp
|
|
|
Burial place���������������������������������������������������������������
Saqqara (probable)
Other names����������������������������� �������������������������������Asclepius (name
in Greek) Imouthes (also name in Greek)
Occupation�������������������������������� �������������������������������chancellor to
the Pharaoh Djoser and High
Priest of Ra
Years active��������������������������������������� ������������������������c. 27th century
BCE
Known for������������������������������������������������������������������
Being the architect of Djoser's step pyramid
�
Greek Manetho variants:
Africanus: Imouthes Eusebius:
missing Eusebius, AV: missing
Traditions from long after
Imhotep's death treated him as a great author of wisdom texts and especially as
a physician. No text from his lifetime mentions these capacities and no text
mentions his name in the first 1,200 years following his death. Apart
from the three short contemporary inscriptions that establish him as chancellor
to the Pharaoh, the first text to reference Imhotep dates to the time of
Amenhotep III (c. 1391�1353 BCE). It is addressed to the owner of a tomb,
and reads:
�
The wab-priest may give offerings
to your ka. The wab-priests may stretch to you their arms with libations on the
soil, as it is done for Imhotep with the remains of the water bowl.
� Wildung (1977)
It appears that this libation to
Imhotep was done regularly, as they are attested on papyri associated with
statues of Imhotep until the Late Period (c. 664�332 BCE). Wildung (1977)
explains the origin of this cult as a slow evolution of intellectuals' memory of
Imhotep, from his death onward. Gardiner finds the cult of Imhotep during
the New Kingdom (c. 1550�1077 BCE) sufficiently distinct from the
usual offerings made to other commoners that the epithet "demigod" is
likely justified to describe his veneration.
The first references to the
healing abilities of Imhotep occur from the Thirtieth Dynasty (c. 380�343
BCE) onward, some 2,200 years after his death.
Imhotep is among the few
non-royal Egyptians who were deified after their deaths, and until the
21st century, he was one of nearly a dozen non-royals to achieve this status.
The center of his cult was in Memphis. The location of his tomb remains
unknown, despite efforts to find it. The consensus is that it is hidden
somewhere at Saqqara.
Historicity
Imhotep's historicity is
confirmed by two contemporary inscriptions made during his lifetime on
the base or pedestal of one of Djoser's statues (Cairo JE 49889) and also by a
graffito on the enclosure wall surrounding Sekhemkhet's unfinished step
pyramid. The latter inscription suggests that Imhotep outlived Djoser by a few
years and went on to serve in the construction of Pharaoh Sekhemkhet's pyramid,
which was abandoned due to this ruler's brief reign.
Architecture and engineering
 �
�
The step pyramid of Djoser
Imhotep was one of the chief
officials of the Pharaoh Djoser. Concurring with much later legends,
egyptologists credit him with the design and construction of the Pyramid of
Djoser, a step pyramid at Saqqara built during the 3rd Dynasty. He may also
have been responsible for the first known use of stone columns to support
a building. Despite these later attestations, the pharaonic Egyptians
themselves never credited Imhotep as the designer of the stepped pyramid, nor
with the invention of stone architecture.
Deification
God of medicine
Two thousand years after his
death, Imhotep's status had risen to that of a god of medicine and healing.
Eventually, Imhotep was equated with Thoth, the god of architecture,
mathematics, and medicine, and patron of scribes: Imhotep's cult was merged
with that of his own former tutelary god.
He was revered in the region of
Thebes as the "brother" of Amenhotep, son of Hapu � another
deified architect � in the temples dedicated to Thoth.: v3, p104.
Because of his association with health, the Greeks equated Imhotep with
Asklepios, their own god of health who also was a deified mortal.
According to myth, Imhotep's
mother was a mortal named Kheredu-ankh, she too being eventually revered as a
demi-goddess as the daughter of Banebdjedet. Alternatively, since Imhotep was
known as the "Son of Ptah",: v?, p106 his mother was
sometimes claimed to be Sekhmet, the patron of Upper Egypt whose consort was
Ptah.
Post-Alexander period
The Upper Egyptian Famine Stela,
which dates from the Ptolemaic period (305�30 BCE), bears an inscription
containing a legend about a famine lasting seven years during the reign of
Djoser. Imhotep is credited with having been instrumental in ending it. One of
his priests explained the connection between the god Khnum and the rise of the
Nile to the Pharaoh, who then had a dream in which the Nile god spoke to him, promising
to end the drought.
A demotic papyrus from the temple
of Tebtunis, dating to the 2nd century CE, preserves a long story about
Imhotep. The Pharaoh Djoser plays a prominent role in the story, which also
mentions Imhotep's family; his father the god Ptah, his mother Khereduankh, and
his younger sister Renpetneferet. At one point Djoser desires Renpetneferet,
and Imhotep disguises himself and tries to rescue her. The text also refers to
the royal tomb of Djoser. Part of the legend includes an anachronistic battle
between the Old Kingdom and the Assyrian armies where Imhotep fights an
Assyrian sorceress in a duel of magic.
As an instigator of Egyptian
culture, Imhotep's idealized image lasted well into the Roman period. In the
Ptolemaic period, the Egyptian priest and historian Manetho credited him with
inventing the method of a stone-dressed building during Djoser's reign, though
he was not the first to actually build with stone. Stone walling,
flooring, lintels, and jambs had appeared sporadically during the Archaic
Period, though it is true that a building of the size of the step pyramid made
entirely out of stone had never before been constructed. Before Djoser, Pharaohs
were buried in mastaba tombs.
Medicine
Egyptologist James Peter Allen
states that "The Greeks equated him with their own god of medicine,
Asklepios., although ironically there is no evidence that Imhotep himself was a
physician."
(back
to content)
1.2.0.4 Colonial
Medicine Influence T
This is a comprehensive survey of
the colonial history of medicine in some seventeen African countries that would
be monumental where the colonialist emotionally thought for the people as God
had cursed; and is proposed to take as a theme a pattern which runs throughout
the story, a pattern which� seems to� indicate�
that� the� short�
history� of medicine in the
Commonwealth� countries� in Africa-for�
in its significant aspects it spans little more than� a century-is�
largely the history� of their
medical services; and it is the development�
of medicine� through� those�
services that� I shall try to� sketch very broadly and with, inevitably,
many gaps.
Before the opening of Africa to
exploration, settlement, trade and missionary enterprise, the African people
were not exposed to tremendous stresses and the mortality was immense. For
medical treatment, they relied upon their indigenous practitioners,
usually-although not�� always
accurately-referred to as witch-doctors. These medicine-men practiced largely
by spiritual suggestion, incantations, charms and remedies; but with their
knowledge of herbs and roots, they often discovered by intuition, which the
colonial medical practitioners saw as perhaps by serendipity, a number of
effective indigenous drugs.� Some of
these, indeed, have more recently been shown to have real therapeutic value and
are known to be effective in conditions such as diarrhea and some of the
intestinal parasitic diseases. These discoveries were empiric: but then so were
many of our own; and relative to cultural development, there is little basic
difference between the application of their concoctions and the practice of
carrying potatoes in the pocket as a cure for rheumatism. Nevertheless, their
approach knew something of science: disease was held-as it is held in many fractals
that the colonialists saw as primitive African communities today-to be the
result of the direct activity of spirits, who had to be placated, yet the modern
world now operates in similar fractal condition that if they had mastered, the
world will not be in difficulty. Tribal mores were strong and the influence of
the physical environment in the sense that we know it today was not considered.
The dawning of western medicine
began gradually as exploration and settlement developed. Sporadic contributions
had been made in the eighteenth century as a result of observations made by individual
naval and military surgeons and missionary doctors, but these contributions
were not appreciated fully at the time and their immediate influence was small.
However, some classic records remain.�
One of these was the account in 1803 by Thomas Winterbottom, Physician
to the Colony of Sierra Leone from 1792 to 1796, of the Africans in Sierra
Leone and 'the present state of medicine among them'. This is commonly claimed
to contain the first English account of sleeping sickness.
In fact, that account was given
by John Atkins, a naval surgeon, who practiced in West African waters and who
met the disease on the Guinea Coast in 1721.' In his description of 'the sleepy
Distemper in Negroes', in his book The Navy Surgeon [1734), he states:� 'Their sleeps are sound, and sense and feeling
very little: for pulling, drubbing, or whipping will scarce stir up sense or
power enough to move, and the moment you cease beating, the smart is forgot'.
To these somewhat Draconian
diagnostic measures were added a schedule of treatment which sounds a little
drastic to our ears, but was no doubt not without benefit to the patient:� 'bleeding in the jugular, quick purges,
stematories, vesicatories, acupuncture, seton, fontanels, and Sudden Plunges in
the Sea: the latter is most effectual when the distemper is new, and the patient
is not yet attended with a drivling at mouth or nose'. It is the charlatan
method of treatment that the colonialists used to make our colonial medical
practitioners to be dependent on the prescription of their imported medicine to
make our economy dependent on the occidental economic system.
Nevertheless, a sound basis had
been established by educated naval surgeons who were concerned not only with
the maladies prevailing in warm climates but with those incidents to getting
there.� The navigators venturing to Africa
and elsewhere owed much to such far-sighted pioneers as Gilbert Blane and James
Lind.
A great deal of the early
provision of medical facilities for Africans was owed to missionary
enterprise.� The example of David
Livingstone contributed largely to the establishment of medical work as a
recognized part of missionary activity.�
Others were soon to follow and medical missionary work rapidly expanded
in West, East and South Africa through the efforts of various churches who
increasingly provided training for their members and the establishment of
hospitals, dispensaries and other medical facilities.
For example, John Abercrombie in
1841 founded the Edinburgh Missionary Society for training medical students for
missionary work. Yet in 1849 it was estimated that there were only 40 medical
missionaries in the whole world. In 1863, lay doctors were associated with the
Holy Ghost Fathers in 'Zanzibar; and the Universities' Mission to Central Africa
and the Church Missionary Society started medical missionary services in
various parts of Africa.� The latter Society
founded Livingstone College for instructing missionaries in the elements of
practical medicine in 1893 and in 1897 founded a hospital in Uganda.� The White Fathers had started work in the
regions of the great lakes in East Africa in 1878 and in� 1899 the White� Sisters instituted� health work there.
Within the British sphere of
influence in Africa, it is not surprising that the first glimpses of activity
should have been seen in the West African territories.� Sierra Leone was among the oldest of these.
When a free settlement of Negro slaves from Nova Scotia was begun there in
1787, through the vision of the philanthropist Granville Sharp, it was almost
wiped out by disease at the very beginning. Although conditions apparently
improved, through the use of ordinary basic methods of hygiene, the improvement
benefited largely the settlers and their families alone.� Health conditions throughout West Africa were
bad; and yellow fever, malaria and other conditions took a toll so great that
there was a constant struggle with disease, handicapped by a lack of knowledge.
That remarkable woman Mary Kingsley in her West African Studies, published in
1899, 13 deplored prevailing apathy and noted that 'no trouble is taken to pull
down the death-rate by Science'. Although the Africans who relied on their
herbal preventive measures never knew this diseases effect. Africa had been
protected from global pandemics by the Sahara Desert.
While expeditions and the various
Chartered Companies had provided such medical assistance as they could, it was
sparse and not easy to come by. Indeed even two years after� Sierra Leone�
had� been handed� over to�
the� Crown� in�
1808, a Commission� of
Inquiry,� referring� to� the� medical�
department,�� stated:� 'The�
provisions� for� this�
department,� in a recent
parliamentary vote, were a first and second surgeon, an apothecary and his
assistants;� and were these offices filled
up in a suitable way they might have been sufficient to effect their
purpose� but such is the proportion� of the salaries to the efficiency and ability
required� in the officers, that� no competent�
person could be found� to accept
the first two posts'.
The early Administrations�� in Africa had at first mainly devoted the
provision of medical services, through force of circumstances, to the needs of
existing establishments. The wider extension of these to the African
communities as a whole had to wait upon further knowledge, better
communications, more staff and more money. The 'insalubrity' of the climate
blamed by the earlier observers as the source of illnesses in Tropical Africa
was a misnomer:� for the major enemy of
progress was not the climate, but the mosquito; yellow fever, malaria, filariasis
and diseases not then identified as arthropod-borne had dominated the scene and
frustrated the efforts of pioneers to establish permanent health
conditions.�
Malaria wrecked many expeditions
and some of these are vividly described by Gelfand in his monograph Rivers of
Death.� With the first proof of the role
of a blood-sucking insect as a vector of parasites pathogenic to man, Manson in
1879 had started a movement-for it was no less-which was to influence the
future of tropical medicine and hygiene for all time. As one of his
biographers, Alcock,' wrote, Manson's discovery 'merely as a scientific
achievement laid open a large new territory for investigation, started a flood of
new ideas, and thus paved the way for fresh conquests over ignorance'. The
encouragement and influence which Manson gave to Ronald Ross, culminating in
his demonstration that mosquitoes were vectors of malaria parasites, is now familiar
history:� but although Ross's discoveries
were first made in India, his further application of this knowledge to
parasitic disease profoundly affected the health of all tropical countries and
Africa was one of the first to gain. In 1899, Ross visited Sierra Leone and not
only identified the vector of human malaria there, but subsequently set out
proposals for dealing with it. In 1901 he prepared a report on the main
measures required to reform health conditions in West Africa. Later he was to
visit Lagos in Nigeria and Accra in the (then) Gold Coast and other
investigations were to follow. In 1909 that great pioneer of tropical hygiene,
Sir William Simpson, visited various parts of West Africa to study the existing
organization of the medical services, particularly from the public health
aspect. His very full report showed that while curative medicine had made
considerable strides as a result of newer knowledge, prevention of
disease-especially�� as regards the great
mass of indigenous people-had made little progress:� 'the conditions that have changed', he wrote,
'belong to the individual rather than to the locality'.
The appearance of Mary Kingsley's
book and Ross's investigations took place at about a period when a great step
was taken in the organization of medical services in Africa and elsewhere. A
far-sighted Colonial Secretary, Mr. Joseph Chamberlain, on the advice of
Manson, addressed the General Medical Council and the principal British Medical
Schools in 1888 with the proposal that medical officers appointed to tropical
territories should have a special knowledge of tropical diseases. Ten years
later in a despatch to all Governors of Colonies he advised that a special
school for training in tropical medicine should be set up and that this subject
should be taught on a wider scale in the principal medical schools in the
United Kingdom. The London School of Tropical Medicine was founded in 1899: but
it was not, in fact, the first, for a similar school had been established in
Liverpool, earlier in the same year, not by government initiative but by the
enthusiasm of a great captain of industry, Mr. (later Sir) Robert Jones, whose
interests in the West Coast of Africa were considerable. The pattern of the
present organization of medical services in Africa may be said to have taken
shape in the establishment of an amalgamated West African Medical Service in
1902. Similar groupings were to follow: The East African Medical Services were
amalgamated in 1903, though they separated later, but again achieved some
closer union. The eventual logical step was the establishment of a Colonial
Medical Service with appointments made in London, but with their own local
administrations yet with a similar structure which varied according to their local
requirements.�
In East Africa, for example,
although the pattern of development followed lines similar to those in West
Africa, there were a number of differing local factors which required special
approaches.� In East Africa generally
there were eventually many Asian immigrants, and numerous European settlers in
highland areas, and thus the racial distribution differed from that in West
Africa. In Kenya, the medical department was first organized in 1905, when
control of the country passed to the Colonial Office, although there had been a
few medical officers in the days of the Chartered Company. In Uganda, there was
a Government Hospital in Kampala in 1908, but Mulago Hospital, opened as a
general hospital in 1922, was to become eventually the now magnificent teaching
hospital for the medical school of the East African University College in
Makerere. Uganda was indeed early in the field of training African medical
personnel.� From an initial course of
training in Mengo in 1917, there developed in time the medical school with full
facilities for professional training which now exists. The ravages of sleeping
sickness which plagued Uganda in the opening years of this century was a
particular factor in stimulating a new attitude in the provision of health
services for Africans. In some infected areas, as many as 200,000 persons died.
This resulted, among other awakenings,
in a stimulus to the Royal Society to send commissions to study African
sleeping sickness and one result of the heightened interest in this alarming
disease was the foundation by the Colonial Office in 1908 of the Sleeping
Sickness Bureau in London, formed to collect and distribute information on this
disease. This organization was the forerunner of the Bureau of Hygiene and
Tropical Diseases whose abstracting Bulletins are still a guiding light to
current literature on tropical medicine and hygiene. The development of
medicine and medical services in Tanganyika was a natural extension of the
groundwork inherited from the former German East Africa. When the country
became a Mandated Territory under British administration�� in 1923 medical services went ahead.� The history of their development has been
admirably related by Clyde.� In Zanzibar,
Nyasaland and the High Commission Territories of Basutoland, Bechuanaland and
Swaziland, development took place slowly on the general pattern suited to their
local conditions.
In South Africa, already with a
long medical history, a Ministry of Public Health was established in 1919.
Here, development of medical services which had been occurring steadily for
more than two hundred years was naturally more sophisticated than that of its
neighbours and it has progressed along western lines. The large factors of
mining and of immigrant labour on a large scale from neighbouring countries
posed, however, special problems of their own.
The medical problems of Southern
Rhodesia were similar to those of the Union, though malaria was a greater
problem.� Northern Rhodesia (now Zambia)
has had problems of sleeping sickness and the additional health questions posed
by the large amount of labour in its copper mines. In 1948, Southern Rhodesia
acquired a Minister of Health and the Medical Department was subdivided into
curative and preventive services.
While Egypt and the Sudan no
longer fall within the scope of this survey, their past contributions to the
development of medicine in African countries of the Commonwealth have been
considerable.� A great deal of intensive
work on tropical diseases, especially on schistosomiasis, has been carried out
in these countries, much of it by Commonwealth��
workers in two world wars; and the contributions�� made by the Wellcome Tropical Research
Laboratories in Khartoum, equipped by Henry Wellcome in 1902, and the training
of Sudanese in the Kitchener School of Medicine founded in 1924 have been
significant landmarks.�
The pioneer work of such great
figures as Balfour and Chalmers is well known. It would not be practicable within
the compass of a single lecture-and it would in any case, be extremely boring
to the listener-to list the detailed forms which medical developments took in
the different countries.� Basically, the
ground structure was the same; a central administration, medical staff deployed
on regional and district bases, with hospitals of varying grades, health
centres, dispensaries and ancillary staff according to the needs and the
resources of particular areas. In addition, there are general and specialized
laboratories, and, in larger centres, research institutes, sleeping sickness organizations�� where these are required, mass campaigns
against endemic diseases and-as in Nigeria-mobile units derived from these and
now used as 'shock troops' for dealing with epidemics, surveillance and other
activities.� Today in the
independent�� countries, the pattern
tends to be that of Ministries of Health, rather than of the former Medical
Departments.
Most important� are the training centres, which vary from
full-scale medical schools, such� as� those�
in� Ibadan�� in�
Nigeria,� Makerere� in�
Uganda,� and� the�
University� of Rhodesia,� to others training� more specifically various grades of medical
auxiliaries medical assistants� with a
broad� training� not up to graduate� status,�
laboratory� technicians,� field�
assistants� and� various�
dispensers� and� 'Aides',��
all� with� a�
degree� of knowledge sufficient to
deal with the kind of problems� which
might be encountered at their level in the field. The emphasis on training today
is on prevention and many campaigns are frequently sponsored by W.H.O., after
which not only are the local staff encouraged to maintain the work themselves,
but where possible the machinery is integrated into the general public health
services.
It must not be thought, however,
that medicine in Africa has developed solely from the efforts of the
territorial administrations.�� Reference
has already been made to the great work carried out by the medical missions. In
addition, the increase in the industrial, agricultural, commercial, mining and
other forms of development brought with it many companies and other agencies. Several
of these have their own medical staff, some of them highly organized. Not only,
therefore, is occupational hygiene finding its place in the new Africa, but
these agencies have much to contribute to health in general both alone and in
association with governmental enterprise.
To discuss the prevailing
diseases of the African countries in the Commonwealth would be a story in
itself. In any case most of the diseases commonly called tropical are present
there as elsewhere, and perhaps the only truly indigenous one is African
trypanosomiasis.� It would not perhaps be
out of place, however, to note that as the means of controlling these diseases
improve and are extended, they will bring more into perspective the importance
of the cosmopolitan diseases. These have always been there, less obtrusive
perhaps because of the more specifically tropical conditions, but likely to be
more so as the pattern of living changes.�
Cerebrospinal meningitis has been constantly present and has caused many
serious epidemics, especially in West Africa, during the century. Measles is a
prominent killing disease of African children. Tuberculosis is a major problem
and despite modern advances in treatment and prevention these measures are
commonly restricted or modified by logistics and cost, though some notable advances
have been made. Venereal disease is widespread.
Occupational disease is likely to
become more prominent as development advances. The wide studies and knowledge
of virus diseases have served to uncover many infections which were hitherto
not identified.� For example, it is only
in recent decades that the extent of poliomyelitis in Africa has been
recognized.� Of special interest is the recognition
of increasing numbers of infections caused by arboviruses, some indeed having
been identified originally in Africa. Two of these are of special interest.
Chikungunya virus was first isolated as a result of a study of a dengue-like
outbreak in Tanganyika in 1952. Now it is a well-recognized member of the
arbovirus group and its incidence has been shown far afield, as in its
association with haemorrhagic and dengue-like fevers in such countries as India
and Thailand.� O'Nyong-Nyong fever, also
a dengue-like disease, was identified in Uganda in 1959. Of particular interest
was a finding that it showed some interference with outbreaks of malaria and
this phenomenon is being pursued.
A very topical subject, with an
African history, is Burkitt's tumour, a lymphoma notably found in African
children. It was given prominence by Burkitt in Uganda in the 1960s but has
since been detected widely in many other countries, in various subjects and
forms. Epidemiological studies showed a striking association between
topographical, meteorological�� and�� other��
features�� and�� conditions��
favourable�� to mosquito�� breeding.�
This suggested a possible arborvirus aetiology and vigorous studies are
being pursued, not only in Africa, but in many virus research institutes in
Europe and the United States, on this aspect of the subject. The implications of
these studies in the investigation of a possible role of viruses in the
aetiology of cancer are enormous; and although a number of viruses have been isolated
from Burkitt's tumours, none in fact has so far been incriminated as being
causative. �
What were the factors which
influenced the course of medicine in Africa from the first gropings of the
mid-nineteenth century to the vast developments in the twentieth? There were a
number, at first sight unrelated, but to some degree overlapping and they weave
between them an enlightening story of medico-social evolution.� The central point of all this was the African
himself, with his soil, his animals, his tribal mores, a whole environment
which was engaged in a constant struggle with two formidable foes-poverty and
parasites. Although Afrca at the time never needed money for anything other
than on market days because, trade by barter for every day requirements was
normal.
Basically, there were certain
operating factors. There was the more enlightened attitude of the Colonial
Administrations. There was the co-operation of missionary, governmental and
non-governmental agencies in the joint application of knowledge and resources.
There was the opening up of trade, industry, commerce and communications and
with it the provision of men, money and momentum to apply practical
measures.� There was a vast and rapid
increase in scientific knowledge and research with the discovery of new drugs,
antibiotics, insecticides and the application of public health engineering.
There was the development of W.H.O. with its help and guidance. There was the
effect of wars, especially two world wars, which influenced the application of
practical medical measures, both for better and for worse.� There was the impact of migration and
urbanization, with all the consequent results of the breaking of tribal and
family ties and the exposure to tuberculosis, venereal and other diseases of
overcrowding.� There was the achievement
one by one, of national independence by African countries and of a new status
and pattern of living. Above all there were two outstanding factors, the
recognition of the over-riding importance of preventive rather than solely
curative medicine and the education, particularly�� the health education, of the peoples
themselves.
The South African war had
produced a striking object lesson in the need for preventive medicine in the
field. For some 7,000 men killed in action, for example, there were 57,000
affected by typhoid.� The First World War
broke out with a knowledge of tropical medicine already established on a sound basis:� but there was still much to learn and a great
stimulus was provided by the urgent necessity for protecting troops against
disease in the field; and tropical medicine emerged enriched by its experience and
triumphant�� in a newer knowledge which
was soon applied to the problems of peace.�
The Second World War found the African countries better equipped for the
formidable tasks which faced them; and while the civil medical departments were
greatly depleted, they were constantly learning the new lessons which the
various campaigns in different regions of Africa and elsewhere had taught them.
The introduction of many synthetic antimalarials, drugs for use against
sleeping sickness, schistosomiasis and other helminthic diseases and the use of
sulphones for leprosy played a notable part.�
The development of D.D.T. and related insecticides, and later of
organophosphorus and other types of insecticides, provided new weapons against
the vectors of disease.� Improved
molluscicides strengthened the control of schistosomiasis.� The development of a safe and effective
yellow fever vaccine has had so striking an effect that yellow fever-once the
scourge of Africa-is now a comparative��
rarity there.��
Antibiotics, curative�� in so many diseases, reduced the incidence
of yaws to a manageable proportion in many areas. But these 'wonder�� drugs'��
and pesticides were soon to show their limitations. Resistance of
parasites and vectors developed in a number of areas, but fortunately many of
these drugs and pesticides were replaced by newer discoveries. The application
of the newer measures was, furthermore, beset by formidable difficulties,
logistic, sociological and financial, so that the general eradication of
insect-borne disease in rural areas of Africa is not yet in sight.
Meanwhile, the human element, as
one might expect, dominated much of the scene.�
Industrialization�� and
urbanization, already referred to, played an increasing part. The rapid
development of the great mining areas in Kimberley and the Rand had brought
workers from many parts of Africa. Other developments in West and East Africa
brought their own problems.� The copper
mines in Zambia needed measures to combat occupational disease. Fortunately,
where mining activities were adequately controlled, such organizations�� as the Silicosis Bureau and the arrangements
for regular examination of labourers dealt adequately with such occupational
diseases and their consequences and they have been reduced to appreciably low
proportions.
Soon after World War II the drive
for independence in the African countries took on a new momentum.� When these countries achieved their
independence one by one, they were left with a great legacy of highly efficient
medical and public health organization, built on the western pattern and with
the machinery ready to take over. But machinery is not enough:� once again the human element is paramount.� All those in the medical services, expatriate
and indigenous, had been largely trained in the ways of western medicine: but
few had been trained to the quite specific needs of medicine in Africa, their
priorities and the best ways in which to apply them. It became apparent and much
recent writing has supported this-that much training for medicine in Africa
should be carried out in Africa and that until education is much more
widespread the number of conventionally trained doctors cannot hope to deal single
handed with the vast health problems of rural Africa. The standards of medical
qualification must not be reduced:� but
the emphasis needs to be put on the specific problems to be faced in rural
Africa.� Much groundwork remains to be
done in health education, by 'selling' to the people the needs for health and
above all to show them how to apply the basic measures themselves. Much of this
can best be done in the field through the influence of Africans themselves, who
can translate the concepts of modern science in terms which their people can
understand; and this should be encouraged throughout the social scale from the
Medical Officer of Health to the Village Headman. Fortunately, in many
countries facilities for training are being developed in increasing
numbers.�
Meanwhile, the goal must be the
eventual application of full scientific measures, the increasing education of
fully qualified doctors, adapted where necessary to local needs, but with the
use of every discipline which modem science has to offer: and this implies not
just medical science but sociology, psychology and all those approaches necessary
to meet in a humanitarian way the cultural needs of the people concerned.� The first priority is not for expensive
equipment: it is for enlightened doctors. Fortunately, research is not lacking
and indeed in many parts of Africa has reached a high state of maturity.� One can but look, for example, at such
agencies originally formed, as the East and West African Councils for Medical
Research, the East African Medical Survey, the East African Tsetse and
Trypanosomiasis Research and Reclamation Organization, the Viral Research
Institutes in Entebbe and Lagos, the West African Institute for Trypanosomiasis
Research and numerous other institutions, committees and research laboratories
either former or existing. Many pilot schemes on the control of diseases in
various parts of Africa have pointed the way to wider measures.
The many developments medicine in
Africa have achieved some remarkable results and indeed some of the projects
undertaken are themselves classics in the history of tropical health.� A few examples may give some indication of
the compass of some of these undertakings. One was the introduction of sleeping
sickness settlements in East Africa associated so closely with the name of
George MacLean, though it eventually involved a tremendous combined operation
of many disciplines and agencies. The basic concept was that in bush country infested
with tsetse flies in Tanganyika where Trypanosoma rhodesiense infection
occurred there were some natural clearings unattractive to the fly and with
relatively small populations.�
The purpose of the scheme was to
enlarge those areas and to transfer to those new clearings people from villages
in bush areas which were infested with tsetse flies. This meant a complete
change of their way of life and the development of a new environment which
would embrace all the necessities for the growth of self-supporting
communities. This was resettlement on a vast scale, with provision of water
supplies, dwellings, farm animals and the development of crops. Whole
communities were thus separated from tsetse flies and hence from infection with
sleeping sickness. A similar system was also applied in country of a different
kind such as that adjacent to rivers and lakes where T. gambiense was the
parasite, and various methods of approach were carried out in other parts of
East and West Africa.
In West Africa a system of selective
clearing was introduced, and it was in Nigeria that a classical undertaking was
made in resettlement and formation of thriving communities in an area heavily
infected with T. gambiense sleeping sickness. This was in the Anchau area where
a scheme was undertaken to control the vector flies in a corridor of some 70 x
10 miles.t" This ultimately resulted in the disappearance of trypanosomiasis�� in man and animals and the people themselves
maintained the area which they had cleared.
Both of these enterprises called
for closely planned and executed operations not only by the medical department,
but by administrative, veterinary and agricultural departments. This underlines
what cannot be repeated too often regarding public health advances in Africa,
namely that it is not just a departmental problem, but one which involves close
consultation and activity between all the agencies and disciplines which
contribute to the full development of the African in his environment.
Brief reference may be made to
two other projects which illustrate the need to foresee the implications for
community health in the undertaking of large-scale industrial schemes in Africa
and the hazards of man-made obstacles to health. The Volta River hydro-electric
scheme in Ghana posed many problems, not the least of which was the settlement
and protection of people from disease resulting from flood. Measures had to be
taken to deal with such conditions as malaria, ankylostomiasis, and
schistosomiasis, and this involved careful planning and execution by the health
authorities. The construction of the Kariba Dam in the Zambesi Valley raised
comparable problems and a comprehensive medical organization was developed to
deal with them. Detailed accounts of these approaches have been written and
would repay reading.
It is clear from the foregoing
that clinical medicine, while it must always have its proper compassionate
place in relieving individual suffering in Africa, should develop hand in hand
with increasing preventive efforts. It is curious that in western countries the
greatest advances in therapeutics have occurred in the last half century, while
preventive medicine was already taking shape in the Victorian era. In tropical
Africa the position was, in a sense, reversed.�
The first gropings after the control of tropical diseases were based on
the use of such drugs and empiric treatments as were available, but the concept
of prevention had to await the newer knowledge of transmission of disease and
of its control. It is true that the prophylactic use of some of the newer drugs
may be the only means, by reason of limited communications, men and money, for
mass prevention of a number of diseases in rural areas of Africa.� But in others wider preventive measures,
whether against diseases, vectors or ignorance, are the means in which
increasing hope must be placed in the future.
In the development of medicine in
Africa from scientific ignorance to organized community health the groundwork
is sound and the pattern clear and flexible enough to be adapted to various
local needs: yet it must be repeated that however well organized the practical
measures, the future must depend on increasing education of the people
themselves. The problems are basically African problems and their solutions
must ultimately rest with trained Africans at increasing levels of general,
health and medical education.� For some
time to come many developing countries will need expert outside help and
guidance in solving their medical problems.�
Such is already available through links with some British universities
and other institutions who second staff to the needy countries, and by
fellowships and other forms of aid enabling experts to spend periods in some of
the former British African Territories to help in ad hoc projects or in an
advisory capacity. In time, the Africans will take over completely themselves;
but whatever form their medical facilities may take, the objectives will be the
same-to pursue war on what President Nyerere of Tanzania succinctly described
as 'poverty, ignorance and disease?� so
that the peoples of Africa may be capable of leading full and healthy lives,
free from the hazards which decimated their forefathers and many of those, too,
who went to Africa to help them. To this objective Commonwealth Medicine has
been proud to contribute in the past and is proud to continue to
contribute�� in the interim in that
tradition so well summarized in the motto of the Royal Society of Tropical
Medicine and Hygiene, Zonae torridae tutamen.
(back
to content)
1.2.1
Mesopotamian c
Medicine in Assyria and Babylonia
was influenced by demonology and magical practices. Surprisingly accurate
terra-cotta models of the liver, then considered the seat of the soul, indicate
the importance attached to the study of that organ in determining the
intentions of the gods. Dreams also were studied to learn the gods' intentions.
While magic played a role in
healing, surviving cuneiform tablets indicate a surprisingly empirical approach
to some diseases. The tablets present an extensive series of medical case
histories, indicating a large number of medical remedies were used in
Mesopotamia, including more than 500 drugs made from plants, trees, roots,
seeds, and minerals. Emollient enemas were given to reduce inflammation;
massage was performed to ease gastric pain; the need for rest and quiet was
stressed for some diseases; and some attention was paid to diet. Water was
regarded as particularly important, since it was the sacred element of the god
Ea, the chief among the numerous healing gods. The serpent Sachan was also
venerated as a medical deity.
1.2.2 Israeli/ Palestinian c
Hebrew medicine was mostly
influenced by contact with Mesopotamian medicine during the Assyrian and
Babylonian captivities. Disease was considered evidence of the wrath of God.
The priesthood acquired the responsibility for compiling hygienic regulations,
and the status of the midwife as an assistant in childbirth was clearly
defined. Although the Old Testament contains a few references to diseases
caused by the intrusion of spirits, the tone of biblical medicine is modern in
its marked emphasis on preventing disease. The Book of Leviticus includes
precise instructions on such varied subjects as feminine hygiene, segregation
of the sick, and cleaning of materials capable of harboring and transmitting
disease. Although circumcision, the surgical removal of the foreskin on the
male�s penis, is the only surgical procedure clearly described in the Bible,
common medical practices include wounds dressed with oil, wine, and balsam. The
leprosy so frequently mentioned in the Bible is now believed to have embraced
many skin diseases, including psoriasis.
(back
to content)
1.2.2.1 Thalassotherapy w
Thalassotherapy (from the Greek
word thalassa, meaning "sea") is the use of seawater as a form of
therapy. It also includes the systematic use of sea products and shore climate.
There is no scientific evidence that thalassotherapy is effective.
Some claims are made that
thalassotherapy was developed in seaside towns in Brittany, France during the
19th century. A particularly prominent practitioner from this era was Dr.
Richard Russell, whose efforts have been credited with playing a role in the
populist "sea side mania of the second half of the eighteenth
century", although broader social movements were also at play. In P�voa de
Varzim, Portugal, an area believed to have high concentrations of iodine due to
kelp forests, and subject to sea fog, the practice is in historical records since
1725 and was started by Benedictine monks; it expanded to farmers shortly
after. In the 19th century, heated saltwater public baths opened and became
especially popular with higher classes.
Others claim that the practice of
thalassotherapy is older: "The origins of thermal baths and related
treatments can be traced back to remote antiquity. Romans were firm believers
in the virtues of thermalism and thalassotherapy.
(back
to content)
1.2.3 Chinese Medicine m
The earliest Chinese medicine, in
common with most other ancient civilizations, assumed disease and illness were
caused by the gods or by demons. The correct remedies for illness involved
ritual exorcisms and appeals to the Gods.
A more naturalistic explanation
of illness developed with the belief in Yin and Yang. The Yin and Yang
principles were considered to control everything and their interaction
controlled the functioning of the human body. Yin was feminine, soft, cold,
moist, receptive, dark, and associated with water, while Yang was masculine,
dry, hot, creative, bright, and associated with fire. Human health depended on
a balance between Yin and Yang. Further factors effecting disease were wind,
rain, twilight and brightness of day so there was a total of six disease making
influences. Any of these six influences could upset the balance of Qi, which
was a vital spirit similar to breath or air, which existed throughout the human
body.
Chinese knowledge of anatomy was
very limited due to a strict prohibition on the dissection of the human body.
Chinese belief concerning the inner organs was largely erroneous. They believed
there were five �firm� organs that acted as receiving organs and lay opposite
five �hollow� organs who served the purpose of evacuation. The firm organs were
the heart, spleen, lungs, liver and kidneys. The heart was considered to be the
place of wisdom and judgment while the liver and the lungs were associated with
the soul. The male�s right kidney was seen as the source of sperm and its
connection with the passage of urine was not understood. The hollow organs were
the bladder, gall bladder, colon, small intestine and the stomach.
Chinese doctors attempted to make
a diagnosis by studying the state of the pulse. This practice known as
sphygmology involved attempting to recognize some very subtle variations in the
pulse. There were considered to be 51 different varieties of pulse which were
to be taken in 11 different areas of the body. Chinese doctors were attempting
to obtain far more information from the pulse, than it could possibly provide.
Acupuncture, aimed to restore the
balance of Yin and Yang, and involved inserting needles into particular parts
of the body. There were 388 areas of the body into which the needles could be
inserted and they needed to be inserted at the correct time, based upon the
weather, the time of day and the phases of the moon. The needles were left in
anything from five to fifteen minutes. Acupuncture does appear to be effective
for pain relief as the needles seem to make the body produce endorphins, the
body�s own natural painkillers. Claims have been made that acupuncture can cure
many diseases including muscle, bone, respiratory and digestive disorders.� A further Chinese treatment was Moxa which
involved inflicting a slight burn on the skin. It was considered to be a
treatment for a vast range of complaints such as diarrhoea, abdominal pains,
anaemia, vertigo, nose bleeding, gout, toothaches and headaches.
1.2.3.1 Traditional
Chinese Medicine - an Overview p
Background: Traditional Chinese
medicine, which is the basis of the Chinese culture heritage, has a long
history of 5000 years and it has significantly contributed to the survival of
their nation and its prosperity. Over time, various theories have been
systematized and developed in order to maintain and improve the health of the
Chinese population. Objective: The objectives of the paper are: a) to present
the historical development of traditional Chinese medicine, b) to explain the
basic principles on which traditional Chinese medicine is based on and c) the
basic methods of treatment and most common herbal remedies used in traditional
Chinese medicine. Methods: The paper is of descriptive nature, and numerous and
informative literature was used for its writing, mainly texts from books and
articles published in indexed journals retrieved from the world online
databases. Results and Discussion: The first records of traditional Chinese
medicine date back to the Huang Di period, and the first record is from a book
called NeiJing and it represents the theoretical foundation of traditional
Chinese medicine.
Over thousands of years, progress
has been made in this area and numerous dynasties have invested resources and
knowledge to maintain and develop it. The Han Dynasty and the Tang Dynasty
produced some of the best physicians and connoisseurs of traditional medicine,
and the Ming Dynasty contributed perhaps most of all. Immediately after the end
of the Opium Wars, the Western world evaluated traditional Chinese medicine as
a feudal and scientifically unproven method. Since then, the Chinese
authorities have focused on preserving the integrity of their traditional
medicine, and at the end of the 20th century, the World Health Organization
accepted traditional Chinese medicine as a scientifically based method of
treatment and gave it the name Complementary Medicine. The theory of Chinese
traditional medicine is based on several principles: qi theory, the concept of
yin-yang, the theory of the five elements, the concept of zang-fu organs, and
the theory of meridians and parallels. Conclusion: Traditional Chinese medicine
has made a significant contribution to the development of modern medicine
during its long history, as well as one of its most difficult and complicated
aspects the acupuncture, which requires extensive knowledge of all concepts of
traditional Chinese medicine and perfect precision.
1. BACKGROUND
History is full of mythology in
the case of the Three Kings of Heaven who are revered as the founders of
Chinese civilization. Fu Hsi, for who is believed to have ruled 2000 years
before Christ, is the legendary founder of the first Chinese dynasty. His most
important inventions included writing, painting, music, original mythical
trigrams, and the yin-yang concept. Both the Ching or Rule of Change that is
respected as one of the oldest Chinese books has been attributed to Fu Hsi.
The invention of key agricultural
and farming techniques has been attributed to Shen Nung, another Heavenly
Emperor. When the emperor, who is also known as the Divine Peasant, saw that
his people were suffering from disease and poisoning he taught them to sow five
kinds of grain and he personally studied thousands of plants so that people
know which are medicinal and which are poisonous. In his experiments with
poisons and antidotes, Shen Nung tried as many as seventy different poisons in
one day. After collecting many drugs in the first major study of herbal
medicine and after presenting a magnificent example of selfless devotion to
medical research, Shen Nung died after a failed experiment. During a century of
rule, Huang Ti, the last of the three legendary Heavenly Emperors, gave his
people a wheel, a magnet, an observatory, a calendar, the art of measuring
heart rate, and the Huang-ti Nei Ching (Yellow Emperor�s Canon of Internal
Medicine) �a text that inspired and guided Chinese medical thought over 2500
years. Like many ancient texts, the Nei Ching has been corrupted over the
centuries with additions, cutouts, and typographical errors. Scholars agree
that the existing text is very old, perhaps even dating back to the first
century BC, but the time of its compilation is polemical.
Most historians believe that the
existing text was composed at the beginning of the T�ang dynasty (618- 907).
Other medical texts have once overshadowed it but most of the classics of
Chinese medicine can be considered an interpretation, commentary, and
supplement to the Yellow Emperor�s Code (CANON). Although the Inner Canon is
appraised as one of the oldest and most influential texts of classical Chinese
medicine, studies of medical manuscripts that were buried with their owners,
probably during the second century BC, and found in Mawangda, Hunan in the
1970s provided a new insight into early Chinese medical thought. As the newly
discovered texts are analyzed, scholars are beginning to understand the
philosophical foundations of Chinese medicine and the ways in which educated
physicians from the fourth to the first century BC managed to distance
themselves from shamans and other folk healers. Physicians were apparently
still researching approaches in psychology, pathology, and therapy that
differed from those found in the Inner Canon (text). Therapists in older texts
included medical drugs, exorcism, magical and religious techniques, and
surgical procedures, but acupuncture, the main therapeutic technique in the
Inner Canon, is not described in the Mawangdui manuscripts.
2. OBJECTIVE
The objectives of the paper are:
a) to present the historical development of traditional Chinese medicine, b) to
explain the basic principles on which traditional Chinese medicine is based on
and c) the basic methods of treatment and most common herbal remedies used in
traditional Chinese medicine.
3. METHODS
To write this paper, we used the
scientific literature from articles that are stored in scientific databases and
available by the Internet, and represent a reliable source.
Books stored in libraries in the
Sarajevo Canton were also used as a source for writing the article, most of
which were found in the National and University Library in Sarajevo.
Among them are books: Liu Z, Liu
L. Essentials of Chinese medicine. Vol. 1. Springer. 2009; Lloyd J. U. Origin
and history of all the pharmacopeial vegetable drugs, chemicals and
preparations with bibliography. Read Books; 2008;
Gurley B, Wang P, Gardner S.
Ephedrine-type alkaloid content of nutritional supplements containing Ephedra
sinica (Ma-huang) as determined by high performance liquid chromatography. J
Pharm Sci 1998; 87: 1547-1553. Used articles are quite recent and have been
published in indexed journals, which means that their content is verified and
reliable. In order to write a part of the paper on medicinal plants that
traditionally originate from China, these books were used: Kovačević
N., entitled �Fundamentals of Pharmacognosy� and the book �History of Medicine�
by Magner LN. which is stored in the library of pharmaceutical company
Bosnalijek Sarajevo. The book is of high quality and it offers a variety of
content on the development of medicine and pharmacy over their long history.
This paper also contains numerous
illustrations that complement the quality presentation of Traditional Chinese
Medicine and their sources are cited in the legends below the figures (1-22).
4. RESULTS
The history of traditional
Chinese medicine
The first records on Traditional
Chinese Medicine (TCM) date back to 5000 years ago. The TCM encompasses Han
medicine, as well as the theories and practices of various national minorities
from China such as Miao, Dai, Mongols and Tibetans. The first records of TCM
appear from the period 2698-2598 BC, during the era of Huangdi or the Yellow
Emperor. However, the duties and responsibilities of physicians were defined
only later, in 1122
�
Figure 1. Bian Que�the oldest known physician from the area
of today�s China and author of the Bian Que Neijing book dedicated to
traditional Chinese medicine Available at:
https://upload.wikimedia.org/wikipedia/commons/e/e0/Chinese_woodcut%2C_Famous_medical_figures%3B_Portrait_of_Bian_Que_Wellcome_L0039317.jpg.
Accessed: March 9, 2017.
�
Figure 2. Paragraph from The Neijing, first part (Su Wen).
Available at:
https://en.wikipedia.org/w/index.php?title=File:The_Su_Wen_of_the_Huangdi_Neijing.djvu&page=3
Accessed: March 9, 2017.
BC, during the Zhou dynasty. At
the time, every large estate had its own physician, and it was characteristic
that physicians were paid when the householders were healthy, not when they
would get ill. Thus, the primary concern of physicians was maintaining health
and preventing disease, not treatment. TCM is the oldest continuously
practiced, scientific medical system in the world. It certainly should not be
classified as a term of folk medicine, nor quackery, because TCM is a complex
and precise health care system created from the efforts of great Chinese minds
to understand the secrets of the functioning of the human body (3). In its
beginnings, TCM was a practical and effective art based on observations and
experience with the application of philosophical principles such as Yin and
Yang or wu-xing (the theory of the five elements).
The basic thinking was that
health can be maintained if there is a balance of the human body with the inner
spirit and the outer environment. For this reason, diagnosis and treatment were
based on finding of disbalance and its return to normal state.
One of the oldest physicians is
Bian Que (Figure 1) or Qin Yueren of Hebei Province who lived in 500 BC. He was
known as an excellent diagnostician with excellent pulse examination and
acupuncture therapy skills. According to historical records, he is the author
of the Bian Que Neijing book used during the Han Dynasty. Unfortunately, the
book wasn�t preserved.
However, the publication of The
Neijing (Canon of Internal Medicine of the Yellow Emperor) is the most
significant book on TCM, which established the theoretical foundations of the
medical system itself and philosophical theory. The writing of this book took
hundreds of years, all the way from 770 to 221 BC. Astronomical and
geographical observations, as well as theories about the existence of the human
being, medicine, science, culture and philosophy can be found in the book. The
book consists of two parts: Su Wen and Ling Shu. The first part of the book
deals with the general principles of health and standard methods of diagnosis
and treatment, and the second part is more specialist-oriented on the art of
acupuncture and moxibustion (Figure 2).
The Han dynasty (206 BC to 220
AD) is considered one of the most important dynasties for the development of
TCM and was marked by physicians such as Zhang Zhongjing and Hua Tuo.
Hua Tuo (Figure 3) was born in
Anhui Province and is one of the most famous physicians of ancient China and
one of the first known surgeons in China. Hua Tuo is known for being the first
to invent anesthesia and deepen his knowledge of human anatomy. Practicing
acupuncture and herbal remedies, he used simple methods using a small number of
acupuncture points and prepared herbal remedies with simple herbal formulas. He
was a practitioner of Qi Gong and invented the theory of five animals that is
still used today (tiger, deer, bear, monkey and crane).
Even as a child, Hua Tuo lost his father and had to
find a job. The fate was such that he was employed in a local herbal pharmacy.
While working there, he carefully observed the practice of the physicians at
the time. At a time when Hua Tuo was growing up, there was turbulent political
turmoil and constant fighting. He was not a member of the army or an elite
citizen, but he was spending time with the poor and dedicated his life to
helping them, so he was also known as the �folk physician�. He soon became very
famous, but despite the offer to become the king�s personal physician, he
refused the offer. Hua Tuo was known that if the cause of the disease could not
be removed with acupuncture or herbs, the only solution was to surgically
remove the cause.
It is documented that Hua Tuo
used the Figure 2. Paragraph from The Neijing, first part (Su Wen). Available
at: https://en.wikipedia.org/w/index.php?title=File:The_Su_Wen_of_the_Huangdi_Neijing.djvu&page=3
Accessed: March 9, 2017.
�
Figure 3. Hua Tuo and illustration of performing a surgery on a
patient.
Available at:
http://www.acupuncturetoday.com/mpacms/at/article.php?id=31781.
Accessed: March 11, 2017.
so-called Ma Fei San herbal
formula in patients which had the effects of anesthesia and then performed
surgery. One of the problems Hua Tuo noticed was that there were always a lot
of sick people, more than he could cure. Therefore, he devised the Wu Qin Xi
theory (the theory of five animals) which basically provided instructions on
physical exercises, and which imitated the movements of a tiger, deer, monkey,
bear, and crane. Unfortunately, as with most geniuses and influential
historical figures, Hua Tuo ended his life in prison with the death penalty.
Cao Cao, the ruler of the Wei kingdom, had severe headaches, presumably a
migraine, which Hua Tuo first cured with simple acupuncture. However, Hua Tuo
refused to stay in the castle and returned to his sick wife and people. Not
long after, Cao Cao brought him back to his court and forbade him to leave it.
The problem was that it was no longer possible to cure migraines with herbs or
acupuncture, so Hua Tuo suggested surgery and surgical removal of the cause.
Cao Cao considered it an attempted murder and sentenced him to death. During
his captivity, he transferred all his knowledge to paper, but the guards did
not want to preserve his works, so it was all lost along with him.
On the other hand, Zhang Zhongjing
(Figure 4) is the most famous physician of all time in China and is considered
a holy figure in medicine, something like Hippocrates in Western medicine. He
wrote a work called Shang Han Za Bing Lun (treatment of febrile illnesses and
various diseases) which contained over 100 effective formulas that are still
used today. Zhang introduced such a system that the treatment was carried out
on the basis of the differentiation of the syndrome in the patients.
�
Figure 4. Zhang Zhongjing � Chinese ancient doctor who is
considered the most important physician from the ancient era (150 � 219 AD).
Available at:
https://www.britannica.com/biography/Zhang-Zhongjing.
Accessed: March 11, 2017.
Unfortunately, due to various political turmoil and numerous
battles, very little historical data about his life has been preserved.
Not long after, during the
Jin-Yuan dynasty, the theories of TCM were further developed and advanced with
the establishment of four branches of TCM. Liu Wansu found the so-called
cooling school where the basic principle was treatment with herbs that cause a
feeling of cooling in patients. Zhang Zhihe found a school of �attack� based on
the use of diaphoretics, emetics and purgatives to attack pathogens and expel
them from the body. Li Dongyuan advocated a theory that focused on all diseases
being caused by damage to the stomach/spleen, most commonly caused by
uncoordinated eating, drinking, work, or seven excessive emotions. Ultimately,
Zhu Danxi was a devotee of preparing various tonics, especially those that
cleansed the kidneys and liver. He believed that people get sick because they
enjoy the pleasures and immoral things in this world too much which would upset
the balance of yin.
The greatest success and
development of TCM was experienced during the Ming Dynasty (1368-1644),
culminating in the publication of the Compendium of Material Medica (Figure 5)
by Li Shizhen. Li Shizhen dedicated himself to gathering the most important and
credible medical experiences over 30 years and singled out a total of 1,094
herbal medicines, 443 animal medicines and 354 mineral medicines. For each
drug, an adequate name, source, form and medical history were prescribed, as
well as the manner in which it was collected, prepared, stored and dosed.
The basics of Traditional Chinese
Medicine Modern TCM theory has emerged from the naturalistic philosophies of
ancient China with special influences of experiences that have accumulated
through generations and generations. TCM may seem outdated and charlatan today,
but it is a complete, integrated method of interpreting human physiology and
pathological changes in the body. The most important concepts of TCM are qi,
yinyang and the theory of the five elements (wuxing). Theoretical concepts of
specific TCM include the doctrine of zheng ti guang nian, the concepts of
viscera and compassion (zangfu xue shuo), channels and networks (jingluo),
bodily substances (qi, blood, essence and body fluids qi xue jing jinye) and
pathological agents (bing yin). All these theories, together with the
methodologies of the four methods (si zhen) and basic discrimination (bian
zheng) form the theoretical basis of TCM. Each of the therapeutic methods of
TCM, such as acupuncture and moxibustion (zhenjiu), Chinese herbology (zhongyao
fang), and Chinese therapeutic massage (zhongyi tuina) are based on the above
mentioned theoretical foundations.
Concept of Qi theory The basic
concept of qi theory is that qi is the basic substance from which the entire
universe is built and that all objects in the universe are born by the
transformation of qi. Ancient philosophers argued that qi could exist in two
states: dispersion and condensation, and these two states�
Figure 5. Fragment from the book Compendium of Material
Medica which was written by Li Shizhen. Available at:
https://commons.wikimedia.org/wiki/
File: Compendium_of_Materia_Medica_2.jpg.
Accessed: March 12, 2017.
of qi determine two modes of
perception in human: one having a form and one without a form. When qi is in a
state of dispersion then we speak about a state without form. It is a state
that does not occupy any limited space and does not possess a definite and
stable form. In contrast, when it is in a state of condensation then it
possesses its own form or shape. In this state it can occupy a limited space
and possess the final and stable form of any of the objects. The most
interesting thing is that qi can pass from one state to another to infinity.
From a medical point of view, qi is a substance that permeates the human body
and they together form one whole. Chi is considered the basic substance of the
human body and once it is in a dispersed state�the body dies. Something in line
with the yin-yang theory, which will be explained later, there are two types of
qi�Yang qi and Yin qi. Yang qi is described as lightness, purity, activity and
warmth, while Yin qi is just the opposite. Therefore, the celestial vault is
composed of Yang Chi, while the earth is formed of Yin Chi, and their
combination and unification created all living and non-living matter on Earth,
including humans, animals and plants. The fact that every living matter in the
world is different from each other is the result of a different combination of
the two types of qi.
According to the qi concept,
there are two types of change in the universe. One type of change is
quantitative and it is difficult to notice and occurs gradually and is only
measured quantitatively, not qualitatively. The second change is qualitative
and it occurs when the quantitative change has reached its maximum and then
there is a transmutation of one thing into another. All of this can be related
to TCM because it combines the effects of seasonal changes on the vital
activities of the human body.
In addition, TCM attaches great
importance to the diversity and specificity of geographical locations and
orientations, which is in line with one of the most difficult relationships to
explain, and that is the relationship between space and time and the principles
of dynamic change in the universe.
The concept of Yin-Yang According
to ancient Chinese philosophy, yin and yang represent two essentially opposite
categories. At first, their understanding was simple, describing the turning of
the face or back to sunlight. It was later introduced into the theory that yin
and yang refer to almost all imaginable opposites, such as time, position, side
of the world, state, etc. Ancient Chinese philosophers wisely observed that for
every phenomenon there are two opposing aspects with each other. Thus, yang is
represented by phenomena such as speech, active state, external, upper, warm,
light, while yin is associated with opposite phenomena: silence, inactive
state, internal, lower, cold, dark (Figure 6).
Yin and yang theory have four fundamental foundations, known
as the four relations of yin yang:
� opposition,
� interdependence and coherence,
� intermediate consumption and support and
� intertransformation.
As already stated, yin yang
theory is used to describe a universal qualitative standard. One of the basic
aspects is certainly yin which exists as the very opposite of yang. Heaven and
earth, sun and moon, night and day, inside and outside are manifestations of
the dual intrinsics of the universe.
In the context of medicine, the
upper body is yang, and it is related to the lower body which is yin. However,
the front of the body is yin, while the back of the body is yang. Likewise, the
medial part of the body is yin and the lateral part is yang. Most importantly,
the inner part of the body represents yin, while the outer part is yang. Inside
the yin, or inside the body, there are so-called zang organs (called viscera)
and which are considered solid and belong to yin, while fu organs belong to
yang. Diseases that manifest with symptoms such as fever or excessive metabolic
activity belong to yang, while the opposite is yin. The fast and short pulse is
yang, while the slow and long pulse is yin (Table 1).
Since yin and yang form one
whole, they are also interdependent. The whole is defined by the existence of
two opposites such as fire and water, hot and cold, interior and exterior. In
the field of medicine this can be seen in the relationship of structure and
function. The structure is in any case yin, while the function is yang. A
sufficient amount of the substance (structure) in the form of, for example,
body fluid, healthy tissue, etc., enables the normal function of the organism.
Only when the process is functional can adequate recovery occur and such a
balance between structure and function is the basis of healthy��
Table 1. Basics of yin yang
opposites that are used in Traditional Chinese Medicine
�
Figure 7. Five primary elements in Traditional Chinese
Medicine and their connection.
Available at:
http://www.springer.com/cda/content/document/cda_downloaddocument/9781461452744-c1.pdf?SGWID=0-0-45-1415302-p174674052.
Accessed: March 18, 2017.
functional activity. Interaction
and connection are another aspect of yin yang. There is no phenomenon, event or
situation that can be described as complete yin or complete yang. Every phenomenon
in the university has yin and yang aspects, depending on the angle from which
the situation is viewed. For example, day is considered yang when compared to
night, but the first hours of the day (before noon) are yang compared to the
hours after noon, which are yin.
So, in China it is said that
morning is yang with yang, and afternoon is yin with yang. Every phenomenon can
be brought to infinity in this manner.
Inter-consumption and support are
also an integral part of yin yang. Growth, development and progress in one
aspect means setback in another aspect. Under normal circumstances,
consumption/support occurs within certain limits. In the context of physiology,
this phenomenon may be associated with homeostasis. Exceeding these limits
results in organ dysfunction and disease. If yang disorder occurs, e.g.,
increased metabolic activity, yin resources are consumed. Conversely, aging
(yin) can lead to a drastic reduction in bodily functions (yang). In
pathological terms, all diseases have four causes: yang or yin excess, yang or
yin deficiency.
Another characteristic is
intertransformation. From a medical point of view, this can happen in two ways:
harmoniously, as a natural course of development, aging and death, or
inconsistently due to drastic changes in the environment or internal imbalance.
Thus, Chinese physicians claimed that when yin is extremely pronounced, at some
point it will turn into yang. Such a case can be seen when high fever (yang
disorder) leads to shock and the onset of hypothermia and loss of
consciousness, which in turn are yin symptoms.
Theory of five elements (wuxing)
The theory of the five
elements/phases establishes such a system of correspondence that all phenomena
in the universe can be classified into five categories. The categories
represent a tendency to move and transform in the universe and are related to
natural phenomena such as wood (mu), fire (huo), earth (tu), metal (yin) and
water (shui). A constant correlation between them is used to explain changes in
nature (Figure 7).
Each of the categories/elements
represents a category of certain functions and qualities. The wood is
associated with spring, flowering, growth, awakening, morning, childhood, anger
and wind. Fire, on the other hand, is associated with summer and represents a
state of maximum activity, accelerated growth, noon, excessive happiness and an
open flame. The earth is associated with the end of summer, i.e. the transition
to autumn. It represents balance and equilibrium, early afternoon, refreshment,
anxiety and moisture. The metal is associated with autumn, reduced functions,
movement towards crystallization, clarity, sadness and no precipitation. As for
water, it is related to winter, state of decay, accumulation, rest, night and
possible development of new potential, concentration of will and fear and cold.
This categorization can be applied in China to colors, sounds, smells, tastes,
emotions, animals, planets, and almost everything in the universe (Table 2).
All five elements are interconnected by fixed connections.
There are two connections between
them, and they are sheng and ke connections. Both connections are natural and
necessary. Sheng is an incentive, and ke is a control.
Sheng is a connection where one
element gives rise to another. Thus, for example, wood stimulates fire, and
fire stimulates earth, earth stimulates metal and metal stimulates water, while
water stimulates wood. The circle is
�
Table 2. Relationships of five
elements and their corresponding states also known as the mother-son
relationship, with the stimulus phase acting as the mother for the next. There
is also a circle through which the elements control each other, so wood
controls the earth, earth controls water, water fires, fire metal and metal
controls wood.
The five-element theory is
directly related to the zang and fu viscera, and to the acupuncture channels
that are classified in this manner. The theory of the five elements is also
used to interpret the physiology and pathology of the human body and its
connection with the natural environment.
Thus, the five-element theory is
related to etiology, diagnosis, treatment, and prognosis.
The most important statement of
the five-element theory is related to the zang organs: the tree represents the
liver, which regulates the free flow of qi; fire represents the heart which
provides heat to the whole body; the earth represents the spleen which is in
charge of transporting and transforming food; metal represents the lungs that
allow the relief of qi; water represents the kidneys that are in charge of
storing the essence and regulating body fluids. Given that it has already been
said that the elements encourage and control each other, this can be explained
in this way:
� Wood stimulates fire: all the blood flows through the
liver and directs it to the heart so that the heart can regulate its flow;
� Fire stimulates the earth: the heart gives the heat
necessary for the proper functioning of the spleen;
� Earth stimulates the metal: the spleen transforms and
transports essential nutrients and sends them to the lungs so that it can
regenerate and support their activity;
� Metal stimulates water: the lungs send yin fluid to the
kidneys;
� Water stimulates the tree: the essence of the kidneys
renews the blood that goes further to the liver;
� Wood controls the soil: the cleansing effect of the liver
prevents the spleen qi from stagnating;
� Fire controls the metal: the heartbeat prevents the lungs
from being reduced to a minimum;
� Earth controls water: transport through the spleen
prevents excessive fluid flow through the kidneys;
� Metal controls the wood: cleansing through the lungs
allows less load on the liver�s qi;
� Water controls fire: the flow of yin through the kidneys
alleviates the yin of the heart.
Visceral Zang and Fu theory
In traditional Chinese medicine, most human organs are
divided into two groups: five zang and six fu organs.
The five zang organs are the
heart, liver, spleen, lungs and kidneys, which are the most important organs in
the human body. The six fu organs are the gall bladder, stomach, small and
large intestine, bladder, and san jiao, all of which are important for the role
of transporting and processing food and water.
The physiological functions of
the heart were taken to control blood flow through blood vessels, support the
mind, and control the tongue. It is a completely logical explanation of the
role of the heart in circulation, and it was believed that the physiological
function of the heart could affect the very mind of a human. Also, the tongue
is connected to the heart by the cardiac meridian, so through this connection
it is considered that the heart dominates the sense of taste on the tongue, but
also speech, so it was believed that heart disease must manifest on the tongue.
The lungs played a basic role in
respiration, controlling the decline and dispersion of qi, supporting the skin
and hair, communicating with the throat and nasal openings, and are
meridian-related to the colon. The lungs are a very important organ in TCM
because they exchange qi that comes from outside and inside, and thus control
the complete qi in the human body. Lung dysfunction can lead to qi disorders
and cough or dyspnea.
The spleen is located in the
so-called. medium energizer.
Its basic physiological function
is the transport and transformation of water and food, and the control of blood
and the maintenance of its normal circulation and the nutrition of muscles and
four extremities. The spleen is connected to the lips and their condition
reflects the condition of the spleen.
The liver is located in the right
hypochondriac region and its main function is to store and regulate blood,
support the free flow of qi, control tendons and open the eyes.
Changes in the state of the liver
are associated with emotional changes such as depression or excitement. The
condition of the liver in traditional Chinese medicine was reflected through
the condition of the eyes since the liver was thought to nurture eye health
through blood circulation.
The main role of the kidneys was
to store congenital and acquired essence and control of human reproduction,
regulate water distribution, receive qi as an assistant to the lungs,
which�

represents their direct
connection (lungs and kidneys). The condition of the kidneys was reflected in
the physiological preservation of hearing, i.e. the ears, because it was
considered that the kidneys, with their chi, nurture hearing and ears.
The gall bladder was considered
to be directly related to the liver and the dysfunction in the physiological
functions of the gall was thought to be reflected in changes in taste on the
tongue i.e. an increased sense of bitterness.
Changes in emotional states
associated with the liver are also associated with gall.
The stomach is considered the
central organ of digestion and is directly connected to the gall bladder. Its
basic physiological functions are food and water storage, appetite control and
pain in the epigastric region. The optimal qi of the abdomen controls all five
zang organs, so they will be filled with energy, and in the case of disturbed
qi, the weakness of the same will be felt.
The small and large intestines
are located in the lower part of the abdomen, and their role is the final
digestion of food and the absorption of nutritional elements, i.e. the uptake
of waste products from the small intestine into the large intestine. Diseases
of the colon lead to disorders in the digestion of food and its transport,
leading to constipation.
There is also the so-called san
jiao organ whose basic physiological function is to control the qi activity of
the whole organism. It is divided into three parts: the upper jiao is located
just above the diaphragm and the heart and lungs are located there, the middle
jiao is located between the diaphragm and the navel, and the spleen and abdomen
are located there. The lower jiao is located just below the navel and is where
the liver, kidneys, bladder, and intestines are located.
System of meridians and parallels
The meridians (ying) and parallels (luo) represent the pathways through which
qi and blood circulate. The meridians are the largest channels in the system
and they extend vertically through the interior of the body, while the
parallels are the branches of the meridians. Since they can be found throughout
the whole body, they serve to interconnect zang-fu and other organs, openings
of the body, skin, muscles and bones. They form a special network that
communicates with all the internal organs of the body and limbs, and connect
the upper part of the body with the lower. The meridian system consists of 12
basic meridians: three Yin meridians of the hand, three Yin meridians of the
foot, three Yang meridians of the hand, and three Yang meridians of the foot;
and of 8 additional meridians: Du, Ren, Chong, Dai, Yingqiao, Yangqiao, Yinwei
and Yangwei. The eight additional meridians are not directly connected to the
internal organs, but intersect with the 12 basic meridians and help them
achieve normal communication.
The first meridian is the
pulmonary channel of the hand (Taiyin) and it starts from the middle of the
abdomen, reaches the large intestine and then returns to the diaphragm, passes
through the lungs and then through the lungs and larynx to the surface of the
right hand where it ends on the index finger (Figure 8).
The second meridian is the colon
meridian of the colon Yangming which starts from the index finger of the right
hand and extends along the lateral side of the forearm and the lateral side of
the elbow. From the elbow, the front border of the upper arm reaches the highest
point of the shoulder and at that point it branches into two branches.
One enters the body and passes
through the lungs, diaphragm and colon, and the other passes through the outer
part of the neck, cheeks and reaches the inner surfaces of the teeth in the
lower jaw, ending in a circular motion around the lips and at a point
corresponding to the height of the nose at the nape of the neck (Figure 9).
The abdominal meridian of the
foot Yangming extends from the nose, through the diaphragm, spleen, colon,
through the lateral side of the right foot to the tip of the middle toe (Figure
10).
The meridian of the spleen starts
from the thick toe, extending along the inside of the foot to the outside of
the ankle. From that point, the meridian extends along the inner side of the
lower leg to the medial aspect of the knee and hip, and then enters the abdomen
and spleen. From the spleen, the meridian extends to the chest, larynx, and
root of the tongue. Another branch extends from the spleen to the heart and
connects to the cardiac meridian (Figure 11).
The heart meridian of the hand
Shaoyin is a meridian that has three branches and each starts from the heart.
One branch flow down to the
diaphragm and small intestine.
The second branch of the meridian
goes up to the larynx and ends in the eye. The third branch of the meridian
passes through the chest and connects the heart to the lungs, and then goes to
the armpits. From the armpit it goes down the medial side of the hand and ends
at the tip of the little finger and connects with the meridian of the small
intestine (Figure 12).
The small intestine meridian of
the Taiyang hand begins where the previous meridian ends, from the tip of the
little finger and extends to the posterior part of the shoulder and there
encompasses the shoulder and continues further to the middle of the upper back
and merges with the Du meridian. At this point, the meridian branches into two
parts in which one part connects with the heart, diaphragm, abdomen, and small
intestine, and the other part with the neck, cheeks, outer part of the eye, and
enters the ear (Figure 13).
The bladder meridian Taiyang,
starts from the inside of the eye and reaches the forehead to the side of the
head.
One smaller branch then passes to
the brain, and the main branch extends to the nape of the head and reaches the
neck and spine. One part then branches and connects to the kidney, and the
other part continues to the bladder.
The main part of the meridian
continues through the buttocks, the knee and ends on the lateral side of the
little toe and thus connects with the renal meridian (Figure 14).
The renal meridian from the foot
Shaoyin begins on the inferior side of the little toe, passes through the
ankle, the medial side of the lower leg, the hip, and enters the body where the
lower part of the spine begins. Here the meridian branches and connects with
the kidney and gall bladder, and then returns to the surface of the body and
binds to the upper abdomen and chest. The branch associated with the kidney
passes to the liver, diaphragm, and enters the lungs from where it passes
through the larynx and ends at the root of the tongue (Figure 15).
The most famous herbal remedies
of the Traditional Chinese Medicine Rheum rhabarbarum Rhubarb (Figure 16) has
been used in Chinese pharmacy for thousands of years, and was first described
by the mythical legend Shen Nung, although there are some opinions that the
plant was used as far back as 2700 years before. According to Dioscorides, the
roots of this plant were brought to Greece from the shores of the Bosphorus, it
was not used much commercially during the Islamic era, it arrived in Europe
during the 14th century where it was imported from Silk Street via the ports of
Aleppo and Smyrna. It was then known as Turkish rhubarb. For centuries, the
plant grew along the banks of the Volga river, whence its ancient name Rha. The
expensive cost of transporting the plant from Asia made rhubarb a very prized
and expensive plant�it was several times more expensive than cinnamon or opium.
At one time, Marco Polo researched where this plant grows and picked it in the
province of Tangut. Even in his report, Ambassador Ruy Gonzales de Clavijo
wrote in 1403 that the best goods arriving in Samarkand from China certainly
included rhubarb. The name rhubarb itself comes from the Greek words rha and
barbarum.
 ��
��
Figure 15. The renal meridian from the foot Shaoyin
Available at: http://cdn.intechopen.com/pdfs-wm/21300.pdf.
Accessed: March 20, 2017.
�
Figure 17. Panax ginseng.
Available at:
http://thisisnotacure.files.wordpress.com/2012/02/panax-ginseng.gif?w=714.
Accessed: March 22, 2017.
The word rha means both plant and
river Volga. Rhubarb arrived in the USA in 1820, and was brought by Western
European immigrants. Rhubarb is a perennial herbaceous plant that grows up to 3
meters high. The rhizome and root are very developed. It grows in the northern
parts of China and in Tibet. The drug is represented by parts of peeled and
dried rhizomes of several years old wild and cultivated rhubarb plants. The
taste of the rhizome is bitter and it crunches under the teeth, it has a weak
and specific smell.
Rhubarb rhizome contains
anthraquinone heterosides.
Heterodiantron structures and
their heterosides are also present in the rhizome. It has tannins, starch,
pectin, resinous substances and calcium oxalate. In terms of action,
anthraquinone heterosides have a laxative effect and tannins have an astringent
effect. Rhubarb rhizome pollinated was used as a laxative in acute constipation,
and in smaller doses it was used in digestive disorders.
Panax ginseng Ginseng root
(Figure 17), due to its stimulating effect on the body, has long been used in
concentrated form as a medicinal agent or in diluted form as a tea preparation.
The Chinese have noticed that
regular consumption of ginseng improves the general condition of the body,
appetite and mental activity, and has a preventive effect against many
diseases. During the Vietnam War, ginseng was used by many Vietcong fighters,
using it to treat the wounded who died in explosions. In the late fifties of
the last century, Soviet scientists proved its extremely beneficial effect on
raising the fitness of athletes, and it was used in the former Soviet Union to
achieve top results.
The Russian Olympic team uses
Siberian ginsengbased preparations on a daily basis. Japanese researchers have
found that taking Siberian ginseng significantly improves the results of
cyclists�by as much as 23 percent compared to athletes who do not take ginseng.
Ginseng is also called the root of life.
Ginseng is one of the oldest,
most widely used and most studied plants in the world. Although there are
several plants called Ginseng and they all belong to the genus Panaxa, American
Ginseng (Panax Quinquefolius) is believed to cool the body, so it is used in
various fevers, while Asian Ginseng (Panax Ginseng) has the opposite effect and
is used to improve circulation. Different types of Ginseng often symbolize the
energy of yin (American) and yang (Asian), because their action is opposed to
each other just like these ancient concepts. American Ginseng, in addition to
cooling the body, increases energy and endurance, which is necessary for people
who are stressed and live a modern fast-paced lifestyle. On the other hand, by
relaxing the yang, this force opposed to cold yin, through the Asian plant
helps the body recover and stimulates the whole body. Asian Ginseng (Panax
Ginseng) is a perennial shrub, about 70 centimeters tall. From its stems grow
leaves in the vertebrae. The fruits are bright red berries, with two seeds
each, flattened in width. The dried root of the plant is most commonly used,
although sometimes dried leaves that are less prized than the root can also be
found. Ginseng was first discovered in China about 5000 years ago, in the
Manchuria region. It quickly became appreciated for restoring strength and
renewing energy, and its �human� form became a powerful symbol of divine
harmony on earth.
In the first Chinese book on
medicinal herbs �Classical Medicinal Plants� (Pen Tsao Ching) Ginseng is
recommended for enlightening the mind and increasing wisdom. Ginseng grows in
secluded places in the shady forests and hills of Korea, China and Russia. In
ancient times, only wild Ginseng was used because it was long believed that
Ginseng could not be grown because of its sensitivity and the special
conditions in which it must grow, from the proper temperature to shady soil
rich in minerals. Ginseng is known as an adaptogen, or agent that increases
resistance to stress. It also strengthens the immune system, provides energy
and vitality, rejuvenates the body by improving its functions. In addition to
its excellent effect on the immune system, ginseng has a very beneficial effect
on the nervous and cardiovascular system. It increases concentration,
intellectual ability and memory, helps with headaches, insomnia and has an
antidepressant effect. In addition, it detoxifies the blood, prevents anemia,
lowers blood sugar and cholesterol levels, regulates blood pressure, improves circulation.
It is an excellent antioxidant, and some research shows that it also helps in
the treatment of cancer.
The best results are achieved in
combination with other traditional Chinese plants. Wild American Ginseng was
once widespread in all mountainous regions of the United States and Canada, and
today it is an endangered species.
That is why it is now grown on
farms to protect Wild Ginseng from over-harvesting. The Native Americans have
traditionally used it as a stimulant and to treat headaches, fevers,
indigestion and infertility. Like Asian, American Ginseng is an adaptogen, a
plant that helps the body cope with various types of stress and is considered
one of the most popular plants in the USA. Both American and Asian Ginseng
contain ginsenosides, although the type and ratio of these substances differ in
Asian and American herbs. American ginseng has a more relaxing effect than
Asian Ginseng, which has a stimulating effect.
Animal laboratory studies have
shown that American Ginseng is effective in boosting the immune system, as an
antioxidant and has good potential in treating inflammatory diseases, diabetes,
colds and flu and helping to treat cancer. Siberian Ginseng is also considered
an adaptogen because plant extracts help the body adapt to stress. The
regulatory action of Siberian Ginseng extract has been shown to be useful in
meteorologists. Experiences from traditional medicine, as well as numerous
studies conducted especially on Russian athletes, suggest a beneficial effect
of Siberian Ginseng extract on the regulation of low blood pressure. Siberian
Ginseng root preparations have found useful application in improving physical
and mental condition (working ability), increasing the body�s general
resistance and strengthening the heart, blood circulation and nerves. It is
also used as an immunostimulant.
This herb can be taken long term.
Podophyllum peltatum
�
Figure 18. Podophyllum peltatum � plant which is used in
Traditional Chinese medicine as laxative Available at: http://www.henriettes-herb.com/files/images/old/barton-w/w-barton-t25-podophyllum-peltatum.jpg.
Accessed: March 24, 2017.
It is a small woody perennial
plant up to 30 centimeters tall. At the top of the shoots are two large,
finger-divided leaves. Podophyllum peltatum (Figure 18) grows in the forests of
the eastern part of the North American continent and in India in the Himalayas.
The drug is a resin obtained from the ethanolic extract of the rhizome of this
plant. The resin is a crumbly, amorphous mass, gray in color, with an extremely
bitter taste and a specific odor.
The main pharmacologically active
ingredients of the resin are podophyllotoxin and peltatins. Both inhibit the
growth of experimentally induced tumors. These lignans prevent tubulin
polymerization and the formation of dividing spindle microtubules, thus
stopping cell division in metaphase. Rhizome and resin podophyllin have
traditionally been used as a laxative and remedy against intestinal parasites.
Today, this application has been abandoned due to its extreme toxicity. In the
form of galenic preparations, they are rarely used for external use on the
skin. Podophyllotoxin is a natural lignan that is the basis for obtaining
synthetic derivatives of teniposide and etoposide. Etoposide is commonly used
in combination chemotherapy for testicular and bronchial cancer, lymphoma, and
acute leukemia. Teniposide is used in the treatment of lymphoma, acute
leukemia, brain tumors and urogenital tumors.
Cinnamomum ceylanicum
Cinnamon (Figure 19) is first
mentioned in the Chinese books from 2800 BC, where it is used for medical
purposes for colds and digestive problems. It is also mentioned in the Bible,
Moses used it in anointing oils, and the ancient Romans burnt it during burial,
probably to neutralize unpleasant odors, among other things. Due to its
pleasant smell, but also as a preservative, Egyptians used it in the process of
mummification. Although today it is one of all known and present spices,
cinnamon wasn�t always available. The search for cinnamon was one of the
initiators of many quests in the 15th century. Given that it was delivered from
afar, because it originally originated in Ceylon, and that the Venetians, in
fact, had a monopoly on maritime routes, only the elite could afford the
fragrant
|
|
Figure 19. Cinnamonum
celyanicum- Ceylon cinnamon.
Available at:
http://www.sacredearth.com/Ezine/winter09/ChineseCinn.gif.
Accessed: March 24,
2017.
|
and expensive spice. Due to the
growing demand and use for medical and culinary purposes and high prices, traders
have realized that by controlling the only place in the world where this spice
grows, they have a monopoly on its placement, and thus control the world price.
The first to secure a monopoly were Portuguese merchants� they reached Ceylon
(bypassing the horn of Africa) in the 15th century. They tried to increase
production, enslaved the local population and eliminated competition. Soon the
Dutch intervened and in 1640, they suppressed the Portuguese and took control
of the monopoly. Nor did the Dutch rule last forever, it was replaced by the
English and by 1796 they had completely conquered the monopoly over the
production and trade of cinnamon. However, it was also the end of the local
cultivation of cinnamon, the plant spread to other parts, so that today
cinnamon is neither a luxury nor an expensive spice. The spice, which was an
exclusive product of Sri Lanka, is today grown in India, Sumatra, Java, Brazil,
Vietnam, Egypt and Madagascar. In traditional Chinese medicine, cinnamon is
used for colds, digestive problems, nausea. Chinese writings mention the
beneficial use of cinnamon for people whose feet are always cold. The Egyptians
used it in the process of embalming, but also for storing meat. The ancient
Romans put cinnamon in many medicinal powders. It was used for colds but also
as a room freshener�it was lit both in homes and in temples. Great use brought
great demand and high price, so that Pliny the Elder in the first century noted
that cinnamon is 15 times more valuable than silver.
Ayurvedic medicine treats
diabetes with cinnamon, indigestion.
It is an integral part of tea cinnamon wasn�t used for
better digestion, and the oil is used in aromatherapy for calming.
Numerous studies indicate a
positive role of cinnamon in diet. For example, Swedish researchers from Malm�
University Hospital examined the effects of cinnamon on human health and gave
subjects rice pudding with or without cinnamon. In subjects whose pudding was
sprinkled with cinnamon, the blood sugar level was significantly lower. Researchers
believe that cinnamon slows down digestion, giving the body more time to break
down carbohydrates. However, skeptics note that an insufficient sample�only
fourteen respondents�calls this research into question. Another study from 2003
indicates the positive role of cinnamon in people with diabetes. In people with
diabetes 2, if they take 1-6 grams of cinnamon a day, the glucose level is
reduced after six months, in some by as much as 29%. Also, the level of
triglycerides was reduced by 23-30%. Cinnamon also has an antifungal,
antibacterial effect, and has been shown to be successful in persistent
Helicobacter pylori infections. Cinnamon is always a green, short tree. The
drug consists of peeled and dried bark of young branches of the cinnamon tree. A
dozen thin covers are folded and dried quickly in the sun or in dryers.
Otherwise, it comes in the form of gutter pieces that contain up to a dozen
thin covers. The cortex of the cinnamon tree contains essential oil in the
amount of 0.5 to 2.5%, and the essential oil contains cimetaldehyde, cinnamic
acid, eugenol, limonene and alphaterpineol.
The cortex also contains coumarin
mucus and tannins. Cinnamon essential oil has a characteristic aroma and
exhibits antibacterial activity. In combination with other drugs, it also has
an antispasmodic effect. Powdered cortex is used for digestive disorders and
painful spasm of smooth muscles. The oil is used as a flavoring agent for some
pharmaceutical preparations, as well as for the production of aromatic water and
in the perfume industry. The largest amounts of cortex and essential oil are
used as a spice.
Ephedra sinica Ephedra (Figure
20) is a plant of Chinese origin and is known in China as ma huang, it has been
used traditionally for over 5000 years. Indeed, there are several species of
the genus Ephedra that are used for various medicinal purposes, and have often
been used in the preparation of the Soma solution used in the Indo-Iranian
religion. It was also used by the Indians in the preparation of Indian tea.
The ephedra is a low branched
shrub. The drug makes up the dried, above-ground, herbaceous part of the plant
in bloom. Herb ephedra contains flavonoids and proanthocyanidins but the most
important ingredients are protoalkaloids.
The most important are ephedrine
and pseudoephedrine.
Ephedrine is an indirect
sympathomimetic. It works similar to adrenaline, but weaker. The
anti-inflammatory action of pseudoephedrine has been experimentally confirmed.
It is used in the treatment of asthma, bronchitis and febrile conditions. In
the form of drops, it is used in the treatment of diseases of the nose and
eyes: it narrows blood vessels and acts as a mild local anesthetic.
Wolfiporia cocos Fuling (Figure
21) has been used in Traditional Chinese
�
Figure 20. Ephedra sinica � herb which is used in
Traditional Chinese Medicine for treating asthma and bronchitis.
Available at: http://www.itmonline.org/image/ma1.JPG
Accessed: March 25, 2017.
Medicine for thousands of years.
Due to its multiple medicinal effects, this mushroom is considered, according
to Chinese tradition, one of the eight treasures. Fuling mushroom is used in
Chinese medicine to make a large number of medicines, but also delicacies and
snacks for the richest families, including the royal vine.
This mushroom is characterized by
several names, such as Poria cocos, Indian barrel, Chinese root, Fu Ling Pi, Fu
Shen, hoelen, etc. Today, this mushroom can be found in the wild, but is also
cultivated in places such as Yunnan, Anhui, Hubei, Henan, Sichuan, etc., and
the best quality comes from Yunnan.
The healing effects of fuling
stem from its rich chemical composition. Triterpenoids, polysaccharides,
ergosterol, caprylic acid, undecanoic acid, lauric acid, dodecanoic acid,
palmitic acid, caprylates and other elements can
|

|
Figure 21. Fuling
mushroom � often used mushroom in TCM. Available at:
http://www.chineseherbshealing.com/poria-fu-ling/.
Accessed: March 27, 2017.
|
be found in the flesh of this
fungus. Of the triterpenoids, the most important are pachymic acid, tumuloic
acid, Cmethyl ester of polypenic acid, methyl ester of tumulose acid, etc., and
the most important polysaccharides are pachyman, pachymaran and gluan H11.
In Traditional Chinese Medicine,
but also in modern pharmacological tests, it has been established that this
fungus has the following effects:
� Diuretic effect: fuling mushroom itself has no diuretic
effect, but in a combination called Wu Ling
San, it shows a pronounced diuretic effect;
� Antibacterial effect: in vitro experiments have shown that
the ethanol extract of this fungus can have a bactericidal effect on
leptospires;
� Digestive system: fuling can relax the intestines, reduce
the strength of stomach acid and prevent ulcers in the stomach or small intestine;
� Regulation of blood sugar;
� Enhances heart contractility.
Cordyceps sinensis � Chinese caterpillar mushroom
Cordyceps (Figure 22) is a
mushroom native to Tibet, be found in the flesh of this fungus. Of the
triterpenoids, the most important are pachymic acid, tumuloic acid, Cmethyl
ester of polypenic acid, methyl ester of tumulose acid, etc., and the most
important polysaccharides are pachyman, pachymaran and gluan H11.
In Traditional Chinese Medicine, but also in modern
pharmacological tests, it has been established that this fungus has the
following effects:
� Diuretic effect: fuling mushroom itself has no diuretic
effect, but in a combination called Wu Ling
San, it shows a pronounced diuretic effect;
� Antibacterial effect: in vitro experiments have shown that
the ethanol extract of this fungus can have a bactericidal effect on
leptospires;
� Digestive system: fuling can relax the intestines, reduce
the strength of stomach acid and prevent ulcers in the stomach or small
intestine;
� Regulation of blood sugar;
� Enhances heart contractility.
Cordyceps sinensis � Chinese caterpillar mushroom
Cordyceps (Figure 22) is a mushroom native to Tibet,
|
|
Figure 22. Cordyceps � a
mushroom which attacks caterpillars and it grows out of their corpse.
Available at:
http://www.pecurke-sitake.com/kordiceps-gljiva.php
Accessed: March 27,
2017.
|
China, and grows at an altitude of 5,000 meters. Its price
is extremely high, and it costs up to 3000 USD per kilogram.
Precisely because of the great
demand, and also because of the difficulties in finding the mushroom itself, it
was given for medicinal purposes only to noble families and the King of China
himself. Its natural nutritional basis is not like other fungi, but it is a
type of caterpillar. The mushroom attacks these caterpillars, kills them and
then sprouts out of them with its finger-like body. Scientists have been trying
to grow this mushroom for a long time, since its natural reproduction does not
meet world demand, but everything has remained to be tried.
In traditional Chinese medicine,
this mushroom is used to strengthen the lungs and kidneys, as well as to tone
yin yang. It is believed to calm emotions, remove mucus and prevent bleeding.
It has a positive effect on cancer control, treatment of rheumatism, fatigue,
respiratory diseases, inflammation, insomnia and irregular men-struation.
Cordyceps improves the supply of tissues and organs with blood and oxygen. It
has been scientifically proven that this mushroom has antimicrobial action and
that it stops the growth of the bacterium Clostridium without breaking down
bifidobacteria and lactobacilli in the intestines. Studies have also shown a
significant increase in the activity of natural cells that kill cancer cells
(macrophages).
Acupuncture as a method of
treatment in Traditional Chinese Medicine Acupuncture is a method of treatment
using needles that are inserted into specific points on the body, and which the
Chinese have mapped during the long history of TCM. The goal is to stimulate
energy centers and improve the flow of qi through the body. It is a word of
Latin origin (acus�needle, pungere�to prick), and it was the name given to it
by European missionaries who visited China at the end of the 16th century and
were the first to bring the word of healing in this way. The origin of
acupuncture is related to the story of a warrior wounded by an arrow. The arrow
was taken out and the wound healed, and it was later noticed that the disease
had healed on another part of his body. The first needles used by the Chinese
were stone, then bone and bamboo, while today disposable surgical steel needles
are used. In addition to classical acupuncture, electroacupuncture is
increasingly used to perform surface electrostimulation through the skin.
Acupuncture points are stimulated with a special probe (sticks) without
stabbing.
In 1979, the World Health
Organization recognized acupuncture as an equal branch of medicine because it
meets standards that are in line with modern methods of treatment. It is
accepted that it can be used as the only therapy, in combination with another
method of treatment or as an adjuvant therapy. Its indication area is very
wide, and the effect is observed in 70-80% of cases. On that occasion, a list
of diseases that are successfully treated with this method was compiled. Some
of them are: sinusitis, constipation, headaches, migraines, neuralgia, pain of
the skeletal and muscular system, bronchitis, asthma, ulcers, infertility,
menstrual problems, insomnia, various skin diseases, diabetes, hemorrhoids,
etc.
Acupuncture has been shown to be
very effective in relieving postoperative pain, nausea and vomiting due to
chemotherapy and radiation. Acupuncture follows the development of technology
and successfully follows modern achievements, so there was the emergence of
electroacupuncture, fluid acupuncture, laser acupuncture and the like. The
method of laser acupuncture is non-invasive, painless and shortterm therapy.
The exact mechanism of action of lowpower laser energy has not been fully elucidated.
At the cellular level, the basic processes that lead to the healing of cells,
tissues, organs and the organism as a whole are accelerated or slowed down.
Biological changes are a consequence not only of the immediate effect of the
laser, but also of the host response consisting in a change in metabolic
activities lasting up to a month. The advantages of laser acupuncture are:
asepsis, painlessness, economy and possible application on any part of the
body, skin or mucous membranes.
Acupuncture and moxibustion are
specific methods by which internal diseases are treated by �external� methods.
Thus a variety of diseases can be cured using methods that require absolute
knowledge of the internal channels and the flow of qi through them. In order
for someone to perform acupuncture, it is necessary to know the theory of �eight
principles�, zang-fu theory and the flow and arrangement of meridians and
parallels through the human body. After discovering the channel or internal
organ that is damaged, it is necessary to find out the mechanism of the disease
and determine the essence and secondary symptoms, and only then decide on
acupuncture or moxibustion, and whether there should be a method of
strengthening or reducing. The basic principle of acupuncture treatment is: the
method of strengthening should be applied in xu (deficiency) syndrome, and the
method of reduction for shi (excess) syndrome. Moxibustion is applied when
vital function or yang is declining.
Acupuncture is based on the selection of three puncture
points:
� Selection of distant points (e.g. if treating a facial
disease, points located on the lower part of the body are selected);
� Selection of local points (in case of a wound, points
close to the wound are selected) and;
� Selection of adjacent points (if local points cannot be
selected, the so-called adjacent points are selected to strengthen the
therapeutic effect).
5. DISCUSSION
History is overfull with
mythology in the case of the Three Kings of Heaven who are revered as the
founders of Chinese civilization. Fu Hsi, who is thought to have ruled 2000
years before Christ, is the legendary founder of the first Chinese dynasty. His
most important inventions included writing, painting, music, original mythical
trigrams, and the yin-yang concept. During a century of rule, Huang Ti, the
last of the three legendary Heavenly Emperors, gave his people a wheel, a
magnet, an observatory, a calendar, the art of measuring heart rate, and the
Huang-ti Nei Ching (Yellow Emperor�s Canon of Internal Medicine) �a text that
inspired and guided Chinese medical thought over 2500 years. Like many ancient
texts, the Nei Ching has been corrupted over the centuries with additions,
cutouts, and typographical errors.
Scholars agree that the existing
text is very old, perhaps even dating back to the first century BC, but the
time of its compilation is polemical. Most historians believe that the existing
text was composed at the beginning of the T�ang dynasty (618-907).
The first records of traditional
Chinese medicine (TCM) date back to 5000 years ago. TCM encompasses Han
medicine and the theories and practices of various national minorities from
China such as Miao, Dai, Mongols and Tibetans. The first records of TCM appear
from the period 2698-2598 years before the new era, during the era of Huangdi
or the Yellow Ruler. However, the duties and responsibilities of physicians
were defined only later, in 1122 BC, during the Zhou dynasty. At the time,
every large estate had its own physician, and it was characteristic that physicians
were paid when the householders were healthy, not when they fell ill. Thus, the
primary concern of physicians was to maintain health and prevent disease, not
to treat it. TCM is the oldest continuously practiced, scientific medical
system in the world. It should certainly not be classified as an expression of
folk medicine, nor quackery, because TCM is a complex and precise health care
system created from the efforts of great Chinese minds to understand the
secrets of the functioning of the human body. In its beginnings, TCM was a
practical and effective art based on observations and experience with the
application of philosophical principles such as Yin and Yang or wu-xing (the
theory of the five elements).
The basic thinking was that
health can be maintained if there is a balance of the human body with the inner
spirit and the outer environment. For this reason, diagnosis and treatment were
based on targeted finding of imbalance and its return to normal. The greatest
success and development of TKM was experienced during the Ming Dynasty
(1368-1644), culminating in the publication of the Compendium of Material
Medica (Figure 5) by Li Shizhen. Li Shizhen has dedicated himself to gathering
the most important and credible medical experiences over 30 years and has
singled out a total of 1,094 herbal medicines, 443 animal medicines and 354
mineral medicines.
For each drug, an adequate name,
source, form and medical history were prescribed, as well as the manner in
which it was collected, prepared, stored and dosed.
Modern TCM theory has emerged
from the naturalistic philosophies of ancient China with special influences of
experiences that have accumulated through generations and generations. TCM may
seem outdated and charlatan today, but it is a complete, integrated method of
interpreting human physiology and pathological changes in the body. The most
important concepts of TCM are qi, yin yang and the theory of the five elements
(wuxing). Theoretical concepts of specific TCM include the doctrine of zheng ti
guang nian, the concepts of viscera and compassion (zangfu xue shuo), channels
and networks (jingluo), bodily substances (qi, blood, essence and body fluids
qi xue jing jinye) and pathological agents (bing yin). All these theories,
together with the methodologies of the four methods (si zhen) and basic
discrimination (bian zheng) form the theoretical basis of TCM. Each of the
therapeutic methods of TCM, such as acupuncture and moxibustion (zhenjiu),
Chinese herbology (zhongyao fang), and Chinese therapeutic massage (zhongyi
tuina) are based on the stated theoretical foundations.
The basic concept of qi theory is
that qi is the basic substance from which the entire universe is built and that
all objects in the universe are born by the transformation of qi. Ancient
philosophers argued that qi could exist in two states: dispersion and
condensation, and these two states of qi determine two modes of perception in
man: one having a form and one without a form.
According to ancient Chinese
philosophy, yin and yang represent two essentially opposite categories. At
first, their understanding was simple, describing the turning of the face or
back to sunlight. It was later introduced into the theory that yin and yang
refer to almost all imaginable opposites, such as time, position, side of the
world, state, etc. Ancient Chinese philosophers wisely observed that for every
phenomenon there are two opposing aspects with each other. Thus, yang
represents phenomena such as speech, active state, external, upper, warm,
light, while yin is associated with opposite phenomena: silence, inactive
state, internal, lower, cold, dark.
The theory of the five
elements/phases establishes such a system of correspondence that all phenomena
in the universe can be classified into five categories. The categories
represent a tendency to move and transform in the universe and are related to
natural phenomena such as wood (mu), fire (huo), earth (tu), metal (yin) and
water (shui). A constant connection between them is used to explain changes in
nature. In traditional Chinese medicine, most human organs are divided into two
groups: five zang and six fu organs. The five zang organs are the heart, liver,
spleen, lungs and kidneys, which are the most important organs in the human
body. The six fu organs are bile, stomach, small and large intestine, bladder,
and san jiao, all of which are important for the role of transporting and
processing food and water.
The meridians (ying) and
parallels (luo) represent the pathways through which qi and blood circulate.
The meridians are the largest channels in the system and they extend vertically
through the interior of the body, while the parallels are the branches of the
meridians. Since they can be found throughout the whole body, they serve to
interconnect zang-fu and other organs, openings of the body, skin, muscles and
bones. They form a special network that communicates with all the internal
organs of the body and limbs, and connects the upper part of the body with the
lower. The meridian system consists of 12 basic meridians: three Yin meridians
of the hand, three Yin meridians of the foot, three Yang meridians of the hand,
and three Yang meridians of the foot; and of 8 additional meridians: Du, Ren,
Chong, Dai, Yingqiao, Yangqiao, Yinwei and Yangwei. The eight additional
meridians are not directly connected to the internal organs but intersect with
the 12 basic meridians and help them to achieve normal communication.
Acupuncture is a method of
treatment using needles that are inserted into specific points on the body, and
which the Chinese have mapped during the long history of TCM. The goal is to
stimulate energy centers and improve the flow of qi through the body. It is a
word of Latin origin (acus�needle, pungere�to prick), and it was called by
European missionaries who visited China at the end of the 16th century and were
the first to bring word about healing in this way. The origin of acupuncture is
related to the story of a warrior wounded by an arrow. The arrow was taken out
and the wound healed, and it was later no ticed that the disease had healed on
another part of his body. The first needles used by the Chinese were stone,
then bone and bamboo cane, and today disposable surgical steel needles are
used.
6. CONCLUSION
Traditional Chinese medicine has
managed to resist time and has existed for 5000 years, since when there is the
first record of its practice. Although the word is traditional in the name, it
follows the development of modern medicine, so the World Health Organization
(WHO) has accepted it as a scientifically proven medicine. Experiences of
treatment with drugs from Greak, Persian and Arabic medicine, Traditional
medicine has been accepted as official Complementary medicine in daily praxis,
recommended by WHO (18-24). The basis of traditional Chinese medicine consists
of several theories, such as zang-fu organs, yin and yang, qi, the theory of
the five elements and the concept of meridians and parallels. All theories are
interconnected and form one complicated whole. Yin and yang and qi are perhaps
the most important aspect of traditional Chinese medicine because everything is
based on balancing the energy of qi and the balance between yin and yang.
Certainly, the most complicated aspect of traditional Chinese medicine is
acupuncture, which requires detailed knowledge of all five theories and
knowledge of key points on the human body and their interrelationship, all for
the purpose of treating certain diseases and balancing qi and balancing yin and
yang.
� Authors contribution: All authors were included in
preparation of this article. Final proof reading was made by the Tarik Catic
and Izet Masic.
� Conflict of interest: None declared.
� Financial support and sponsorship: Nil
(back
to content)
1.2.3.2 History of Acupuncture w
Acupuncture can be traced back to
the primitive society of China, which is divided into two time periods
The old stone age (10,000 years
ago and beyond) and the new stone age (10,000-4000 years ago).
During the old stone age knives
were made of stone and were used for certain medical procedures.
During the new stone age, stones
were refined into fine needles and served as instruments of healing. They were
named bian stone � which means use of a sharp edged stone to treat disease.
The most significant milestone in
the history of Acupuncture occurred during the period of Huang Di �The Yellow
Emperor (2697-2597).
In a famous dialogue between
Huang Di and his physician Qi Bo, they discuss the whole spectrum of the
Chinese Medical Arts. These conversations would later become the monumental
text � The Nei Jing (The Yellow Emperors Classic of Internal Medicine).
The most significant milestone in
the history of Acupuncture occurred during the period of Huang Di �The Yellow
Emperor (2697-2597).
In a famous dialogue between
Huang Di and his physician Qi Bo, they discuss the whole spectrum of the
Chinese Medical Arts. These conversations would later become the monumental
text � The Nei Jing (The Yellow Emperors Classic of Internal Medicine).
The most significant milestone in
the history of Acupuncture occurred during the period of Huang Di �The Yellow
Emperor (2697-2597).
In a famous dialogue between
Huang Di and his physician Qi Bo, they discuss the whole spectrum of the
Chinese Medical Arts. These conversations would later become the monumental
text � The Nei Jing (The Yellow Emperors Classic of Internal Medicine).
During the Shang Dynasty (1000
BC) , hieroglyphs showed evidence of Acupuncture and Moxibustion. Bronze
needles were excavated from ruins, but the bian stones remained the main form
of needle.
During the Warren States Era
(421-221 B.C.) metal needles replaced the bian stones. The Miraculous Pivot
names nine types of Acupuncture needles. The historical records notes many
physicians practicing Acupuncture during this time. Another milestone for this
period was the compilation of the Nan Jing (Book of Difficult Questions). The
Nan Jing discusses five element theory, hara diagnosis, eight extra meridians,
and other important topics.
From 260-265 A.D., the famous
physician Huang Fu Mi, organized all of the ancient literature into his classic
text � Systematic Classics of Acupuncture and Moxibustion.
The text is twelve volumes and
describes 349 Acupuncture points. It is organized according to the theory of:
zang fu, Qi and blood, channels and collaterals, acupuncture points, and
clinical application. This book is noted to be one of the most influential
texts in the history of Chinese Medicine.
Acupuncture experienced great
development during the Sui (581-618) and Tang (618-907) Dynasties. Upon request
from the Tang Government (627-649A.D.), the famous physician Zhen Quan revised
the important Acupuncture texts and charts.
From 260-265 A.D., the famous
physician Huang Fu Mi, organized all of the ancient literature into his classic
text � Systematic Classics of Acupuncture and Moxibustion.
The text is twelve volumes and
describes 349 Acupuncture points. It is organized according to the theory of:
zang fu, Qi and blood, channels and collaterals, acupuncture points, and
clinical application. This book is noted to be one of the most influential
texts in the history of Chinese Medicine.
Acupuncture experienced great
development during the Sui (581-618) and Tang (618-907) Dynasties. Upon request
from the Tang Government (627-649A.D.), the famous physician Zhen Quan revised
the important Acupuncture texts and charts.
1601 � Yang Jizhou wrote Zhenjin
Dacheng (Principles of Acupuncture and Moxibustion). This great treatise on
Acupuncture reinforced the principles of the Nei Jing and Nan Jing. This work
was the foundation of the teachings of G. Soulie de Morant who introduced Acupuncture
into Europe.
From the Qing Dynasty to the
Opium Wars (1644-1840), herbal medicine became the main tool of physicians and
Acupuncture was suppressed.
Following the revolution of 1911,
Western Medicine was introduced and Acupuncture and Chinese Herbology were
suppressed
�Due to the large population and need for
medical care, Acupuncture and herbs remained popular among the folk people, and
the �barefoot doctor� emerged.
In 1950 Chairman Mao Zedong
officially united Traditional Chinese Medicine with Western Medicine, and
acupuncture became established in many hospitals
In the same year Comrade Zhu De
reinforced Traditional Chinese Medicine with his book New Acupuncture
�Acupuncture gained attention in the United States when
President Richard Nixon visited China in 1972.
� During one part of the visit, the delegation was shown a
patient undergoing major surgery while fully awake, ostensibly receiving
acupuncture rather than anesthesia.
The Ming Dynasty (1568-1644) was the enlightening period for
the advancement of Acu-puncture. Many new developments included:
- Revision of the classic texts
- Refinement of Acupuncture techniques and manipulation
- Development of Moxa sticks for indirect treatment
- Development of extra points outside the main meridians
- The encyclopaedic work of 120 volumes- Principle and
Practice of Medicine was written by the famous physician Wang Gendung
The greatest exposure in the West
came when New York Times reporter James Reston, who accompanied Nixon during
the visit, received acupuncture in China for post-operative pain after
undergoing an emergency appendectomy under standard anaesthesia.
Reston believed he had pain
relief from the acupuncture and wrote it in The New York Times.
In 1973 the American Internal
Revenue Service allowed acupuncture to be deducted as a medical expense. This
sparked an intense interest in acupuncture by the public.
Several months later, a report
favourable to acupuncture was published in the Journal of the American Medical
Association.
(back
to content)
1.2.3.3 Feng shui w
Feng shui (/ˈfʌŋˌʃuːi/),
also known as Chinese geomancy, is an ancient Chinese traditional practice
which claims to use energy forces to harmonize individuals with their
surrounding environment. The term feng shui means, literally,
"wind-water". From ancient times, landscapes and bodies of water were
thought to direct the flow of the universal Qi � �cosmic current� or energy �
through places and structures. Because Qi has the same patterns as wind and
water, a specialist who understands them can affect these flows to improve
wealth, happiness, long life, and family; on the other hand, the wrong flow of
Qi brings bad results. More broadly, feng shui includes astronomical,
astrological, architectural, cosmological, geographical, and topographical
dimensions.
Feng shui analysis of a 癸山丁向
site, with an auspicious circle
Feng shui
Chinese name
Traditional Chinese 風水
Simplified Chinese 风水
Literal meaning "wind-water"
Transcriptions
Standard Mandarin
Hanyu Pinyin ���� ��������������� fēngshuǐ
Bopomofo ������������������������� ㄈㄥ
ㄕㄨㄟˇ
Wade�Giles ���������������������� f�ng1-shui3
Tongyong Pinyin ������������� fongshuěi
Yale Romanization ��������� fēngshwěi
IPA ��������������������������������������� [fə́ŋ.ʂwèɪ]
Wu
Romanization ������������������� fon平
sy上
Gan
Romanization ������������������� Fung1
sui3
Hakka
Romanization ������������������� fung24
sui31
Yue: Cantonese
Yale Romanization ��������� f�ngs�ui
or fūngs�ui
Jyutping ����������������������������� fung1seoi2
IPA ��������������������������������������� [fôŋ.sɵ̌y]
or [fóŋ.sɵ̌y]
Southern Min
Hokkien POJ hong-su�
Eastern Min
Fuzhou BUC ���������������������� hŭng-cūi
Vietnamese name
Vietnamese ���������������������� phong
thủy
H�n-N�m 風水
Thai name
Thai ������������������������������������� ฮวงจุ้ย
(Huang chui)
Korean name
Hangul �������������������������������� 풍수
Hanja ���������������������������������� 風水
Transcriptions
Revised Romanization ������������������ pungsu
McCune�Reischauer ��������������������� p'ungsu
Japanese name
Kanji ���������������������������������������������������� 風水
Hiragana �������������������������������������������� ふうすい
Transcriptions
Revised Hepburn ���������������������������� fūsui
Kunrei-shiki �������������������������������������� h�sui
Filipino name
Tagalog ����������������������������������������������� Pungs�y,
Puns�y
Khmer name
Khmer ������������������������������������������������� ហុងស៊ុយ
(hongsaouy)
Historically, as well as in many
parts of the contemporary Chinese world, feng shui was used to orient buildings
and spiritually significant structures such as tombs, as well as dwellings and
other structures. One scholar writes that in contemporary Western societies,
however, �feng shui tends to be reduced to interior design for health and
wealth. It has become increasingly visible through 'feng shui consultants' and
corporate architects, who charge large sums of money for their analysis,
advice, and design.�
Feng shui has been identified as
both non-scientific and pseudoscientific by scientists and philosophers, and
has been described as a paradigmatic example of pseudoscience. It exhibits a
number of classic pseudoscientific aspects, such as making claims about the
functioning of the world which are not amenable to testing with the scientific
method. Some users of feng shui may be trying to gain a sense of security or
control. Their motivation is similar to the reasons that some people consult
fortune-tellers.
HISTORY
ORIGINS
As of 2013, the Yangshao and
Hongshan cultures provide the earliest known evidence for the use of feng shui.
Until the invention of the magnetic compass, feng shui relied on astronomy to
find correlations between humans and the universe.
In 4000 BC, the doors of
dwellings in Banpo were aligned with the asterism Yingshi just after the winter
solstice�this sited the homes for solar gain. During the Zhou era, Yingshi was
known as Ding and it was used to indicate the appropriate time to build a
capital city, according to the Shijing. The late Yangshao site at Dadiwan (c.
3500�3000 BC) includes a palace-like building (F901) at its center. The
building faces south and borders a large plaza. It stands on a north�south axis
with another building that apparently housed communal activities. Regional
communities may have used the complex.
A grave at Puyang (around 4000
BC) that contains mosaics� a Chinese star map of the Dragon and Tiger asterisms
and Beidou (the Big Dipper, Ladle or Bushel)� is oriented along a north�south
axis. The presence of both round and square shapes in the Puyang tomb, at
Hongshan ceremonial centers and at the late Longshan settlement at Lutaigang,
suggests that gaitian cosmography (heaven-round, earth-square) existed in
Chinese society long before it appeared in the Zhoubi Suanjing.
Cosmography that bears a
resemblance to modern feng shui devices and formulas appears on a piece of jade
unearthed at Hanshan and dated around 3000 BC. Archaeologist Li Xueqin links
the design to the liuren astrolabe, zhinan zhen, and luopan.
Beginning with palatial
structures at Erlitou, all capital cities of China followed rules of feng shui
for their design and layout. During the Zhou era, the Kaogong ji (Chinese: 考工記;
"Manual of Crafts") codified these rules. The carpenter's manual Lu
ban jing (魯班經; "Lu ban's
manuscript") codified rules for builders. Graves and tombs also followed
rules of feng shui, from Puyang to Mawangdui and beyond. From the earliest
records, the structures of the graves and dwellings seem to have followed the
same rules.
EARLY INSTRUMENTS AND TECHNIQUES
Some of the foundations of feng
shui go back more than 3,500 years before the invention of the magnetic
compass. It originated in Chinese astronomy. Some current techniques can be
traced to Neolithic China, while others were added later (most notably the Han
dynasty, the Tang, the Song, and the Ming).
The astronomical history of feng
shui is evident in the development of instruments and techniques. According to
the Zhouli, the original feng shui instrument may have been a gnomon.
Chinese used circumpolar stars to
determine the north�south axis of settlements. This technique explains why
Shang palaces at Xiaotun lie 10� east of due north. In some of the cases, as
Paul Wheatley observed, they bisected the angle between the directions of the
rising and setting sun to find north. This technique provided the more precise
alignments of the Shang walls at Yanshi and Zhengzhou. Rituals for using a feng
shui instrument required a diviner to examine current sky phenomena to set the
device and adjust their position in relation to the device.
The oldest examples of
instruments used for feng shui are liuren astrolabes, also known as shi. These
consist of a lacquered, two-sided board with astronomical sightlines. The
earliest examples of liuren astrolabes have been unearthed from tombs that date
between 278 BC and 209 BC. Along with divination for Da Liu Ren the boards were
commonly used to chart the motion of Taiyi through the nine palaces. The
markings on a liuren/shi and the first magnetic compasses are virtually
identical.
The magnetic compass was invented
for feng shui and has been in use since its invention.
Traditional feng shui
instrumentation consists of the Luopan or the earlier south-pointing spoon (指南針
zhinan zhen)�though a conventional compass could suffice if one understood the
differences. A feng shui ruler (a later invention) may also be employed.
A feng shui spiral at Los Angeles
Chinatown's Metro station
DEFINITION AND CLASSIFICATION
The goal of feng shui as
practiced today is to situate the human-built environment on spots with good
qi, an imagined form of "energy". The "perfect spot" is a
location and an axis in time.
Traditional feng shui is inherently
a form of ancestor worship. Popular in farming communities for centuries, it
was built on the idea that the ghosts of ancestors and other independent,
intangible forces, both personal and impersonal, affected the material world,
and that these forces needed to be placated through rites and suitable burial
places, which the feng shui practitioner would assist with for a fee. The
primary underlying value was material success for the living.
According to Stuart Vyse, feng
shui is "a very popular superstition." The PRC government has also labeled
it as superstitious. Feng shui is classified as a pseudoscience since it
exhibits a number of classic pseudoscientific aspects such as making claims
about the functioning of the world which are not amenable to testing with the
scientific method. It has been identified as both non-scientific and
pseudoscientific by scientists and philosophers, and has been described as a
paradigmatic example of pseudoscience.
Qi (ch'i)
FOUNDATIONAL CONCEPTS
A traditional turtle-back tomb of
southern Fujian, surrounded by an omega-shaped ridge protecting it from the
"noxious winds" from the three sides
Qi (气,
pronounced "chee") is a movable positive or negative life force which
plays an essential role in feng shui. The Book of Burial says that burial takes
advantage of "vital qi". The goal of feng shui is to take advantage
of vital qi by appropriate siting of graves and structures.
POLARITY
Polarity is expressed in feng
shui as yin and yang theory. That is, it is of two parts: one creating an
exertion and one receiving the exertion. The development of this theory and its
corollary, five phase theory (five element theory), have also been linked with
astronomical observations of sunspot.
The Five Elements or Forces (wu
xing) � which, according to the Chinese, are metal, earth, fire, water, and
wood � are first mentioned in Chinese literature in a chapter of the classic
Book of History. They play a very important part in Chinese thought: �elements�
meaning generally not so much the actual substances as the forces essential to
human life. Earth is a buffer, or an equilibrium achieved when the polarities
cancel each other. While the goal of Chinese medicine is to balance yin and
yang in the body, the goal of feng shui has been described as aligning a city,
site, building, or object with yin-yang force fields.
Bagua (eight trigrams)
Eight diagrams known as bagua (or
pa kua) loom large in feng shui, and both predate their mentions in the Yijing
(or I Ching). The Lo (River) Chart (Luoshu) was developed first, and is
sometimes associated with Later Heaven arrangement of the bagua. This and the
Yellow River Chart (Hetu, sometimes associated with the Earlier Heaven bagua)
are linked to astronomical events of the sixth millennium BC, and with the Turtle
Calendar from the time of Yao. The Turtle Calendar of Yao (found in the Yaodian
section of the Shangshu or Book of Documents) dates to 2300 BC, plus or minus
250 years.
In Yaodian, the cardinal
directions are determined by the marker-stars of the mega-constellations known
as the Four Celestial Animals:
East: The Azure Dragon (Spring equinox)�Niao (Bird 鳥),
α Scorpionis
South: The Vermilion Bird (Summer solstice)�Huo (Fire 火),
α Hydrae
West: The White Tiger (Autumn equinox)�Mǎo (Hair 毛),
η Tauri (the Pleiades)
North: The Black Tortoise (Winter solstice)�Xū
(Emptiness, Void 虛), α Aquarii, β
Aquarii
The diagrams are also linked with
the sifang (four directions) method of divination used during the Shang
dynasty. The sifang is much older, however. It was used at Niuheliang, and
figured large in Hongshan culture's astronomy. And it is this area of China
that is linked to Yellow Emperor (Huangdi) who allegedly invented the south-pointing
spoon (see compass).
Traditional feng shui is an
ancient system based upon the observation of heavenly time and earthly space.
Literature, as well as archaeological evidence, provide some idea of the
origins and nature of feng shui techniques. Aside from books, there is also a
strong oral history. In many cases, masters have passed on their techniques
only to selected students or relatives.
Modern practitioners of feng shui
draw from several branches in their own practices.
FORM BRANCH
The Form Branch is the oldest
branch of feng shui. Qing Wuzi in the Han dynasty describes it in the Book of
the Tomb and Guo Pu of the Jin dynasty follows up with a more complete
description in The Book of Burial.
The Form branch was originally
concerned with the location and orientation of tombs (Yin House feng shui),
which was of great importance. The branch then progressed to the consideration
of homes and other buildings (Yang House feng shui).
The "form" in Form
branch refers to the shape of the environment, such as mountains, rivers,
plateaus, buildings, and general surroundings. It considers the five celestial
animals (phoenix, green dragon, white tiger, black turtle, and the yellow
snake), the yin-yang concept and the traditional five elements (Wu Xing: wood,
fire, earth, metal, and water).
The Form branch analyzes the
shape of the land and flow of the wind and water to find a place with ideal qi.
It also considers the time of important events such as the birth of the
resident and the building of the structure.
COMPASS BRANCH
The Compass branch is a
collection of more recent feng shui techniques based on the Eight Directions,
each of which is said to have unique qi. It uses the Luopan, a disc marked with
formulas in concentric rings around a magnetic compass.
TRADITIONAL FENG SHUI
The Compass Branch includes
techniques such as Flying Star and Eight Mansions.
More recent forms of feng shui
simplify principles that come from the traditional branches, and focus mainly
on the use of the bagua.
ASPIRATIONS METHOD
The Eight Life Aspirations style
of feng shui is a simple system which coordinates each of the eight cardinal
directions with a specific life aspiration or station such as family, wealth,
fame, etc., which come from the Bagua government of the eight aspirations. Life
Aspirations is not otherwise a geomantic system.
Ti Li (Form Branch)
Popular Xingshi Pai (形勢派)
"forms" methods
Luan Tou Pai, 巒頭派, Pinyin:
lu�n t�u p�i, (environmental analysis without using a compass)
Xing Xiang Pai, 形象派 or 形像派,
Pinyin: x�ng xi�ng p�i, (Imaging forms)
Xingfa Pai, 形法派, Pinyin:
x�ng fǎ p�i
Liiqi Pai (Compass Branch)
Popular Liiqi Pai (理气派)
"Compass" methods
San Yuan Method, 三元派 (Pinyin:
sān yu�n p�i)
Dragon Gate Eight Formation, 龍門八法
(Pinyin: l�ng m�n bā fǎ)
Xuan Kong, 玄空 (time and space
methods)
Xuan Kong Fei Xing 玄空飛星
(Flying Stars methods of time and directions)
Xuan Kong Da Gua, 玄空大卦
("Secret Decree" or 64 gua relationships)
Xuan Kong Mi Zi, 玄空秘旨
(Mysterious Space Secret Decree)
Xuan Kong Liu Fa, 玄空六法
(Mysterious Space Six Techniques)
Western forms of feng shui
List of specific feng shui branches
Zi Bai Jue, 紫白訣 (Purple
White Scroll)
San He Method, 三合派
(environmental analysis using a compass)
Accessing Dragon Methods
Ba Zhai, 八宅 (Eight Mansions)
Yang Gong Feng Shui, 楊公風水
Water Methods, 河洛水法
Local Embrace
Others
Yin House Feng Shui, 陰宅風水
(Feng Shui for the deceased)
Four Pillars of Destiny, 四柱命理
(a form of hemerology)
Zi Wei Dou Shu, 紫微斗數
(Purple Star Astrology)
I-Ching, 易經 (Book of Changes)
Qi Men Dun Jia, 奇門遁甲
(Mysterious Door Escaping Techniques)
Da Liu Ren, 大六壬
(Divination: Big Six Heavenly Yang Water Qi)
Tai Yi Shen Shu, 太乙神數
(Divination: Tai Yi Magical Calculation Method)
Date Selection, 擇日 (Selection of
auspicious dates and times for important events)
Chinese Palmistry, 掌相學 (Destiny
reading by palm reading)
Chinese Face Reading, 面相學 (Destiny
reading by face reading)
Major & Minor Wandering Stars (Constellations)
Five phases, 五行 (relationship of
the five phases or wuxing)
BTB Black (Hat) Tantric Buddhist
Sect (Westernised or Modern methods not based on Classical teachings)
Symbolic Feng Shui, (New Age Feng
Shui methods that advocate substitution with symbolic (spiritual, appropriate
representation of five elements) objects if natural environment or object/s
is/are not available or viable)
Pierce Method of Feng Shui
(Sometimes Pronounced: Von Shway) The practice of melding striking with
soothing furniture arrangements to promote peace and prosperity
After Richard Nixon's visit to
the People's Republic of China in 1972, feng shui became popular in the United
States. Critics, however, warn that attempts to prove its power scientifically
have shown that it is a pseudoscience. Others charge that it has been
reinvented and commercialized by New Age entrepreneurs or are concerned that
much of the traditional theory has been lost in translation, not paid proper
consideration, frowned upon, or even scorned.
Feng shui, however, has
nonetheless found many uses. Landscape ecologists often find traditional feng
shui an interesting study. In many cases, the only remaining patches of Asian
old forest are "feng shui woods", associated with cultural heritage,
historical continuity, and the preservation of various flora and fauna species.
Some researchers interpret the presence of these woods as indicators that the
"healthy homes", sustainability and environmental components of
traditional feng shui should not be easily dismissed. Environmental scientists
and landscape architects have researched traditional feng shui and its
methodologies. Architects study feng shui as an Asian architectural tradition.
Geographers have analyzed the techniques and methods to help locate historical
sites in Victoria, British Columbia, Canada, and archaeological sites in the
American Southwest, concluding that Native Americans also considered astronomy
and landscape features.
Believers use it for healing
purposes though there is no empirical evidence that it is in any way effective,
to guide their businesses, or create a peaceful atmosphere in their homes. In
particular, they use feng shui in the bedroom, where a number of techniques
involving colors and arrangement achieve comfort and peaceful sleep. Some users
of feng shui may be trying to gain a sense of security or control, such as by
choosing auspicious numbers for their phones or Contemporary uses of
traditional feng shui
A modern "feng shui
fountain" at Taipei 101, Taiwan favorable house locations. Their
motivation is similar to the reasons that some people consult fortune-tellers.
In 2005, Hong Kong Disneyland
acknowledged feng shui as an important part of Chinese culture by shifting the
main gate by twelve degrees in their building plans. This was among actions
suggested by the planner of architecture and design at Walt Disney
Imagineering, Wing Chao.
At Singapore Polytechnic and
other institutions, professionals including engineers, architects, property
agents and interior designers, take courses on feng shui and divination every
year, a number of whom becoming part-time or full-time feng shui consultants.
TRADITIONAL FENG SHUI
Matteo Ricci (1552�1610), one of
the founding fathers of Jesuit China missions, may have been the first European
to write about feng shui practices. His account in De Christiana expedition
apud Sinas tells about feng shui masters (geologi, in Latin) studying
prospective construction sites or grave sites "with reference to the head
and the tail and the feet of the particular dragons which are supposed to dwell
beneath that spot". As a Catholic missionary, Ricci strongly criticized
the "recondite science" of geomancy along with astrology as yet another
superstitio absurdissima of the heathens: "What could be more absurd than
their imagining that the safety of a family, honors, and their entire existence
must depend upon such trifles as a door being opened from one side or another,
as rain falling into a courtyard from the right or from the left, a window
opened here or there, or one roof being higher than another?"
Victorian-era commentators on
feng shui were generally ethnocentric, and as such skeptical and derogatory of what
they knew of feng shui. In 1896, at a meeting of the Educational Association of
China, Rev. P. W. Pitcher railed at the "rottenness of the whole scheme of
Chinese architecture," and urged fellow missionaries "to erect
unabashedly Western edifices of several stories and with towering spires in
order to destroy nonsense about fung-shuy".
CRITICISMS
After the founding of the
People's Republic of China in 1949, feng shui was officially considered a
"feudalistic superstitious practice" and a "social evil"
according to the state's ideology and was discouraged and even banned outright
at times. Feng shui remained popular in Hong Kong, and also in the Republic of
China (Taiwan), where traditional culture was not suppressed.
During the Cultural Revolution
(1966-1976) feng shui was classified as one of the so-called Four Olds that
were to be wiped out. Feng shui practitioners were beaten and abused by Red
Guards and their works burned. After the death of Mao Zedong and the end of the
Cultural Revolution, the official attitude became more tolerant but
restrictions on feng shui practice are still in place in today's China. It is
illegal in the PRC today to register feng shui consultation as a business and
similarly advertising feng shui practice is banned. There have been frequent
crackdowns on feng shui practitioners on the grounds of "promoting
feudalistic superstitions" such as one in Qingdao in early 2006 when the
city's business and industrial administration office shut down an art gallery
converted into a feng shui practice. Some officials who had consulted feng shui
were terminated and expelled from the Communist Party.
In 21st century mainland China
less than one-third of the population believe in feng shui, and the proportion
of believers among young urban Chinese is said to be even lower. Chinese
academics permitted to research feng shui are anthropologists or architects by
profession, studying the history of feng shui or historical feng shui theories
behind the design of heritage buildings. They include Cai Dafeng,
Vice-President of Fudan University. Learning in order to practice feng shui is
still somewhat considered taboo. Nevertheless, it is reported that feng shui
has gained adherents among Communist Party officials according to a BBC Chinese
news commentary in 2006, and since the beginning of Chinese economic reforms
the number of feng shui practitioners is increasing.
CONTEMPORARY FENG SHUI
SYCEE-SHAPED INCENSE USED IN FENG
SHUI
One critic called the situation
of feng shui in today's world "ludicrous and confusing," asking
"Do we really believe that mirrors and flutes are going to change people's
tendencies in any lasting and meaningful way?" He called for much further
study or "we will all go down the tubes because of our inability to match
our exaggerated claims with lasting changes." Robert T.
Carroll sums up the charges:
...feng shui has become an aspect
of interior decorating in the Western world and alleged masters of feng shui
now hire themselves out for hefty sums to tell people such as Donald Trump
which way his doors and other things should hang. Feng shui has also become
another New Age "energy" scam with arrays of metaphysical
products...offered for sale to help you improve your health, maximize your
potential, and guarantee fulfillment of some fortune cookie philosophy.
Skeptics charge that evidence for
its effectiveness is based primarily upon anecdote and users are often offered
conflicting advice from different practitioners, though feng shui practitioners
use these differences as evidence of variations in practice or different
branches of thought. A critical analyst concluded that "Feng shui has
always been based upon mere guesswork".
Another objection was to the
compass, a traditional tool for choosing favorable locations for property or
burials. Critics point out that the compass degrees are often inaccurate
because solar winds disturb the electromagnetic field of the earth. Magnetic
North on the compass will be inaccurate because true magnetic north fluctuates.
The American magicians Penn and
Teller dedicated an episode of their Bullshit! television show to criticize the
acceptance of feng shui in the Western world as science. They devised a test in
which the same dwelling was visited by five different feng shui consultants:
each produced a different opinion about the dwelling, showing there is no
consistency in the professional practice of feng shui.
Feng shui is criticized by Christians
around the world. Some have argued that it is "entirely inconsistent with
Christianity to believe that harmony and balance result from the manipulation
and channeling of nonphysical forces or energies, or that such can be done by
means of the proper placement of physical objects. Such techniques, in fact,
belong to the world of sorcery.
Feng shui practitioners in China
have found officials that are considered superstitious and corrupt easily
interested, despite official disapproval. In one instance, in 2009, county
officials in Gansu, on the advice of feng shui practitioners, spent $732,000 to
haul a 369-ton "spirit rock" to the county seat to ward off "bad
luck". Feng shui may require social influence or money because experts,
architecture or design changes, and moving from place to place is expensive.
Less influential or less wealthy
people lose faith in feng shui, saying that it is a game only for the wealthy.
Others, however, practice less expensive forms of feng shui, including hanging
special (but cheap) mirrors, forks, or woks in doorways to deflect negative
energy.
(back
to content)
1.2.3.4 Qigong w
Qigong (/ˈtʃiːˈɡɒŋ/),
qi gong, chi kung, chi 'ung, or chi gung (simplified Chinese: 气功;
traditional Chinese: 氣功; pinyin:
q�gōng; Wade�Giles: ch�i kung; lit. 'life-energy cultivation') is a system
of coordinated body-posture and movement, breathing, and meditation used for
the purposes of health, spirituality, and martial-arts training. With roots in
Chinese medicine, philosophy, and martial arts, qigong is traditionally viewed
by the Chinese and throughout Asia as a practice to cultivate and balance qi (pronounced
approximately as "chi" or "chee"), translated as "life
energy".
Qigong
Qigong practitioners at World Tai Chi and Qigong Day event
in Manhattan.
Chinese name
Traditional Chinese ������������������������������������������������������� 氣功
Simplified Chinese ��������������������������������������������������������� 气功
Transcriptions
Standard Mandarin
Hanyu Pinyin �������������������������������������������������������������������� q�gōng
Wade�Giles ���������������������������������������������������������������������� ch�i
kung
Tongyong Pinyin ������������������������������������������������������������� c�gōng
Yale Romanization ��������������������������������������������������������� ch�gūng
IPA ��������������������������������������������������������������������������������������� [tɕʰîkʊ́ŋ]
Wu
Romanization ������������������������������������������������������������������� chi去
khon平
Yue: Cantonese
Yale Romanization ��������������������������������������������������������� hei
gūng
Jyutping ����������������������������������������������������������������������������� hei3
gung1
IPA ��������������������������������������������������������������������������������������� [hēi.kʊ́ŋ]
Southern Min
Hokkien POJ ��������������������������������������������������������������������� kh�-kong
Qigong practice typically
involves moving meditation, coordinating slow-flowing movement, deep rhythmic
breathing, and a calm meditative state of mind. People practice qigong
throughout China and worldwide for recreation, exercise, relaxation, preventive
medicine, self-healing, alternative medicine, meditation, self-cultivation, and
training for martial arts.
Qigong (Pinyin), ch'i kung
(Wade-Giles), and chi gung (Yale) are Romanized words for two Chinese
characters: q� (气/氣) and
gōng (功).
Qi (or chi) primarily means air,
gas or breath but is often translated as a metaphysical concept of 'vital
energy', referring to a supposed energy circulating through the body; though a
more general definition is universal energy, including heat, light, and
electromagnetic energy; and definitions often involve breath, air, gas, or the
relationship between matter, energy, and spirit.
Qi is the central underlying
principle in traditional Chinese medicine and martial arts. Gong (or kung) is
often translated as cultivation or work, and definitions include practice,
skill, mastery, merit, achievement, service, result, or accomplishment, and is
often used to mean gongfu (kung fu) in the traditional sense of achievement
through great effort. The two words are combined to describe systems to
cultivate and balance life energy, especially for health and wellbeing.
Etymology
The term qigong as currently used
was promoted in the late 1940s through the 1950s to refer to a broad range of
Chinese self-cultivation exercises, and to emphasize health and scientific
approaches, while de-emphasizing spiritual practices, mysticism, and elite
lineages.
With roots in
ancient Chinese culture dating back more than 4,000 years, a wide variety of
qigong forms have developed within different segments of Chinese society: in
traditional Chinese medicine for preventive and curative functions; in
Confucianism to promote longevity and improve moral character; in Daoism and
Buddhism as part of meditative practice; and in Chinese martial arts to enhance
self defending abilities. Contemporary qigong blends diverse and sometimes
disparate traditions, in particular the Daoist meditative practice of
"internal alchemy" (Neidan 內丹術), the
ancient meditative practices of "circulating qi" (Xing qi 行氣)
and "standing meditation" (Zhan zhuang 站桩),
and the slow gymnastic breathing exercise of "guiding and pulling"
(Dao yin 導引). Traditionally, qigong was taught by
master to students through training and oral transmission, with an emphasis on
meditative practice by scholars and gymnastic or dynamic practice by the
working masses.
Starting in the late 1940s and
the 1950s, the mainland Chinese government tried to integrate disparate qigong
approaches into one coherent system, with the intention of establishing a firm
scientific basis for qigong practice. In 1949, Liu Guizhen established the name
"Qigong" to refer to the system of life-preserving practices that he
and his associates developed, based on Dao yin and other philosophical traditions.
This attempt is considered by some sinologists as the History and origins
�
The physical exercise chart; a
painting on silk depicting the practice of Qigong Taiji; unearthed in 1973 in
Hunan Province, China, from the 2nd-century BC Western Han burial site of
Mawangdui Han tombs site, Tomb Number 3.
With roots in
ancient Chinese culture dating back more than 4,000 years, a wide variety of
qigong forms have developed within different segments of Chinese society: in
traditional Chinese medicine for preventive and curative functions; in
Confucianism to promote longevity and improve moral character; in Daoism and
Buddhism as part of meditative practice; and in Chinese martial arts to enhance
self defending abilities. Contemporary qigong blends diverse and sometimes
disparate traditions, in particular the Daoist meditative practice of
"internal alchemy" (Neidan 內丹術), the
ancient meditative practices of "circulating qi" (Xing qi 行氣)
and "standing meditation" (Zhan zhuang 站桩),
and the slow gymnastic breathing exercise of "guiding and pulling"
(Dao yin 導引). Traditionally, qigong was taught by
master to students through training and oral transmission, with an emphasis on
meditative practice by scholars and gymnastic or dynamic practice by the
working masses.
Starting in the late 1940s and
the 1950s, the mainland Chinese government tried to integrate disparate qigong
approaches into one coherent system, with the intention of establishing a firm
scientific basis for qigong practice. In 1949, Liu Guizhen established the name
"Qigong" to refer to the system of life-preserving practices that he
and his associates developed, based on Dao yin and other philosophical
traditions. This attempt is considered by some sinologists as the start of the
modern or scientific interpretation of qigong. During the Great Leap Forward
(1958�1963) and the Cultural Revolution (1966�1976), qigong, along with other
traditional Chinese medicine, was under tight control with limited access among
the general public, but was encouraged in state-run rehabilitation centers and
spread to universities and hospitals.
After the Cultural Revolution,
qigong, along with t'ai chi, was popularized as daily morning exercise
practiced en masse throughout China.
Popularity of qigong grew rapidly
during the Deng and Jiang eras after Mao Zedong's death in 1976 through the
1990s, with estimates of between 60 and 200 million practitioners throughout
China. Along with popularity and state sanction came controversy and problems:
claims of extraordinary abilities bordering on the supernatural, pseudoscience
explanations to build credibility, a mental condition labeled qigong deviation,
formation of cults, and exaggeration of claims by masters for personal benefit.
In 1985, the state-run National Qigong Science and Research Organization was
established to regulate the nation's qigong denominations. In 1999, in response
to widespread revival of old traditions of spirituality, morality, and
mysticism, and perceived challenges to State control, the Chinese government took
measures to enforce control of public qigong practice, including shutting down
qigong clinics and hospitals, and banning groups such as Zhong Gong and Falun
Gong.: 161�174
Since the 1999 crackdown, qigong
research and practice have only been officially supported in the context of
health and traditional Chinese medicine. The Chinese Health Qigong Association,
established in 2000, strictly regulates public qigong practice, with limitation
of public gatherings, requirement of state approved training and certification
of instructors, and restriction of practice to stateapproved forms.
Through the forces of migration
of the Chinese diaspora, tourism in China, and globalization, the practice of
qigong spread from the Chinese community to the world. Today, millions of
people around the world practice qigong and believe in the benefits of qigong
to varying degrees. Similar to its historical origin, those interested in
qigong come from diverse backgrounds and practice it for different reasons,
including for recreation, exercise, relaxation, preventive medicine,
selfhealing, alternative medicine, self-cultivation, meditation, spirituality,
and martial arts training.
PRACTICES
OVERVIEW
Qigong comprises a diverse set of
practices that coordinate body (調身), breath (調息),
and mind (調心) based on Chinese philosophy.
Practices include moving and still meditation, massage, chanting, sound
meditation, and non-contact treatments, performed in a broad array of body
postures. Qigong is commonly classified into two foundational categories: 1)
dynamic or active qigong (dong gong), with slow flowing movement; and 2)
meditative or passive qigong (jing gong), with still positions and inner
movement of the breath.: 21770�21772 From a therapeutic perspective, qigong can
be classified into two systems:
1) internal qigong, which focuses
on self-care and self-cultivation, and;
2) external qigong, which
involves treatment by a therapist who directs or transmits qi.: 21777�21781
As moving meditation, qigong
practice typically coordinates slow stylized movement, deep diaphragmatic
breathing, and calm mental focus, with visualization of guiding qi through the
body. While implementation details vary, generally qigong forms can be
characterized as a mix of four types of practice: dynamic, static, meditative,
and activities requiring external aids.
Dynamic practice involves fluid
movement, usually carefully choreographed, coordinated with breath and
awareness. Examples include the slow stylized movements of T'ai chi ch'uan,
Baguazhang, and Xing Yi Quan. Other examples include graceful movement that
mimics the motion of animals in Five Animals (Wu Qin Xi qigong), White Crane,
and Wild Goose (Dayan) Qigong. As a form of gentle exercise, qigong is composed
of movements that are typically repeated, strengthening and stretching the
body, increasing fluid movement (blood, synovial, and lymph), enhancing balance
and proprioception, and improving the awareness of how the body moves through
space.
Static practice involves holding
postures for sustained periods of time. In some cases, this bears resemblance
to the practice of Yoga and its continuation in the Buddhist tradition. For
example, Yiquan, a Chinese martial art derived from xingyiquan, emphasizes
static stance training. In another example, the healing form Eight Pieces of
Brocade (Baduanjin qigong) is based on a series of static postures.
Meditative practice utilizes
breath awareness, visualization, mantra, chanting, sound, and focus on
philosophical concepts such as qi circulation, aesthetics, or moral values. In
traditional Chinese medicine and Daoist practice, the meditative focus is
commonly on cultivating qi in dantian energy centers and balancing qi flow in
meridian and other pathways. In various Buddhist traditions, the aim is to
still the mind, either through outward focus, for example on a place, or
through inward focus on the breath, a mantra, a koan, emptiness, or the idea of
the eternal. In the Confucius scholar tradition, meditation is focused on
humanity and virtue, with the aim of selfenlightenment.
USE OF EXTERNAL AGENTS
Many systems of qigong practice
include the use of external agents such as ingestion of herbs, massage,
physical manipulation, or interaction with other living organisms. For example,
specialized food and drinks are used in some medical and Daoist forms, whereas
massage and body manipulation are sometimes used in martial arts forms. In some
medical systems a qigong master uses non-contact treatment, purportedly guiding
qi through his or her own body into the body of another person.
FORMS
There are numerous qigong forms.
75 ancient forms that can be found in ancient literature and also 56 common or
contemporary forms have been described in a qigong compendium.: 203�433 The
list is by no means exhaustive. Many contemporary forms were developed by
people who had recovered from their illness after qigong practice.
Most of the qigong forms come under the following
categories:
1. Medical qigong
2. Martial qigong
3. Spiritual qigong
4. Intellectual qigong
5. Life nourishing qigong
Development of "health qigong"
In 1995, there was Qigong Talent
Bank, an organization of Science Research of Chinese Qigong, functioning as
network system of the senior Chinese qigong talents in China. In order to
promote qigong exercises in a standardised and effective way with a scientific
approach, The Chinese Health Qigong Association (CHQA) appointed panels of
Qigong experts, Chinese medicine doctors and sport science professors from
different hospitals, universities and qigong lineage across China to research
and develop new sets of qigong exercises. In 2003 the CHQA officially promoted
a new system called "health qigong", which consisted of four newly
developed health qigong forms:
Health Qigong Muscle-Tendon Change Classic (Health Qigong Y�
Jīn Jīng 易筋經).
Health Qigong Five Animals Frolics (Health qigong Wu Qin Xi 五禽戲).
Health Qigong Six Healing Sounds (Health Qigong Liu Zi Jue 六字訣).
Health Qigong Eight Pieces of Brocade (Health Qigong Ba Duan
Jin 八段錦).
In 2010, the Chinese Health Qigong Association officially
introduced five additional health qigong forms:
Health Qigong Tai Chi Yang Sheng Zhang (太極養生杖):
a tai chi form from the stick tradition.
Health Qigong Shi Er Duan Jin (十二段錦):
seated exercises to strengthen the neck, shoulders, waist, and legs.
Health Qigong Daoyin Yang Sheng Gong Shi Er Fa (導引養生功十二法):
12 routines from Daoyin tradition of guiding and pulling qi.
Health Qigong Mawangdui Daoyin (馬王堆導引术):
guiding qi along the meridians with synchronous movement and awareness.
Health Qigong Da Wu (大舞): choreographed
exercises to lubricate joints and guide qi.
Other commonly practised qigong styles and forms include:
Soaring Crane Qigong
Wisdom Healing Qigong
Pan Gu Mystical Qigong
Wild Goose (Dayan) Qigong
Dragon and Tiger Qigong
Primordial Qigong (Wujigong)
Chilel Qigong
Phoenix Qigong
Yuan Qigong
Zhong Yuan Qigong
TECHNIQUES
Whether viewed from the
perspective of exercise, health, philosophy, or martial arts training, several
main principles emerge concerning the practice of qigong:
Intentional movement: careful,
flowing balanced style Rhythmic breathing: slow, deep, coordinated with fluid
movement
Awareness: calm, focused meditative state
Visualization: of qi flow, philosophical tenets, aesthetics
Chanting/Sound: use of sound as a focal point
Additional principles:
Softness: soft gaze, expressionless face
Solid Stance: firm footing, erect spine
Relaxation: relaxed muscles, slightly bent joints
Balance and Counterbalance: motion over the center of
gravity
Advanced goals:
Equanimity: more fluid, more relaxed
Tranquility: empty mind, high awareness
Stillness: smaller and smaller movements, eventually to
complete stillness
The most advanced practice is generally considered to be
with little or no motion.
TRADITIONAL AND CLASSICAL THEORY
Qigong practitioners in Brazil
Over time, five distinct
traditions or schools of qigong developed in China, each with its own theories
and characteristics: Chinese Medical Qigong, Daoist Qigong, Buddhist Qigong,
Confucian Qigong, and Martial Qigong.: 30�80 All of these qigong traditions
include practices intended to cultivate and balance qi.
TRADITIONAL CHINESE MEDICINE
The theories of ancient Chinese
qigong include the Yin-Yang and Five Phases Theory, Essence-Qi-Spirit Theory,
Zang-Xiang Theory, and Meridians and Qi-Blood Theory, which have been
synthesized as part of Traditional Chinese Medicine (TCM).: 45�57 TCM focuses
on tracing and correcting underlying disharmony, in terms of deficiency and
excess, using the complementary and opposing forces of yin and yang (陰陽),
to create a balanced flow of qi. Qi is believed to be cultivated and stored in
three main dantian energy centers and to travel through the body along twelve
main meridians (Jīng Lu� 經絡), with numerous
smaller branches and tributaries. The main meridians correspond to twelve main
organs ) (Z�ng fǔ 臟腑). Qi is balanced
in terms of yin and yang in the context of the traditional system of Five
Phases (Wu xing 五行). A person is believed to become ill
or die when qi becomes diminished or unbalanced. Health is believed to be
returned by rebuilding qi, eliminating qi blockages, and correcting qi
imbalances. These TCM concepts do not translate readily to modern science and
medicine.
Daoism
In Daoism, various practices now
known as Daoist qigong are claimed to provide a way to achieve longevity and
spiritual enlightenment, as well as a closer connection with the natural world.
Buddhism
In Buddhism meditative practices
now known as Buddhist qigong are part of a spiritual path that leads to
spiritual enlightenment or Buddhahood.
Confucianism
In Confucianism practices now
known as Confucian qigong provide a means to become a Junzi (君子)
through awareness of morality.
In contemporary China, the
emphasis of qigong practice has shifted away from traditional philosophy,
spiritual attainment, and folklore, and increasingly to health benefits,
traditional medicine and martial arts applications, and a scientific
perspective. Qigong is now practiced by millions worldwide, primarily for its
health benefits, though many practitioners have also adopted traditional
philosophical, medical, or martial arts perspectives, and even use the long
history of qigong as evidence of its effectiveness.
CONTEMPORARY CHINESE MEDICAL
QIGONG
Qigong has been recognized as a
"standard medical technique" in China since 1989, and is sometimes
included in the medical curriculum of major universities in China.: 34 The 2013
English translation of the official Chinese Medical Qigong textbook used in
China: iv, 385 defines CMQ as "the skill of body-mind exercise that
integrates body, breath, and mind adjustments into one" and emphasizes
that qigong is based on "adjustment" (tiao 調,
also translated as "regulation", "tuning", or "alignment")
of body, breath, and mind.: 16�18 As such, qigong is viewed by practitioners as
being more than common physical exercise, because qigong combines postural,
breathing, and mental training in one to produce a particular
psychophysiological state of being.: 15 While CMQ is still based on traditional
and classical theory, modern practitioners also emphasize the importance of a
strong scientific basis.: 81�89
According to the 2013 CMQ
textbook, physiological effects of qigong are numerous, and include improvement
of respiratory and cardiovascular function, and possibly neurophysiological
function.: 89�102
CONVENTIONAL MEDICINE
Especially since the 1990s,
conventional or mainstream Western medicine often strives to heed the model of
evidence-based medicine, EBM, which demotes medical theory, clinical
experience, and physiological data to prioritize the results of controlled, and
especially randomized, clinical trials of the treatment itself. Although some
clinical trials support qigong's effectiveness in treating conditions diagnosed
in Western medicine, the quality of these studies is mostly low and, overall,
their results are mixed.
Integrative, complementary, and
alternative medicine
CONTEMPORARY QIGONG
Integrative medicine (IM) refers
to "the blending of conventional and complementary medicines and therapies
with the aim of using the most appropriate of either or both modalities to care
for the patient as a whole",: 455�456 whereas complementary is using a
non-mainstream approach together with conventional medicine, while alternative
is using a non-mainstream approach in place of conventional medicine. Qigong is
used by integrative medicine practitioners to complement conventional medical
treatment, based on complementary and alternative medicine interpretations of
the effectiveness and safety of qigong.: 22278�22306
SCIENTIFIC BASIS
Scientists interested in qigong
have sought to describe or verify the effects of qigong, to explore mechanisms
of effects, to form scientific theory with respect to qigong, and to identify
appropriate research methodology for further study.: 81�89 In terms of
traditional theory, the existence of qi has not been independently verified in
an experimental setting. In any case, some researches have reported effects on
pathophysiological parameters of biomedical interest.
RECREATION AND POPULAR USE
People practice qigong for many
different reasons, including for recreation, exercise and relaxation,
preventive medicine and self-healing, meditation and self-cultivation, and
training for martial arts. Practitioners range from athletes to people with
disabilities. Because it is low impact and can be done lying, sitting, or
standing, qigong is accessible for people with disabilities, seniors, and people
recovering from injuries.
THERAPEUTIC USE
Therapeutic use of qigong is
directed by TCM, CAM, integrative medicine, and other health practitioners. In
China, where it is considered a "standard medical technique",: 34
qigong is commonly prescribed to treat a wide variety of conditions, and
clinical applications include hypertension, coronary artery disease, peptic
ulcers, chronic liver diseases, diabetes mellitus, obesity, menopause syndrome,
chronic fatigue syndrome, insomnia, tumors and cancer, lower
Practitioners, uses and cautions
back and leg pain, cervical spondylosis, and myopia.: 261�391 Outside China
qigong is used in integrative medicine to complement or supplement accepted
medical treatments, including for relaxation, fitness, rehabilitation, and
treatment of specific conditions. However, there is no high-quality evidence
that qigong is actually effective for these conditions. Based on systematic
reviews of clinical research, there is insufficient evidence for the
effectiveness of using qigong as a therapy for any medical condition.
SAFETY AND COST
Qigong is generally viewed as
safe. No adverse effects have been observed in clinical trials, such that
qigong is considered safe for use across diverse populations. Cost for
self-care is minimal, and cost efficiencies are high for group delivered care. Typically,
the cautions associated with qigong are the same as those associated with any
physical activity, including risk of muscle strains or sprains, advisability of
stretching to prevent injury, general safety for use alongside conventional
medical treatments, and consulting with a physician when combining with
conventional treatment.
OVERVIEW
Although there is ongoing
clinical research examining the potential health effects of qigong, there is
little financial or medical incentive to support high-quality research, and
still only a limited number of studies meet accepted medical and scientific
standards of randomized controlled trials (RCTs). Clinical research concerning
qigong has been conducted for a wide range of medical conditions, including
bone density, cardiopulmonary effects, physical function, falls and related
risk factors, quality of life, immune function, inflammation, hypertension,
pain, and cancer treatment.
SYSTEMATIC REVIEWS
A 2009 systematic review on the
effect of qigong exercises on reducing pain concluded that "the existing
trial evidence is not convincing enough to suggest that internal qigong is an
effective modality for pain management."
CLINICAL RESEARCH
A 2010 systematic review of the
effect of qigong exercises on cancer treatment concluded "the
effectiveness of qigong in cancer care is not yet supported by the evidence from
rigorous clinical trials." A separate systematic review that looked at the
effects of qigong exercises on various physiological or psychological outcomes
found that the available studies were poorly designed, with a high risk of bias
in the results. Therefore, the authors concluded, "Due to limited number
of RCTs in the field and methodological problems and high risk of bias in the
included studies, it is still too early to reach a conclusion about the
efficacy and the effectiveness of qigong exercise as a form of health practice
adopted by the cancer patients during their curative, palliative, and
rehabilitative phases of the cancer journey."
A 2011 overview of systematic
reviews of controlled clinical trials, Lee et al. concluded that "the
effectiveness of qigong is based mostly on poor quality research" and
"therefore, it would be unwise to draw firm conclusions at this
stage." Although a 2010 comprehensive literature review found 77
peer-reviewed RCTs, Lee et al.'s overview of systematic reviews as to
particular health conditions found problems like sample size, lack of proper
control groups, with lack of blinding associated with high risk of bias.
A 2015 systematic review of the
effect of qigong exercises on cardiovascular diseases and hypertension found no
conclusive evidence for effect. Also in 2015, a systemic review into the
effects on hypertension suggested that it may be effective, but that the
evidence was not conclusive because of the poor quality of the trials it
included, and advised more rigorous research in the future. Another 2015
systematic review of qigong on biomarkers of cardiovascular disease concluded
that some trials showed favorable effects, but concludes, "Most of the
trials included in this review are likely to be at high risk of bias, so we
have very low confidence in the validity of the results.
MENTAL HEALTH
Many claims have been made that
qigong can benefit or ameliorate mental health conditions, including improved
mood, decreased stress reaction, and decreased anxiety and depression.
Most medical studies have only
examined psychological factors as secondary goals, although various studies
have shown decreases in cortisol levels, a chemical hormone produced by the
body in response to stress.
China
Basic and clinical research in
China during the 1980s was mostly descriptive, and few results were reported in
peer-reviewed English-language journals.: 22060�22063 Qigong became known
outside China in the 1990s, and clinical randomized controlled trials
investigating the effectiveness of qigong on health and mental conditions began
to be published worldwide, along with systematic reviews.: 21792�21798
CHALLENGES
Most existing clinical trials have
small sample sizes and many have inadequate controls. Of particular concern is
the impracticality of double blinding using appropriate sham treatments, and
the difficulty of placebo control, such that benefits often cannot be distinguished
from the placebo effect.: 22278�22306�
Also of concern is the choice of which qigong form to use and how to
standardize the treatment or amount with respect to the skill of the
practitioner leading or administering treatment, the tradition of
individualization of treatments, and the treatment length, intensity, and
frequency.: 6869�6920, 22361�22370
Qigong is practiced for
meditation and self-cultivation as part of various philosophical and spiritual
traditions. As meditation, qigong is a means to still the mind and enter a
state of consciousness that brings serenity, clarity, and bliss. Many
practitioners find qigong, with its gentle focused movement, to be more accessible
than seated meditation.
Qigong for self-cultivation can
be classified in terms of traditional Chinese philosophy: Daoist, Buddhist, and
Confucian. The practice of qigong is an important component in both internal
and external style Chinese martial arts. Focus on qi is considered to be a
source of power as well as the foundation of the internal style of martial arts
(Neijia). T'ai Chi Ch'uan, Xing Yi Quan, and Baguazhang are representative of
the types of Chinese martial arts that rely on the concept of qi as the
foundation. Extraordinary feats of martial arts prowess, such as the ability to
withstand heavy strikes (Iron Shirt, 鐵衫) and the ability
to break hard objects (Iron Palm, 鐵掌) are abilities
attributed to qigong training.
MEDITATION
AND SELF-CULTIVATION APPLICATIONS
Martial arts
applications
T'ai Chi
Ch'uan and qigong
T'ai Chi Ch'uan (Taijiquan) is a
widely practiced Chinese internal martial style based on the theory of taiji,
closely associated with qigong, and typically involving more complex
choreographed movement coordinated with breath, done slowly for health and
training, or quickly for selfdefense.
Many scholars consider t'ai chi
ch'uan to be a type of qigong, traced back to an origin in the seventeenth
century. In modern practice, qigong typically focuses more on health and
meditation rather than martial applications, and plays an important role in
training for t'ai chi ch'uan, in particular used to build strength, develop
breath control, and increase vitality ("life energy").
(back
to content)
1.2.3.5 Reflexology w
Reflexology, also known as zone
therapy, is an alternative medical practice involving the application of
pressure to specific points on the feet, ears, and/or hands. This is done using
thumb, finger, and hand massage techniques without the use of oil or lotion. It
is based on a pseudoscientific system of zones and reflex areas that
purportedly reflect an image of the body on the feet and hands, with the
premise that such work on the feet and hands causes a physical change to the
supposedly related areas of the body.
History
Practices resembling reflexology
may have existed in previous historical periods. Similar practices have been
documented in the histories of India, China and Egypt. Reflexology was
introduced to the United States in 1913 by William H. Fitzgerald, M.D.
(1872�1942), an ear, nose, and throat specialist, and Edwin F. Bowers.
Fitzgerald claimed that applying pressure had an anesthetic effect on other
areas of the body. It was modified in the 1930s and 1940s by Eunice D. Ingham
(1889�1974), a nurse and physiotherapist. Ingham claimed that the feet and
hands were especially sensitive, and mapped the entire body into
"reflexes" on the feet, renaming "zone therapy"
reflexology. Many of the modern reflexologists use Ingham's methods, or similar
techniques of reflexologist Laura Norman.
In 2015 the Australian
Government's Department of Health published the results of a review of
alternative therapies that sought to determine if any were suitable for being
covered by health insurance; reflexology was one of 17 therapies evaluated for
which no clear evidence of effectiveness was found. Accordingly, in 2017, the
Australian government named reflexology as a practice that would not qualify
for insurance subsidy, saying this step would "ensure taxpayer funds are
expended appropriately and not directed to therapies lacking evidence".
1.2.3.6 Shiatsu w
Shiatsu (/ʃiˈ�ts-,
-ˈɑːtsuː/ shee-AT-, -AHT-soo;
指圧)
is a form of Japanese bodywork based on pseudoscientific concepts in
traditional Chinese medicine such as qi meridians. Having been popularized in
the twentieth century by Tokujiro Namikoshi (1905�2000), shiatsu derives from
the older Japanese massage modality called anma.
Shiatsu
"Shiatsu" in new-style (shinjitai) kanji
Japanese name
Shinjitai ���������������������������������������������������������������������������������������������� 指圧
Transcriptions
Romanization ����������������������������������������������������������������������������������� Shiatsu
There is no scientific evidence
that shiatsu will prevent or cure any disease. Although it is considered a
generally safe treatment�if sometimes painful�there have been reports of
adverse health effects arising from its use, a few of them serious.
Description
In the Japanese language, shiatsu
means "finger pressure". Shiatsu techniques include massages with
fingers, thumbs, feet and palms; acupressure, assisted stretching; and joint manipulation
and mobilization. To examine a patient, a shiatsu practitioner uses palpation
and, sometimes, pulse diagnosis.
The Japanese Ministry of Health
defines shiatsu as "a form of manipulation by thumbs, fingers and palms
without the use of instruments, mechanical or otherwise, to apply pressure to
the human skin to correct internal malfunctions, promote and maintain health,
and treat specific diseases. The techniques used in shiatsu include stretching,
holding, and most commonly, leaning body weight into various points along key
channels."
The practice of shiatsu is based
on the traditional Chinese concept of qi, which is sometimes described as an
"energy flow". Qi is supposedly channeled through certain pathways in
the human body, known as meridians, causing a variety of effects. Despite the
fact that many practitioners use these ideas in explaining shiatsu, neither qi
nor meridians exist as observable phenomena.
Efficacy
There is no evidence that shiatsu
is of any benefit in treating cancer or any other disease, though some evidence
suggests it might help people feel more relaxed. In 2015, the Australian
Government's Department of Health published the results of a review of
alternative therapies that sought to determine if any were suitable for being
covered by health insurance; shiatsu was one of 17 therapies evaluated for
which no clear evidence of effectiveness was found.
Accordingly, in 2017, the
Australian government named shiatsu as a practice that would not qualify for
insurance subsidy, to ensure the best use of insurance funds.
History
 �
�
Shiatsu practitioners believe that an energy called ki flows
through a network of meridians in the body.
Shiatsu's claims of having a
positive impact on a recipient's sense of vitality and well-being have to some
extent been supported by studies where recipients reported improved relaxation,
sleep, and lessened symptom severity. However, the state of the evidence on its
efficacy for treating any malady is poor, and one recent systematic review did
not find shiatsu to be effective for any particular health condition. It is
generally considered safe, though some studies have reported negative effects after
a treatment with shiatsu, and examples of serious health complications exist
including one case of thrombosis, one embolism, and a documented injury from a
"shiatsutype massaging machine".
Shiatsu evolved from anma, a
Japanese style of massage developed in 1320 by Akashi Kan Ichi. Anma was
popularised in the seventeenth century by acupuncturist Sugiyama Waichi, and
around the same time the first books on the subject, including Fujibayashi
Ryohaku's Anma Tebiki ("Manual of Anma"), appeared.
�
Introduction page, Anma Tebiki
The Fujibayashi school carried
anma into the modern age. Prior to the emergence of shiatsu in Japan, masseurs
were often nomadic, earning their keep in mobile massage capacities, and paying
commissions to their referrers.
Since Sugiyama's time, massage in
Japan had been strongly associated with the blind.
Sugiyama, blind himself,
established a number of medical schools for the blind which taught this
practice. During the Tokugawa period, edicts were passed which made the
practice of anma solely the preserve of the blind � sighted people were prohibited
from practicing the art. As a result, the "blind anma" has become a
popular trope in Japanese culture. This has continued into the modern era, with
a large proportion of the Japanese blind community continuing to work in the
profession.
Abdominal palpation as a Japanese
diagnostic technique was developed by Shinsai Ota in the 17th century.
During the Occupation of Japan by
the Allies after World War II, traditional medicine practices were banned
(along with other aspects of traditional Japanese culture) by General
MacArthur.
The ban prevented a large
proportion of Japan's blind community from earning a living. Many Japanese
entreated for this ban to be rescinded. Additionally, writer and advocate for
blind rights Helen Keller, on being made aware of the prohibition, interceded
with the United States government; at her urging, the ban was rescinded.
Tokujiro Namikoshi (1905�2000)
founded his shiatsu college in the 1940s and his legacy was the state
recognition of shiatsu as an independent method of treatment in Japan. He is
often credited with inventing modern shiatsu. However, the term shiatsu was
already in use in 1919, when a book called Shiatsu Ho ("finger pressure
method") was published by Tamai Tempaku.
Also prior to Namikoshi's system,
in 1925 the Shiatsu Therapists Association was founded, with the purpose of
distancing shiatsu from anma massage.
Namikoshi's school taught shiatsu
within a framework of western medical science. A student and teacher of Namikoshi's
school, Shizuto Masunaga, brought shiatsu back to traditional eastern medicine
and philosophic framework. Masunaga grew up in a family of shiatsu
practitioners, with his mother having studied with Tamai Tempaku. He founded
Zen Shiatsu and the Iokai Shiatsu Center school. Another student of Namikoshi,
Hiroshi Nozaki founded the Hiron Shiatsu, a holistic technique of shiatsu that
uses intuitive techniques and a spiritual approach to healing which identifies
ways how to take responsibility for a healthy and happy life in the
practitioner's own hands. It is practiced mainly in Switzerland, France and
Italy, where its founder opened several schools.
(back
to content)
1.2.4 Traditional
Tibetan medicine w
Traditional Tibetan medicine
(Tibetan: བོད་ཀྱི་གསོ་བ་རིག་པ་,
Wylie: bod kyi gso ba rig pa), also known as Sowa-Rigpa medicine, is a
centuries-old traditional medical system that employs a complex approach to
diagnosis, incorporating techniques such as pulse analysis and urinalysis, and
utilizes behavior and dietary modification, medicines composed of natural
materials (e.g., herbs and minerals) and physical therapies (e.g. Tibetan
acupuncture, moxabustion, etc.) to treat illness.
The Tibetan medical system is
based upon Indian Buddhist literature (for example Abhidharma and Vajrayana
tantras) and Ayurveda. It continues to be practiced in Tibet, India, Nepal,
Bhutan, Ladakh, Siberia, China and Mongolia, as well as more recently in parts
of Europe and North America. It embraces the traditional Buddhist belief that
all illness ultimately results from the three poisons: delusion, greed and
aversion. Tibetan medicine follows the Buddha's Four Noble Truths which apply
medical diagnostic logic to suffering.
History
As Indian culture flooded Tibet
in the eleventh and twelfth centuries, a number of Indian medical texts were
also transmitted. For example, the Ayurvedic Astāngahrdayasamhitā
(Heart of Medicine Compendium attributed to Vagbhata) was translated into
Tibetan by རིན་ཆེན་བཟང་པོ།
(Rinchen Zangpo) (957�1055). Tibet also absorbed the early Indian Abhidharma
literature, for example the fifth-century Abhidharmakosasabhasyam by
Vasubandhu, which expounds upon medical topics, such as fetal development. A
wide range of Indian Vajrayana tantras, containing practices based on medical
anatomy, were subsequently absorbed into Tibet.
Some scholars believe that rgyud
bzhi (the Four Tantras) was told by the Buddha, while some believe it is the
primary work of གཡུ་ཐོག་ཡོན་ཏན་མགོན་པོ།
(Yuthok Yontan Gonpo, 708 AD). The former opinion is often refuted by saying
"If it was told by the Lord Buddha, rgyud bzhi should have a Sanskrit
version". However, there is no such version and also no Indian
practitioners who have received unbroken lineage of rgyud bzhi. Thus, the later
thought should be scholarly considered authentic and practical. The provenance
is uncertain.
It was the aboriginal Tibetan
people's accumulative knowledge of their local plants and their various usages
for benefiting people's health that were collected by སྟོན་པོ་གཤེན་རབ་མི་བོ་ཆེ།
the Tonpa Shenrab Miwoche and passed down to one of his sons. Later Yuthok
Yontan Gonpo perfected it and there was no author for the books, because at the
time it was politically incorrect to mention anything related to Bon nor faith
in it.
གཡུ་ཐོག་ཡོན་ཏན་མགོན་པོ།
(Yuthok Yontan Gonpo) adapted and synthesized the Four Tantras in the 12th
Century. The Four Tantras are scholarly debated as having Indian origins or, as
Remedy Master Buddha Bhaisajyaguru's word or, as authentically Tibetan. It was
not formally taught in schools at first but, intertwined with Tibetan Buddhism.
Around the turn of the 14th century, the Drangti family of physicians
established a curriculum for the Four Tantras (and the supplementary literature
from the Yutok school) at ས་སྐྱ་དགོན།
(Sakya Monastery). The ཏཱ་ལའི་བླ་
མ་སྐུ་ཕྲེང་ལྔ་བ།
(5th Dalai Lama) supported སྡེ་སྲིད་སངས་རྒྱས་རྒྱ་མཚོ།
(Desi Sangye Gyatso) to found the pioneering Chagpori College of Medicine in
1696. Chagpori taught Gyamtso's Blue Beryl as well as the Four Tantras in a
model that spread throughout Tibet along with the oral tradition.
The Four Tantras (Gyuzhi, རྒྱུད་བཞི།)
is a native Tibetan text incorporating Indian, Chinese and Greco-Arab medical
systems. The Four Tantras is believed to have been created in the twelfth
century and still today is considered the basis of Tibetan medical practise.
The Four Tantras is the common name for the text of the Secret Tantra
Instruction on the Eight Branches, the Immortality Elixir essence. It considers
a single medical doctrine from four perspectives. Sage Vidyajnana expounded
their manifestation. The basis of the Four Tantras is to keep the three bodily
humors in balance; (wind rlung, bile mkhris pa, phlegm bad kan.)
Four Tantras
Root Tantra � A general outline
of the principles of Tibetan medicine, it discusses the humors in the body and
their imbalances and their link to illness. The Four Tantra uses visual
observation to diagnose predominantly the analysis of the pulse, tongue and analysis
of the urine (in modern terms known as urinalysis)
Exegetical Tantra � This section
discusses in greater detail the theory behind the Four Tantras and gives
general theory on subjects such as anatomy, physiology, psychopathology,
embryology and treatment.
Instructional Tantra � The
longest of the Tantras is mainly a practical application of treatment, it
explains in detail illnesses and which humoral imbalance which causes the
illness. This section also describes their specific treatments.
Subsequent Tantra � Diagnosis and
therapies, including the preparation of Tibetan medicine and cleansing of the
body internally and externally with the use of techniques such as moxibustion,
massage and minor surgeries.
Some believe the Four Tantra to
be the authentic teachings of the Buddha 'Master of remedies' which was
translated from Sanskrit, others believe it to be solely Tibetan in creation by
Yuthog the Elder or Yuthog the Younger. Noting these two theories there remain
others sceptical as to its original author.
Believers in the Buddhist origin
of the Four Tantras and how it came to be in Tibet believe it was first taught
in India by the Buddha when he manifested as the 'Master of Remedies'. The Four
Tantra was then in the eighth century translated and offered to Padmasambhava
by Vairocana and concealed in Samye monastery. In the second half of the
eleventh century it was rediscovered and in the following century it was in the
hands of Yuthog the Younger who completed the Four Tantras and included
elements of Tibetan medicine, which would explain why there is Indian elements
to the Four Tantras.
Although there is clear written
instruction in the Four Tantra, the oral transmission of medical knowledge
still remained a strong element in Tibetan Medicine, for example oral
instruction may have been needed to know how to perform a moxibustion
technique.
Like other systems of traditional
Asian medicine, and in contrast to biomedicine, Tibetan medicine first puts
forth a specific definition of health in its theoretical texts. To have good
health, Tibetan medical theory states that it is necessary to maintain balance
in the body's three Three principles of function principles of function [often
translated as humors]: rLung (pron. Loong), mKhris-pa (pron. Treepa) [often
translated as bile], and Bad-kan (pron. Pay-gen) [often translated as phlegm].
� rLung is the source of the
body's ability to circulate physical substances (e.g. blood), energy (e.g.
nervous system impulses), and the non-physical (e.g. thoughts). In embryological
development, the mind's expression of materialism is manifested as the system
of rLung. There are five distinct subcategories of rLung each with specific
locations and functions: Srog-'Dzin rL�ng, Gyen-rGyu rLung, Khyab-Byed rL�ng,
Me-mNyam rLung, Thur-Sel rL�ng.
� mKhris-pa is characterized by
the quantitative and qualitative characteristics of heat, and is the source of
many functions such as thermoregulation, metabolism, liver function and
discriminating intellect. In embryological development, the mind's expression
of aggression is manifested as the system of mKhris-pa. There are five distinct
subcategories of mKhris-pa each with specific locations and functions: 'Ju-Byed
mKhris-pa, sGrub-Byed mKhris-pa, mDangs-sGyur mKhris-pa, mThong-Byed mKhris-pa,
mDog-Sel mKhris-pa.
� Bad-kan is characterized by the
quantitative and qualitative characteristics of cold, and is the source of many
functions such as aspects of digestion, the maintenance of our physical
structure, joint health and mental stability. In embryological development, the
mind's expression of ignorance is manifested as the system of Bad-kan. There
are five distinct subcategories of Bad-kan each with specific locations and
functions: rTen-Byed Bad-kan, Myag-byed Bad-kan, Myong-Byed Bad-kan, Tsim-Byed
Bad-kan, 'Byor-Byed Bad-kan.
Usage
�
Center for Oriental Medicine. Ulan-Ude, Buryatia, Russia
A key objective of the government
of Tibet is to promote traditional Tibetan medicine among the other ethnic
groups in China. Once an esoteric monastic secret, the Tibet University of
Traditional Tibetan Medicine and the Qinghai University Medical School now
offer courses in the practice. In addition, Tibetologists from Tibet have
traveled to European countries such as Spain to lecture on the topic.
The Tibetan government-in-exile
has also kept up the practise of Tibetan Medicine in India since 1961 when it
re-established the Men-Tsee-Khang (the Tibetan Medical and Astrological
Institute). It now has 48 branch clinics in India and Nepal.
The Government of India has
approved the establishment of the National Institute for Sowa-Rigpa (NISR) in
Leh to provide opportunities for research and development of Sowa-Rigpa.
(back
to content)
1.2.5 Traditional
Korean medicine w
Traditional Korean medicine
(known in North Korea as Koryo medicine) refers to the forms of traditional
medicine practiced in Korea.
�
A Korean acupuncturist inserting
a needle into the leg of a male patient. Wellcome Collection
Korean medicine traditions originated
in ancient and prehistoric times and can be traced back as far as 3000 B.C.
when stone and bone needles were found in North Hamgyong Province, in
present-day North Korea. Korean medicine originated from China. In Gojoseon,
where the founding myth of Korea is recorded, there is a story of a tiger and a
bear who wanted to reincarnate in human form and who ate wormwood and garlic.
In Jewang Ungi (제왕운기), which was written
around the time of Samguk Yusa, wormwood and garlic are described as 'edible
medicine', showing that, even in times when incantatory medicine was the
mainstream, medicinal herbs were given as curatives in Korea. Medicinal herbs
at this time were used as remedial treatment such as easing the pain or tending
injury, along with knowing what foods were good for health.
In the period of the Three
Kingdoms, traditional Korean medicine was mainly influenced by other
traditional medicines such as ancient Chinese medicine. In the Goryeo dynasty,
a more intense investigation of domestic herbs took place: The result was the
publication of numerous books on domestic herbs. Medical theories at this time
were based on the medicine of Song dynasty, but prescriptions were based on the
medicine of the Unified Silla period such as the medical text First Aid
Prescriptions Using Native Ingredients or Hyangyak Gugeupbang (향약구급방),
which was published in 1236. Other medical journals were published during this
period like Introductory
Guide to Medicine for the General
Public or Jejungiphyobang (제중입효방).
Medicine flourished in the period
of the Joseon. For example, the first training system of nurses was instituted
under King Taejong (1400�1418), while under the reign of King Sejong the Great
(1418�1450) measures were adopted to promote the development of a variety of Korean
medicinal ingredients. These efforts were systematized and published in the
Hyangyak Jipseongbang (향약집성방,
1433), which was completed and included 703 Korean native medicines, providing
an impetus to break away from dependence on Chinese medicine. The medical
encyclopaedia named Classified Collection of Medical Prescriptions (醫方類聚,
의방유취),
which included many classics from traditional chinese medicine, written by Kim
Ye-mong (金禮 蒙, 김예몽)
and other Korean official doctors from 1443 to 1445, was regarded as one of the
greatest medical texts of the 15th century. It included more than 50,000
prescriptions and incorporated 153 different Korean and Chinese texts, including
the Concise Prescriptions of Royal Doctors (御醫撮要方,
어의촬요방)
which was written by Choi Chong-jun (崔宗峻, 최종준)
in 1226. Classified Collection of Medical Prescriptions has very important
research value, because it keeps the contents of many ancient Korean and
Chinese medical books that had been lost for a long time.
After this, many books on medical
specialties were published. There are three physicians from the Joseon Dynasty
(1392�1910) who are generally credited with further development of traditional
Korean medicine�Heo Jun, Saam, and Lee Je-ma. After the Japanese invasion in
1592, Dongeui Bogam (동의보감)
was written by Heo Jun, the first of the major physicians. This work further
integrated the Korean and Chinese medicine of its time and was influential to
Chinese, Japanese and Vietnamese medicine.
The next major influence to
traditional Korean medicine is related to Sasang typology (사상의학).
Lee Je-ma and his book, The
Principal of Life Preservation in Oriental Medicine (東醫壽世保元,
동의수세보원)
systematically theorized with the influence of Korean Confucianism and his
clinical experiences in Korea. Lee Je-ma said that even if patients suffer the
same illness, patients need to use different herbal applications to treat the
same illness due to the pathophysiologies of individuals. He stresses that the
health of human body had a close relationship with the state of mind. He
believed that the human mind and body were not separate and they closely
reflected each other, and the aspect of mind needed to be considered when
examining the causes of disease. Thus, not only food and natural environment
but also emotional changes in humans can be another major reason for illness.
He believed that medical diagnosis and treatment should be based on person's
typology rather than on symptoms alone and each person should be given
different prescriptions depending on the constitution of the individual. Sasang
typology (사상의학) focuses on the
individual patients based on different reactions to disease and herbs. Treat
illness by the treatment of the root cause through proper diagnosis. Key to
this diagnosis is to first determine the internal organs or pathophysiology of
each patient.
Dongui Bogam, National Museum of
Korea
The next recognized individual is
Saam, a priest-physician who is believed to have lived during the 16th century.
Although there is much unknown about Saam, including his real name and date of
birth, it is recorded that he studied under the famous monk Samyang. He
developed a system of acupuncture that employs the five element theory.
In the late Joseon dynasty,
positivism was widespread. Clinical evidence was used more commonly as the
basis for studying disease and developing cures. Scholars who had turned away
from politics devoted themselves to treating diseases and, in consequence, new
schools of traditional medicine were established. Simple books on medicine for
the common people were published.
Lee Je-ma classified human beings
into four main types, based on the emotion that dominated their personality and
developed treatments for each type:
Tae-Yang (태양,
太陽)
or "greater yang"
So-Yang (소양,
小陽)
or "lesser yang"
Tae-Eum (태음,
太陰)
or "greater yin"
So-Eum (소음,
小陰)
or "lesser yin"
A study focused on the
examination of traditional Korean medicine during the Covid pandemic has
concluded that "traditional Korean medicine homecare services could
function as a viable alternative for continued medical care disrupted during
the coronavirus disease 19 pandemic."
Methods
Herbal medicine
�
hanyak (traditional medicine)
Herbalism is the study and
practice of using plant material for the purpose of food, medicine, or health.
They may be flowers, plants, shrubs, trees, moss, lichen, fern, algae, seaweed
or fungus.
The plant may be used in its
entirety or with only specific parts. In each culture or medical system there
are different types of herbal practitioners: professional and lay herbalists,
plant gatherers, and medicine makers.
Herbal medicines may be presented
in many forms including fresh, dried, whole, or chopped.
Herbs may be prepared as
infusions when an herb is soaked in a liquid or decocted�simmered in water over
low heat for a certain period. Some examples of infusion are chamomile or
peppermint, using flowers, leaves and powdered herbs. Decocting examples may be
rose hips, cinnamon bark, and licorice root consisting of fruits, seeds, barks,
and roots. Fresh and dried herbs can be tinctured where herbs are kept in
alcohol or contained in a vinegar extract. They can be preserved as syrups such
as glycerites in vegetable glycerin or put in honey known as miels. Powdered
and freeze dried herbs can be found in bulk, tablets, troches similar to a
lozenge, pastes, and capsules.
Non-oral herbal uses consist of
creams, baths, oils, ointments, gels, distilled waters, washes, poultices,
compresses, snuffs, steams, inhaled smoke and aromatics volatile oils.
Many herbalists consider the
patient's direct involvement to be critical. These methods are delivered
differently depending on the herbal traditions of each area. Nature is not
necessarily safe; special attention should be used when grading quality,
deciding a dosage, realizing possible effects, and any interactions with herbal
medications.
An example of herbal medicine is
the use of medicinal mushrooms as a food and as a tea. A notable mushroom used
in traditional Korean medicine is Phellinus linteus known as Song-gen.
Acupuncture
�
Doctor's office in folk village in premodern Korea.
Acupuncture is used to withdraw
blood or stimulate certain points on humans and animals by inserting them on
specific pressure points of the body. Traditional acupuncture involves the
belief that a "life force" (qi) circulates within the body in lines
called meridians. Scientific investigation has not found any histological or
physiological evidence for traditional Chinese concepts such as qi, meridians, and
acupuncture points, and many modern practitioners no longer support the
existence of life force energy (qi) flowing through meridians, which was a
major part of early belief systems. Pressure points can be stimulated through a
mixture of methods ranging from the insertion and withdrawal of very small
needles to the use of heat, known as moxibustion. Pressure points can also be
stimulated by laser, massage, and electrical means.: 234
Moxibustion
Moxibustion is a technique in
which heat is applied to the body with a stick or a cone of burning mugwort.
The tool is placed over the affected area without burning the skin. The cone or
stick can also be placed over a pressure point to stimulate and strengthen the
blood.
A Cochrane Review found limited
evidence for the use of moxibustion in correcting breech presentation of
babies, and called for more experimental trials. Moxibustion has also been studied
for the treatment of pain, cancer, stroke, ulcerative colitis, constipation,
and hypertension. Systematic reviews have found that these studies are of low
quality and positive findings could be due to publication bias.
Education
Graduate School of Korean Medicine
The South Korean government
established a national school of traditional Korean medicine to establish its
national treasure on a solid basis after the closing of the first modern
educational facility (Dong-Je medical school) one hundred years ago by the
Japanese invasion.
In 2008, the School of Korean
Medicine was established inside Pusan National University with the 50
undergraduate students on the Yangsan medical campus. The new affiliated Korean
Medical Hospital and Research Center for Clinical Studies are under
construction.
Compared with common private
traditional medicine undergraduate schools (6 years), this is a special
graduate school (4+4).
General Hospital of Koryo
Medicine
Koryo medicine is a form of traditional medicine
used in North Korea and promoted by the North Korean government, providing half
of the reported healthcare in the country. It is largely practised in the
General Hospital of Koryo Medicine, Pyongyang. Examples of Koryo medicine sold
commercially are Kumdang-2 and Royal Blood-Fresh, sold by the Pugang
Pharmaceutic Company, both of which are popular with Chinese tourists to North
Korea. ������������������������������
(back to content)
1.2.6 Indian Medicine m
Indian medicine began with the
belief that illness was caused by the Gods or by demons and was a punishment
for bad behaviour. Over time however other beliefs arose such as that which
considered good health required a balance being kept between the elements of
air, bile and mucous.
India developed surgery to a
higher standard, than any of the other ancient civilizations. This was because
the prohibition on human dissection which existed in Europe, China and the Arab
world did not exist in India. This enabled the Indian physicians to obtain a
good knowledge of human bones, muscles, blood vessels and joints. A wide
variety of surgical operations was carried out, including cosmetic surgery on
people who had been mutilated as part of a legal punishment. An adulterous wife
could have her nose cut of as a punishment and Indian surgeons learnt how to
repair the damage and replace the nose.
India is a land of many diseases
and Indian doctors were familiar with 1,120 different diseases. They guessed
the connection between malaria and mosquitoes, noticed that the plague was
foreshadowed by the death of large numbers of rats and that flies could infect
food causing intestinal disease. They were also aware that cleanliness could
help in the prevention of disease.
1.2.6.1 Indian Systems of Medicine: A Brief
Profile o
Abstract
Medicinal plants based
traditional systems of medicines are playing important role in providing health
care to large section of population, especially in developing countries.
Interest in them and utilization of herbal products produced based on them is
increasing in developed countries also. To obtain optimum benefit and to
understand the way these systems function, it is necessary to have minimum
basic level information on their different aspects. Indian Systems of Medicine
are among the well known global traditional systems of medicine. In this
review, an attempt has been made to provide general information pertaining to
different aspects of these systems. This is being done to enable the readers to
appreciate the importance of the conceptual basis of these system in evolving
the material medica. The aspects covered include information about historical
background, conceptual basis, different disciplines studied in the systems,
Research and Development aspects, Drug manufacturing aspects and impact of
globalization on Ayurveda. In addition, basic information on Siddha and Unani
systems has also been provided.
Key words: Indian System of
Medicine, Ayurveda, Unani, Siddha, Indigenous systems of medicine, Traditional
systems of medicine
Introduction
It is a well-known fact that
Traditional Systems of medicines always played important role in meeting the
global health care needs. They are continuing to do so at present and shall
play major role in future also. The system of medicines which are considered to
be Indian in origin or the systems of medicine, which have come to India from
outside and got assimilated in to Indian culture are known as Indian Systems of
Medicine (Prasad, 2002). India has the unique distinction of having six
recognized systems of medicine in this category. They are- Ayurveda, Siddha,
Unani and Yoga, Naturopathy and Homoeopathy. Though Homoeopathy came to India
in 18th Century, it completely assimilated in to the Indian culture and got
enriched like any other traditional system hence it is considered as part of
Indian Systems of Medicine (Prasad, 2002). Apart from these systems- there are
large number of healers in the folklore stream who have not been organized
under any category. In the present review, attempt would be made to provide
brief profile of three systems to familiarize the readers about them so as to
facilitate acquisition of further information.
Ayurveda
Most of the traditional systems
of India including Ayurveda have their roots in folk medicine. However, what
distinguishes Ayurveda from other systems is that it has a well-defined
conceptual framework that is consistent throughout the ages. In conceptual
base, it was perhaps highly evolved and far ahead of its time. It was among the
first medical systems to advocate an integrated approach towards matters of
health and disease. Another important distinguishing feature of Ayurveda is
that unlike other medical systems, which developed their conceptual framework
based on the results obtained with the use of drugs and therapy, it first
provided philosophical framework that determined the therapeutic practice with
good effects. Its philosophical base is partly derived from �Samkhya� and
�Nyaya vaisheshika� streams of Indian philosophy. This enabled it to evolve
into rational system of medicine quite early in its evolution and to get
detached from religious influence. It laid great emphasis on the value of
evidence of senses and human reasoning (Ramachandra Rao, 1987).
Historical background
Ayurveda literally means the
Science of life. It is presumed that the fundamental and applied principles of
Ayurveda got organized and enunciated around 1500 BC. Atharvaveda, the last of
the four great bodies of knowledge- known as Vedas, which forms the backbone of
Indian civilization, contains 114 hymns related to formulations for the
treatment of different diseases. From the knowledge gathered and nurtured over
centuries two major schools and eight specializations got evolved. One was the
school of physicians called as �Dhanvantri Sampradaya� (Sampradaya means
tradition) and the second school of surgeons referred in literature as �Atreya
Sampradaya�. These schools had their respective representative compilations-
Charaka Samhita for the school of Medicine and Sushruta Samhita for the school
of Surgery. The former contains several chapters dealing with different aspects
of medicine and related subjects. Around six hundred drugs of plant, animal and
mineral origin have been mentioned in this treatise.
Sushruta Samhita primarily deals
with different aspects of fundamental principles and theory of surgery. More
than 100 kinds of surgical instruments including scalpels, scissors, forceps,
specula etc. are described along with their use in this document. Dissection
and operative procedures are explained making use of vegetables and dead
animals. It contains description of about 650 drugs and discusses different
aspects related to other surgery related topics such as anatomy, embryology,
toxicology and therapeutics (http://www.indianmedicine.nac.in). Vagabhata�s
�Astanga-Hridaya� is considered as another major treatise of Ayurveda. The
above three documents are popularly known as �Brihat trayees� (the big or major
three). In addition to these three scholarly and authoritative treatises a vast
body of literature exist in the form of compilations covering a period of more
than 1500 years (http://www.indianmedicine.nac.in).
Till the medieval period it was
perhaps the only system available in the Indian sub-continent at that time to
cater to the healthcare requirement of the people. It enjoyed the unquestioned
patronage and support of the people and their rulers. This can be considered as
the golden period of Ayurveda because most of the work related to basic
concepts, enunciation of different principles, evolvement of different
formulations occurred during this period. The patronage for the Ayurvedic
system of medicine considerably decreased during the medieval period, which was
marked by unsettled political conditions in the country and series of invasion
by foreigners. The neglect became worse during British rule during which
importance was given to Allopathy through official patronage. In the early part
of 20th century interest in Ayurveda rekindled as part of national freedom
movement. People�s representatives even in British India and princely states
started asking for suitable measures to develop Ayurveda on scientific lines
(http://www.indianmedicine.nac.in).
After India gained Independence
from the British rule in 1947, the movement for revival of Traditional Systems
of Medicine gained momentum. The systems got official recognition and became
part of the National Health care network to provide health care to the
country�s citizen. Government of India initiated a series of measures to
improve the position of Ayurveda as one of the major health care systems vital
for catering to the primary health care needs of the country. A number of
hospitals and colleges for Ayurveda were established. The other major
initiatives were establishment of a research Institute to take care of the R
& D needs (Central Institute of Research in Indigenous System of Medicine
(CIRISM)- in 1955); a Post Graduate Training Centre of Ayurveda in 1956- to impart
Post graduate education; establishment of a University- named Gujarat Ayurved
University at Jamnagar in the Gujarat State in 1967; creation of Central
Council of Indian Medicine (CCIM) in 1972 for regulating Education and
Registration in Ayurveda, Siddha and Unani systems of medicine. A research
council named Central Council for Research in Indian Medicine, Homoeopathy and
Yoga (CCRIMH) was established in 1971. Subsequently, this council was
bifurcated to create three separate councils -Central Council for Research in
Ayurveda & Siddha (CCRAS), Central Council for Research in Unani Medicine
(CCRUM), Central Council for Research in Homoeopathy (CCRH) and Central Council
for Research in Naturopathy and Yoga (CCRNY) . National Institute of Ayurveda
(NIA) was established at Jaipur in Rajasthan state. Recently another University
has been established known as Rajasthan Ayurved University- Jodhpur (Rajasthan
state). A draft national policy for the development of Indian System of
Medicine has been prepared which is available on the web site of Department of
Ayurveda - (http://www.indianmedicine.nac.in).
THE CONCEPT OF HEALTH IN AYURVEDA
In India, Ayurveda is considered
not just as an ethnomedicine but also as a complete medical system that takes
in to consideration physical, psychological, philosophical, ethical and
spiritual well being of mankind. It lays great importance on living in harmony
with the Universe and harmony of nature and science. This universal and
holistic approach makes it a unique and distinct medical system. This system
emphasizes the importance of maintenance of proper life style for keeping
positive health. This concept was in practice since two millennia and the
practitioners of modern medicine have now taken into consideration importance
of this aspect. Not surprisingly the WHO�s concept of health propounded in the
modern era is in close approximation with the concept of health defined in
Ayurveda (Kurup, 2004).
THE PHILOSOPHICAL BACKGROUND
The basic foundation is the
fundamental doctrine according to which whatever present in the Universe
(macrocosm) should be present in the body (the microcosm). It has been
conceptualized that the universe is composed of five basic elements named
Prithvi (Earth), Jala (Water), Teja (Fire), Vayu (Air) and Akash (Space/Ether).
The human body is derived from them in which these basic elements join together
to form what are known as �Tridoshas� (humors) named as Vata, Pitta and Kapha.
These humors govern and control the basic psycho-biological functions in the
body. In addition to these three humors, there exist seven basic tissues
(saptha dhatus)- Rasa, Rakta, Mamsa, Meda, Asthi, Majja and Shukra- and three
waste products of the body (mala) such as faeces, urine and sweat. Healthy
condition of the body represents the state of optimum equilibrium among the
three doshas. Whenever this equilibrium is disturbed due to any reason- disease
condition results. The growth and development of the body components depend on
nutrition provided in the form of food. The food is conceptualized to be
composed of the basic five elements mentioned above. Hence it is considered to
be the basic source material to replenish or nourish the different components
of the body after the action of bio-fire (Agni).
The tissues of the body are
considered as the structural entities and the humours are considered as
physiological entities, derived from different combinations and permutations of
the five basic elements (http://www.indianmedicine.nac.in).
THE CONCEPT OF PATHOGENESIS
People are categorized in to
different categories based on their psychosomatic constitution. Constitution
specific daily (Dinacharya) and seasonal routines (Ritucharya) are prescribed
to maintain positive health. Body may become afflicted with disease if these
routines are not adhered to. This will lead to the loss of equilibrium among
the three humors. The loss of equilibrium of the three humors can also occur as
a consequence of dietary indiscrimination, undesirable habits, seasonal
abnormalities, improper exercise or erratic application of sense organs and
incompatible actions of the body and mind.
Disease condition may ensue due
to other reasons also. For example, any external factor like microorganism,
changes in the climatic conditions may cause the accumulation of dosha leading
to disturbance in the doshic equilibrium and vitiation of doshas. It is
conceptualized that normally doshas are circulated through macro and
micro-channels known as srotas. The srotas are the important medium through
which the body tissues get their nutrition and also the metabolic end products
are transported out of the tissue. If any blockade occurs (srotorodha) due to
accumulation of doshas, the bi-directional flow of nutrients and end products
(malas) gets affected. The doshas accumulated in the region react with the
dushyas (reactants- in this case tissues) resulting in a condition known as
dosha dushya sammurchana- this affects body metabolism. Ama, which is a
semi-processed intermediary product of metabolism, gets accumulated. At this
stage the prodromal symptoms of the disease gets manifested. Thus disturbances
in the bio-channels are considered to be the main reason for the expression of
diseased state of an organ or system.
DIAGNOSIS
The diagnosis is always done by
considering the patient as a whole object to be examined. The physician takes a
careful note of the patient�s internal physiological characteristics and mental
disposition. He also studies other factors like- the affected bodily tissues,
humors, the site at which the disease is located, patient�s resistance and
vitality, his daily routine, dietary habits, the gravity of clinical
conditions, condition of digestion and details of personal, social, economic
and environmental situation of the patient. The general examination is known as
ten-fold examination- through which a physician examines the following
parameters in the patient- 1. Psychosomatic constitution, 2. Disease
susceptibility, 3. Quality of tissues, 4. Body build, 5. Anthropometry, 6.
Adaptability, 7. Mental health, 8. Digestive power, 9. Exercise endurance and
10. Age. In addition to this, examination of pulse, urine, stool, tongue, voice
and speech, skin, eyes and overall appearance is also carried out (Kurup,
2002).
TREATMENT ASPECTS
The treatment lies in restoring
the balance of disturbed humors (doshas) through regulating diet, correcting
life-routine and behavior, administration of drugs and resorting to preventive
non-drug therapies known as �Panchkarma� (Five process) and �Rasayana�
(rejuvenation) therapy. Before initiating treatment many factors like the
status of tissue and end products, environment, vitality, time, digestion and
metabolic power, body constitution, age, psyche, body compatibility, type of
food consumed are taken in to consideration.
TYPES OF TREATMENT
The treatments are of different
types- a- Shodhana therapy (purification treatment), b-Shamana therapy
(palliative treatment), Pathya Vyavastha (prescription of appropriate diet and
activity), Nidan Parivarjan (avoidance of causes and situations leading to
disease or disease aggravation), Satvajaya (psychotherapy) and Rasayan
(adaptogens- including immunomodulators, anti-stress and rejuvenation drugs)
therapy. Dipan (digestion) and Pachan (assimilation) enhancing drugs are
considered good for pacifying the vitiated doshas (humors).
This therapy is supposed to
dissolve the vitiated and accumulated doshas by improving the agni (digestive
power) and restoring the deranged metabolic process. In severe conditions the
above therapy has to be supplemented with purificatory processes like
Panchakarma. In this therapy initially the accumulated vitiated dosha is
liquefied by resorting to external and internal oleation of the patient;
followed by sudation (swedhana) and elimination of vitiated dosha through
emesis (Vamana) or purgation (Virechana), Basti (enema- evacuating type) and
Nasya (nasal insufflation).
Shodhana therapy provides
purificatory effect through which therapeutic benefits can be derived. This type
of treatment is considered useful in neurological and musculo-skeletal
disorders, certain vascular or neuro-vascular states, respiratory diseases, and
metabolic and degenerative disorders. Shamana therapy involves restoring
normalcy in the vitiated doshas (humors). This is achieved without causing
imbalance in other doshas. In this use of appetizers, digestives, exercise and
exposure to sun and fresh air are employed. In the Pathya Vyavastha type of
treatment certain indications and contraindications are suggested with respect
to diet, activity, habits and emotional status. In Nidan Parivarjan type of
treatment the emphasis is on avoiding known causes of the disease by the
patient. In Satvavajaya type of treatment the emphasis is on restraining the
mind from the desires for unwholesome objects and Rasayana therapy deals with
the promotion of strength and vitality (http://www.indianmedicine.nac.in).
DIETICS IN AYURVEDA
Ayurveda lays great emphasis on
the diet regulation. According to Ayurvedic concepts food has great influence
over physical, temperamental and mental development of an individual. The food
is the basic material for the production of the body and life supporting vital
matter known as Rasa. The rasa is converted to body components and supports all
types of life activities.
DIFFERENT DISCIPLINES OF AYURVEDA
Ayurveda is known as Astanga
Ayurveda- means that which is made up of eight parts. The eight major divisions
of Ayurveda are as follow as:
1. Kayachikitsa (Internal
Medicine) 2. Kaumar Bhritya (Pediatrics) 3. Bhootavidya (Psychiatry) 4.
Shalakya (Otorhinolaryngology and Ophthalmology) 5. Shalya (Surgery) 6. Agada
Tantra (toxicology) 7. Rasayana (Geriatrics) and 8. Vajikarana (Aprhodisiacs
and Eugenics)
Present status of Ayurveda and other Indigenous
Systems of Medicine in India
Regulation of the practice of ISM
& H
Eighteen major states have
independent Directorate to look after ISM related issues. In six states the ISM
is administrated under the Health Directorate of the State, in around six smaller
states and Union Territories Officer in�charges look after the issues concerned
with ISM. At present there are more than 6.11 lakh practioners of ISM & H.
The number of Hospitals and dispensaries in this sector is more than 26,000
where free treatment facility is available. In addition large number of
practioners in the un-organized folklore sector provide remedies to
considerable portion of the population (http://www.indianmedicine.nac.in )
EDUCATION
At present there are more than
200 colleges, which offer a four and half year course leading to Bachelor
Degree in Ayurvedic Medicine and Surgery, followed by one year internship.
Similarly 2 colleges offer graduate degree in Siddha System of Medicine and 34
colleges offer degree in Unani System of Medicine and 130 colleges offer
courses leading to degree in Homoeopathy. The turnover of candidates from these
colleges exceeds 9,000 per year. More than 30 Institutes offer postgraduate
courses for Ayurveda and specialization is available in 16 disciplines. In addition
there is National Academy of Ayurveda, which imparts PG education under the
scheme of �Guru Shishya parampara�. This scheme has been created with a view to
provide education on traditional lines like what used to be in ancient times.
In ancient times students used to visit the abode of the teacher to serve him
while learning the art of healing from him. At present around 750 Post graduate
scholars are turned out every year (the duration of course is 3 years). The
degree offered is M.D. (Ayu) and M.S. (Ayu). Recently Pharmacy colleges have
been opened which offer D.Pharm (Ayu), B.Pharm (Ayu) and M.Pharm (Ayu) (for
further details visit-http://www.ayurveduniversity.com). Training programmes
mainly, in-house are conducted, through out the country to train para-ayruvedic
staff. These trained technicians help in carrying out therapeutic process like
panchakarma and ksarasutra (an effective surgical procedure for removing
hemorrhoids). Similarly pharmacists are trained to shoulder responsibilities of
running an ayurvedic pharmacy.
RESEARCH AND DEVELOPMENT
The research activities are being
carried out by Central Council for Research in Ayurveda & Siddha (CCRAS)
and similar councils for Unani, Homoeopathy and Naturopathy & Yoga. The
CCRAS is the premier agency involved in research and development
(http://www.ccras.com). It has 89 field units, which have been re-organized in
to 30 institutes and units. The types of activities undertaken are clinical
research- involving planned clinical trial of single and compound ayurvedic
preparations and drug research which includes medico-botanical surveys,
cultivation of medicinal plants, pharmacognostical studies, phytochemical
studies, drug standardization, pharmacological and toxicological studies. A
vast body of data is available in various published literature and data bases
(Sharma et al 2000, 2001, 2002; Billore et al 2004; Satyavati et al, 1976,
1987, Satyavati, 2005; Mishra, 2004; De et al 1993; Chatterjee and Pakrashi
(1995-1997); Gupta and Tandon (2004) ; Wealth of India series ( 1959-69; 1985
and 2000) ; Dahanukar et al 2000; Rastogi and Dhawan (1982); Ayurvedic
Pharmacopoeia Part- I in three volumes (Anonymous-1989, 1999 and 2000) ;
Sivarajan and Balachandran (1999); Raghunathan and Mitra (1982) and five
volumes (1-5) by Rastogi and Mehrotra (1990, 1991, 1993 ,1995 and 1998).
Literary research, which involves publication of rare and classical manuscripts
of ISM & H., is also carried out (http://www.ccras.com).
Besides research councils
research activities are carried out in Post Graduate centers and Institutes of
national importance like- Central Drug Research Institute (CDRI), Central
Institute of Medicinal and Aromatic Plants (CIMAP), National Botanical Research
Institutes (NBRI) etc and R & D centers attached to Ayurvedic drug
manufacturing firms (Kurup- 2004). However the main tendency is to consider
medicinal plants used in Ayurveda as source material for bio-prospecting of
drugs. There are very few studies, which take in to consideration the ayurvedic
concept behind a given formulation. Ayurveda has a very well developed drug
formulation discipline known as �Bhaishajya Kalpana�, which provides great deal
of information about methods of drug preparation, use of adjuvants, collection
and processing drugs in a particular manner. Research efforts on this aspect
and on basic principles of Ayurveda are yet to be undertaken in concerted
manner.
DRUG MANUFACTURING IN AYURVEDIC SECTOR
Ayurvedic drugs are marketed in various forms. They are available in
both classical forms (tablets, powder, decoction, medicated oil, medicated
ghee, fermented products) and modern drug presentation forms like capsules,
lotions, syrups, ointments, liniments, creams, granules etc. There are more
than 8500 manufacturers of Ayurvedic drugs in the country and the gross
turnover of drugs used in all the ISM & H systems is approximately around 1
billion US dollars. Drug manufacturing in this sector is regulated by Drugs and
Cosmetic act (1940) and rules (1945) (Jain, 2001). Subsequently many chapters
have been added to these acts over the years. Three types of agencies are
involved in the administration of the Acts and Rules enacted by the parliament.
There is Drug Technical Advisory Board and Drug Consultative Committee to
advise the Govt., The Drug Controller General of India who with the help of the
supporting staff is in charge of licensing and enforcing different laws related
to drug manufacturing and dispensing. At the state level Food and Drug
Administration Commissioners shoulder this responsibility. Recently Good
Manufacturing Process for ISM has been defined which have to be followed by all
the agencies involved in the manufacturing of drugs in this sector
(http://www.indianmedicine.nac.in ).
GLOBALIZATION OF AYURVEDA
Globalization of Ayurvedic practice has gained momentum in the past two
decades. Ayurvedic drugs are used as food supplements in USA, European Union
and Japan. Many physicians practice Ayurveda in many parts of the world.
Facilities are available in countries like USA, Argentina, Australia, Brazil,
New Zealand, South Africa, Czech Republic, Greece, Italy, Hungary, Netherlands,
Russia, UK, Israel, Japan, Nepal, Sri Lanka (Kurup, 2004) for imparting short
and long-term training in Ayurveda.
The concepts of proper life
styles, dietary habits, daily and seasonal routines followed in Ayurveda can be
adopted with suitable modification to different countries in different parts of
the globe after giving due consideration to the cultural milieu existing in
those countries and also to the constitutional profile of their population.
Attempts can also be made to utilize the medicinal plant resources of these
countries for meeting the health care needs of their people after
categorization of the plants according to Ayurvedic concepts. Drugs used in ISM
can be used as adjuvant to the main drugs used in Allopathy. Non-drug
therapeutic approaches such as �Panchakarma�, �Ksarasutra� etc can certainly be
integrated into other health systems broadening the choices available to
physicians and patients.
A recent review (Dahanukar et
al., 2000) points out that more than 13,000 plants have been investigated
during the past 5 years. Number of medicinal plants have been shown to possess
important pharmacological activities in pre-clinical testing however the
generated leads have not been adequately followed up with double blind, placebo
controlled clinical trails. Curcuma longa Linn, Boswellia serrata Roxb. ex
Coleb., Picrorhiza kurroa Royle ex Benth, Terminalia chebula Retz., Emblica
officinalis Gaertn., Bacopa monnieri (Linn.) Pennel, Boerhavia diffusa Linn,
Phyllanthus niruri Linn, Celastrus paniculatus, Ocimum sanctum Linn, Gymnema
sylvestre R.Br., Momordica charantia Linn, Commiphora wighti (Arn.) Bhandari,
Withania somnifera (Linn.) Dunal, Pterocarpus marsupium Roxb., Tinospora
cordifolia (Willd). Miers. Ex Hook.f. & Thomson, Trichopus zeylanicum,
Terminalia arjuna (Roxb.) Wight & Arn etc have great potential to develop
in to drugs of global importance. Table-1 provides list of some of the important
medicinal plants with good potential to develop at global level. This list is
not exhaustive and is based mainly on the author�s own preference. Many of the
drugs in the list are not available in sufficient quantity in India but may be
available in other countries especially Nigeria where Commiphora species are
abundant- they can be the source of supply to Indian ISM based industry. One of
the main lacunae is the lack of co-ordinated multi-disciplinary studies to
prove their clinical efficacy beyond doubt. This aspect should be the main
focus of future research endeavors.
(back
to content)
1.2.6.2 Siddha system of medicine w
Siddha system of medicine is
practiced in some parts of South India especially in the state of Tamilnadu. It
has close affinity to Ayurveda yet it maintains a distinctive identity of its
own. This system has come to be closely identified with Tamil civilization. The
term 'Siddha' has come from 'Siddhi'- which means achievement. Siddhars were
the men who achieved supreme knowledge in the filed of medicine, yoga or tapa
(meditation) (Narayanaswamy, 1975).
It is a well-known fact that
before the advent of the Aryans in India a well-developed civilization
flourished in South India especially on the banks of rivers Cauvery, Vaigai,
Tamiraparani etc. The system of medicine in vogue in this civilization seems to
be the precursor of the present day Siddha system of medicine. During the
passage of time it interacted with the other streams of medicines complementing
and enriching them and in turn getting enriched. The materia medica of Siddha
system of medicine depends to large extent on drugs of metal and mineral origin
in contrast to Ayurveda of earlier period, which was mainly dependent upon
drugs of vegetable origin.
According to the tradition
eighteen Siddhars were supposed to have contributed to the development of
Siddha medicine, yoga and philosophy. However, literature generated by them is
not available in entirety. In accordance with the well-known self-effacing nature
of ancient Indian Acharyas (preceptors) authorship of many literary work of
great merit remains to be determined. There was also a tradition of ascribing
the authorship of one�s work to his teacher, patron even to a great scholar of
the time. This has made it extremely difficult to clearly identify the real
author of many classics.
PHILOSOPHICAL FOUNDATION
According to the Siddha concepts
matter and energy are the two dominant entities, which have great influence in
shaping the nature of the Universe. They are called Siva and Sakthi in Siddha
system. Matter cannot exist without energy and vice-versa. Thus both are
inseparable. The universe is made up of five proto-elements. The concept of
five proto-elements and three doshas in this system of medicine is quite
similar to Ayurvedic concept pertaining to them. However, there are certain
differences in the interpretation (Narayanaswamy, 1975). The concepts behind
diagnostic measures also show great similarities differing in certain aspects
only. Diagnosis in Siddha system is carried out by the well �known �ashtasthana
pareeksha� (examination of eight sites) that encompasses examination of nadi
(pulse), kan (eyes), swara (voice), sparisam (touch), varna (colour), na
(tongue), mala (faeces) and neer (urine). These examination procedures are
provided in greater detail in classical Siddha literature in comparison to
classical literature of Ayurveda (Narayanaswamy, 1975).
PRINCIPLES OF TREATMENT
Similar to Ayurveda, Siddha
system also follows ashtanga concept with regards to treatment procedures.
However the main emphasis is on the three branches - Bala vahatam (pediatrics),
Nanjunool (toxicology) and Nayana vidhi (ophthalmology). The other branches
have not developed to the extent seen in Ayurveda. The surgical procedures,
which have been explained in great detail in Ayurvedic classics, do not find
mention in Siddha classics. The therapeutics in both the systems can be broadly
categorized into samana and sodhana therapies. The latter consists of
well-known procedures categorized under panchakarma therapy. This therapy is
not that well developed in Siddha system, only the vamana therapy has received
attention of the Siddha physicians (Narayanaswamy, 1975).
MATERIA MEDICA
The concept pertaining to drug composition, the concept of rasapanchaka
(concept explaining drug properties) is almost similar in both the systems of
medicine. One of the major characteristic features of Siddha materia medica is
utilization of mineral and metal-based preparations to greater extent in comparison
to the drugs of vegetable origin.
The mineral and metal-based drugs
in Siddha System are categorized under the following categories:
1. Uppu (Lavanam)- drugs that are dissolved in water and get
decrepitated when put into the fire giving rise to vapor.
2. Pashanam: drugs that are water insoluble but give off vapors when
put in to fire
3. Uparasam: Similar to pashanam chemically but have different actions.
4. Ratnas and uparatnas, which include drugs based on precious and
semi-precious stones
5. Loham - metals and metal alloys that do not dissolve in water but
melt when put in to fire and solidify on cooling.
6. Rasam: drugs that are soft, sublime when put in to fire changing
into small crystals or amorphous powders.
7. Gandhakam: sulphur is insoluble in water and burns off when put into
fire. From the above basic drugs compound preparations are derived. From the
animal kingdom thirty-five products have been included in the materia medica.
It is much similar to preparations used in Ayurveda. Numbers of plant-based
preparations are also used in Siddha system of medicine they are quite similar
in profile to those mentioned in Ayurveda.
(back
to content)
1.2.6.3 Unani system of medicine w
Historical background
Unani medicine has its origin in
Greece. It is believed to have been established by the great physician and
philosopher- Hippocrates (460-377 BC). Galen (130-201 AD) contributed for its
further development. Aristotle (384-322 BC) laid down foundation of Anatomy &
physiology. Dioscorides � the renowned physician of the 1st Century AD has made
significant contribution to the development of pharmacology, especially of
drugs of plant origin. The next phase of development took place in Egypt and
Persia (the present day Iran). The Egyptians had well evolved pharmacy; they
were adept in the preparation of different dosage forms like oils, powder,
ointment and alcohol etc. (http://www.indianmedicine.nac.in).
The Arabian scholars and
physicians under the patronage of Islamic rulers of many Arabian countries have
played great role in the development of this system. Many disciplines like
chemistry, pharmaceutical procedures like distillation, sublimation,
calcinations and fermentation were developed and refined by them. There are
many well-known names- only some names have been mentioned in this article.
Jabir bin Hayyan (717-813 AD) a Royal physician of his time has worked on the
chemical aspects; Ibne Raban Tabari (810-895 AD) is the author of the book-
Firdous ul Hikmat and introduced concept of official formulary. Abu Bakar
Zarakariya Razi (865-925 AD) has authored a book known as "Alhawi fit
tibb". He has worked in the field of immunology. Of course the name of Bu
Ali Sina (Avicenna 980-1037 AD) is always referred in all matters related to
Unani. He was a renowned global level scholar and philosopher. He had great
role in the development of Unani medicine in the present form. His book
Alqanoon or (The canon of medicine) was an internationally acclaimed book on
medicine, which was taught in European countries till the 17th century. Many
physician of Arab descent in Spain have also contributed to the development of
the system. Some of the important names are-Abul Qasim Zohravi (Abulcasus 946 �
1036 AD) he is the author of the famous book on surgery "Al
Tasreef"-(http://www.indianmedicine.nac.in).
The Arabs were instrumental in
introducing Unani medicine in India around 1350 AD. The first known Hakim
(Physician) was Zia Mohd Masood Rasheed Zangi. Some of the renowned physicians who
were instrumental in development of the system are- Akbar Mohd Akbar Arzani
(around 1721 AD)- the author of the books- Qarabadin Qadri and Tibbe Akbar;
Hakim M. Shareef Khan (1725-1807)- a renowned physician well-known for his book
Ilaj ul Amraz. Hakim Ajmal Khan (1864-1927) a great name among the 20th Century
Unani physicians in India. He was a multifaceted personality besides being a
physician he was a scientist, politician and a freedom fighter. He was
instrumental in the establishment of Unani and Ayurvedic College at Karol Bagh,
Delhi. He was a keen researcher and has supervised many studies on Rauwolfia
serpentina- the source plant for many well-known alkaloids like reserpine,
Ajamaloon etc. Another great contributor is Hakim kabeeruddin (1894-1976), he
has translated 88 Unani books of Arabic and Persian languages into Urdu. The
first institution of Unani medicine was established in 1872 as Oriental College
at Lahore in the undivided India. Thereafter many institutions came into
existence.
After Independence Unani received
boost in the form of Government support through various agencies involved in
the development of ISM. At present there are more than 30 colleges offering
degree course in Unani medicine and the approximate number of physician turn out
is around 20,000. There are around 177 hospitals. A National Institute of Unani
Medicine has been established at Bangalore in Karnataka state in 1983 in
collaboration with the Govt. of Karnataka- for catering to both academic and R
& D requirements. Central Council for Research in Unani Medicine (CCRUM),
is the premier agency involved in R & D activities
(http://www.indianmedicine.nac.in).
Table 1: Some well-known Indian medicinal plants and their
uses
|
Botanical name
|
Parts used
|
Therapeutic uses
|
|
Acorus calamus Linn ( Araceae)
|
Rhizome
|
Nervine tonic, anti-spasmodic (Satyavati et
al ., 1976; Bose et al., 1960)
|
|
Aegle marmelos (L.) Corr. (Rutaceae)
|
Fruit
|
Hypoglycemic; chemopreventive
(Vyas et al., 1979; Dixit et al., 2006)
|
|
Allium sativum Linn (Alliaceae)
|
Bulbs
|
Anti-inflammatory; anti-hyperlipidemic,
fibrinolytic (Dixit et al., 2006)
|
|
Aloe barbadensis Mill., and Aloe vera Tourn. Ex Linn.
(Alliaceae)
|
Gel
|
Skin diseases- mild sunburn, frostbite,
scalds; wound healing (Baliga, 2006)
|
|
Andrographis paniculata (Burm.f.) Wallich ex Nees (Acantahceae)
|
Whole plant
|
Cold; flu � hepatoprotection (Koul and
Kapil-1994; Sharma et al., 2002a)
|
|
Asparagus racemosus Willd
(Alliaceae)
|
Roots
|
Adaptogen, galactogogue (Dahanukar et al.,
1997;Gupta and Mishra, 2006)
|
|
Bacopa monnieri (L) Pennel
(Scorphulariaceae)
|
Whole plant
|
Anti-oxidant; memory enhancing (Singh and
Dhawan, 1997)
|
|
Berberis aristata DC
(Berberidaceae)
|
Bark, fruit, root, stem, wood
|
Anti-protozoal, hypoglycemic, anti-trachoma
(Dutta and Iyer, 1968; Sharma et al., 2000a)
|
|
Boerhavia diffusa L.
(Nyctaginaceae)
|
Roots
|
Diuretic; anti-inflammatory and
anti-arthritic (Sharma et al., 2000b; Harvey, 1966)
|
|
Boswellia serrata Roxb.
(Burseraceae)
|
Oleo resin
|
Anti-rheumatic; anti-colitis and
anti-inflammatory, anti-cancer. (Sharma et al., 2000c)
|
|
Butea monosperma (Lam.) Taub
(Fabaceae)
|
Bark, leaves, flowers, seeds and gum
|
Adaptogen; abortifacient, anti-oestrogenic,
anti-gout, anti-ovulatory
(Sharma et al., 2000d)
|
|
Calotropis gigantea (Linn) R. Br.
(Asclepiadaceae)
|
Flowers, whole plant, root, leaf
|
Anti-inflammatory, spasmolytic, asthma
(Sharma et al., 2000e)
|
|
Callicarpa macrophylla Vahl.
(Verbenaceae)
|
Leaves, roots
|
Uterine disorders (Sood, 1995)
|
|
Cassia fistula Linn
(Leguminosae)
|
Resin
|
Laxative, anti-pyretic, worm infestation
(Joshi, 1998)
|
|
Celastrus paniculatus Willd
(Celastraceae)
|
Whole plant
|
Brain tonic; memory enhancer; in the
treatment of depression (Tanuja Doshi, 1991; Joglekar and Balwani, 1967)
|
|
Centella asiatica (Linn) Urban
(Umbelliferae)
|
Whole plant
|
Tranquilizer; memory enhancer; wound
healing- (Sharma et al., 2000 f; Suguna et al ., 1996)
|
|
Chlorophytum boriavillianum Santapau & RR Fernandus
(Alliaceae)
|
Roots
|
Aphrodisiac (Farooqi et al., 2001)
|
|
Cissus quadrangularis L
(Vitaceae)
|
Whole plant, root, stem and leaf
|
Bone fracture; inflammation (Deka et
al., 1994) (Udupa & Prasad, 1964b)
|
|
Clerodendrum serratum (Linn) Moon (Verbenaceae)
|
Root, leaf, Stem
|
Malaria; anti-asthmatic, anti-allergic
(Gupta and Gupta, 1967) (Sivarajan and
Balachandran 1999a)
|
|
Commiphora mukul ( Hooker Stedor) Engl. (Burseraceae)
|
Resin
|
Hypolipidemic; obesity, rheumatoid arthritis
(Satyavati, 1991)
|
Basic principles
According to the basic principles
of Unani the body is made up of four basic elements i.e. Earth, Air, Water,
Fire which have different Temperaments i.e. Cold, Hot, Wet, Dry. They give
raise, through mixing and interaction, to new entities. The body is made up of
simple and complex organs. They obtain their nourishment from four humors
namely- blood, phlegm, black bile and yellow bile. These humors also have their
specific temperament. In the healthy state of the body there is equilibrium
among the humors and the body functions in normal manner as per its own
temperament and environment. Disease occurs whenever the balance of humors is
disturbed.
In this system also prime
importance is given for the preservation of health. It is conceptualized that
six essentials are required for maintenance of healthy state. They are i. Air,
ii. Food and drink, iii. Bodily movements and response, iv. Psychic movement
and repose, V. Sleep and wakefulness and vi. Evacuation and retention. Specific
requirement for each of these six essentials have been discussed- (Syed
Khaleefathullah, 2002).
The human body is considered to
be made up of seven components, which have direct bearing on the health status
of a person. They are 1. Elements (Arkan) 2. Temperament (Mijaz). 3. Humors
(Aklat) 4. Organs (Aaza) 5. Faculties (Quwa) 6. Spirits (Arwah). These
components are taken in to consideration by the physician for diagnosis and
also for deciding the line of treatment (Syed Khaleefathullah, 2002).
Diagnosis
Examination of the pulse occupies
a very important place in the disease diagnosis in Unani. In addition
examination of the urine and stool is also undertaken. The pulse is examined to
record different features like- size, strength, speed, consistency, fullness,
rate, temperature, constancy, regularity and rhythm. Different attributes of
urine are examined like odor, quantity, mature urine and urine at different age
groups. Stool is examined for color, consistency, froth and time required for
passage etc.
Treatment
Disease conditions are treated by
employing four types of therapies- a- Regimental therapy, b- Dietotherapy,
c-Pharmacotherapy and d- Surgery. Regimental therapy mainly consists of drug
less therapy like exercise, massage, turkish bath, douches etc. Dietotherapy is
based on recommendation of patient specific dietary regimen. Pharmacotherapy
involves administration of drugs to correct the cause of the disease. The drugs
employed are mainly derived from plants some are obtained from animals and some
are of mineral origin. Both single and compound preparations are used for the
treatment.
A large number of studies have
been carried out on number of medicinal plants used in ISM of medicine. Central
Drug Research Institute undertook a series of studies (Anonymous - 1991) under
drug screening programme. Number of compilation have been published providing
information about pharmacological activity profile of medicinal plants,
publications are also available on the chemical profile of number of medicinal
plants, Ayurvedic pharmacopoeia has been published � three volumes have come
out so far, CCRAS has published a series of books under its Data base
preparation project. There is an international publication on scientific
validation of Ayurvedic therapies. Besides these books large number of review
articles have been published in national and international Journals providing
names of drugs used in particular type of disease conditions or screened for
particular type of pharmacological activities.
If the situation prevailing in
this sector is analyzed taking into consideration different aspects- it becomes
clear that there is a perceptible trend towards increased usage of drugs used
in Indian Traditional Systems especially those which are based on herbal
products not only in India but in different parts of the world. However, one of
the basic problems that still remained to be solved is related to proving
efficacy of the products used in these systems on the basis of controlled
clinical trial and complementary pharmacological studies. It is difficult to
ensure consistency in the results and components in the products. This is
traced mainly to lack of standardization of the inputs used and the process
adopted for preparation of the formulations. Government of India has taken
these aspects in to consideration and has initiated many projects for
standardization of single and compound formulations along with standardization
of operating procedures for important formulations. Though standardization is
very difficult it is not an un-attainable goal. Once this is done it would help
in promoting wider use of these drugs especially in chronic degenerative
disorders. Further non-drug therapies and preventive and life management
techniques are also receiving increased attention. Thus this sector seems to be
poised for remarkable growth in the coming years (Kurup, 2004).
The above presentation can be
considered only as brief introduction to the above systems. Lot of literature
and information is available in the published literature citation of which
would make this write up voluminous hence not attempted. However, the websites
referred above provide sufficient information for a beginner. Full complement
of information can be obtained by contacting appropriate bodies. No attempt has
been made to provide information about Yoga and Naturopathy systems because
they are mainly non-drug therapies. Similarly, Homoeopathy system has not been
discussed since it is well known out side Indian sub-continent.
History of Ayurveda� a heritage
of healing
The Origins �
The word �veda� means knowledge. The
evolution of the Indian art of healing and living a healthy life comes from the
four Vedas namely: Rig veda, Sama veda, Yajur veda and Atharva veda. Ayurveda
attained a state of reverence and is classified as one of the Upa-Vedas - a
subsection - attached to the Atharva Veda. The Atharva Veda contains not only
the magic spells and the occult sciences but also the Ayurveda that deals with
the diseases, injuries, fertility, sanity and health.
Ayurveda incorporates all forms
of lifestyle in therapy. Thus yoga, aroma, meditation, gems, amulets, herbs,
diet, astrology, color and surgery etc. are used in a comprehensive manner in
treating patients. Treating important and sensitive spots on the body called Marmas
is described in Ayurveda. Massages, exercises and yoga are recommended.
History
The knowledge we have now is by
three surviving texts of Charaka, Sushruta and Vaghbata.
Charaka (1st century A.D.) wrote
Charaka Samhita (samhita- meaning collection of verses written in Sanskrit).
Sushruta (4th century A.D.) wrote his Samhita i.e Sushruta Samhita.
Vaghbata (5th century A.D.)
compiled the third set of major texts called Ashtanga Hridaya and Ashtanga
Sangraha. Charaka�s School of Physicians and Sushruta�s School of Surgeons
became the basis of Ayurveda and helped organize and systematically classify
into branches of medicine and surgery.
Sixteen major supplements
(Nighantus) were written in the ensuing years � Dhanvantari Bahavaprakasha,
Raja and Shaligrama to name a few � that helped refine the practice of
Ayurveda. New drugs were added and ineffective ones were discarded. Expansion
of application, identification of new illnesses and finding substitute
treatments seemed to have been an evolving process. Close to 2000 plants that
were used in healing diseases and abating symptoms were identified in these
supplements.
Dridhabala in the 4th century
revised the Charaka Samhita. The texts of Sushruta Samhita were revised and
supplemented by Nagarjuna in the 6th century.
There developed eight branches/divisions of Ayurveda:
1. Kaya-chikitsa (Internal Medicine)
2. Shalakya Tantra (surgery and treatment of head and neck,
Ophthalmology and ear, nose, throat)
3. Shalya Tantra (Surgery)
4. Agada Tantra (Toxicology)
5. Bhuta Vidya (Psychiatry)
6. Kaumara bhritya (Pediatrics)
7. Rasayana (science of rejuvenation or anti-ageing)
8. Vajikarana (the science of fertility and aphrodisiac)
Many modern medications were
derived from plants alluded to in Ayurveda texts. The oft-cited example is that
of Rauwolfia serpentina that was used to treat headache, anxiety and snakebite.
Its derivative is used in treating blood pressure today.
Two areas of contribution of
Indian physicians were in treating snakebite and prevention of small pox.
Detailed account of steps to be followed after a poisonous snake bite including
application of tourniquet and lancing the site by connecting the two fang marks
and sucking the poison out is described. A decoction of the medicinal plant
Rauwolfia serpentina is next applied to the wound.
A form of vaccination for small
pox was commonly practiced in India long before the West discovered the method.
A small dose of pus from the pustule of small pox lesion was inoculated to
develop resistance.
Charaka Samhita Charaka was said
to have been in the court of the Kushana king, Kanishka during the 1st century
A. D. Some authors date him as far back as the 6th century B.C. during Buddha
period. The sacred trust between physician and patient was held in high esteem
by Charaka and patient confidentiality, similar to the Hippocratic Oath, was
deemed the proper conduct for a practicing physician. Charaka also told us that
the word Ayurveda was derived from Ayus, meaning life and Veda meaning
knowledge. Nevertheless, according to Charaka the word Ayus denotes more than
just life. Ayus denotes a combination of the body, sense organs, mind and soul.
The principles of treatment in Charaka�s teachings took a holistic approach
that treated not just the symptoms of the disease but the body, mind and soul
as single entity.
Compiled by Charaka in the form
of discussions and symposiums held by many scholars, Charaka Samhita is the
most ancient and authoritative text that has survived. Written in Sanskrit in
verse form, it has 8400 metrical verses. The Samhita deals mainly with the
diagnosis and treatment of disease process through internal and external
application of medicine. Called Kaya-chikitsa (internal medicine), it aims at
treating both the body and the spirit and to strike a balance between the two.
Following diagnosis, a series of methods to purify both the body and spirit
with purgation and detoxification, bloodletting and emesis as well as enema
(known as Pancha-karma) are utilized. The emphasis seems to be to tackle
diseases in the early phase or in a preventative manner before the first
symptoms appear.
Ayurvedic diagnosis and treatment is traditionally divided
into eight branches (sthanas) based on the approach of a physician towards a
disease process. Charaka described them thus:
1. Sutra-sthana - generalprinciples
2. Nidana-sthana - pathology
3. Vimana-sthan- diagnostics
4. Sharira-sthana - physiology and anatomy
5. Indriya-sthana - prognosis
6. Chikitsa-sthana - therapeutics
7. Kalpa-sthana - pharmaceutics
8. Siddhi-sthana - successful treatment.
Detailed accounts of various
methods of diagnosis, study of various stages of symptoms and the comprehensive
management and treatment of debilitating diseases like diabetes mellitus,
tuberculosis, asthma and arthritic conditions are to be found in the Charaka
Samhita. There is even a detailed account of fetal development in the mother�s
womb, which can rival descriptions of modern medical textbooks.
Charaka also wrote details about
building a hospital. A good hospital should be located in a breezy spot free of
smoke and objectionable smells and noises. Even the equipment needed including
the brooms and brushes are detailed. The personnel should be clean and well
behaved. Details about the rooms, cooking area and the privies are given.
Conversation, recitations and entertainment of the patient were encouraged and
said to aid in healing the ailing patient.
SushrutaSamhita Sushruta was a
surgeon in the Gupta courts in the 4th century A.D. Though Indian classics is
full of accounts of healing through transplantation of head and limbs as well
as eye balls, Sushruta Samhita is the first authentic text to describe
methodology of plastic surgery, cosmetic and prosthetic surgery, Cesarean
section and setting of compound fractures.
Sushruta had in his possession an
armamentarium of 125 surgical instruments made of stone, metal and wood.
Forceps, scalpels, trocars, catheters, syringes, saws, needles and scissors
were all available to the surgeon. Rhinoplasty (plastic surgery of the nose)
was first presented to the world medical community by Sushruta in his Samhita,
where a detailed method of transposition of a forehead flap to reconstruct a
severed nose is given. Severed noses were common form of punishment. Torn ear
lobes also were common due to heavy jewelry worn on ear lobes. Sushruta
described a method of repair of the torn ear lobes. Fitting of prosthetics for
severed limbs were also commonly performed feats. Sushruta wrote, �Only the
union of medicine and surgery constitutes the complete doctor. The doctor who
lacks knowledge of one of these branches is like a bird with only one wing.�
While Charaka concentrated on the kaya-chikitsa (internal medicine). Sushruta�s
work mainly expounded on the Shalya Tantra (surgery).
The Samhita contains mostly
poetry verses but also has some details in prose. 72 different ophthalmic
diseases and their treatment are mentioned in great detail. Pterygium, glaucoma
and treatment of conjunctivitis were well known to Sushruta. Removal of
cataract by a method called couching, wherein the opaque lens is pushed to a
side to improve vision was practiced routinely. Techniques of suturing and many
varieties of bandaging, puncturing and probing, drainage and extraction are
detailed in the manuscript.
Ashtanga Hridaya Vaghbata in the
5th century compiled two sets of texts called Ashtanga Sangraha and Ashtanga
Hridaya. It details the Kaya-chikitsa of Charaka Samhita and the various
surgical procedures of Sushruta Samhita. The emphasis seems to be more on the
physiological rather than the spiritual aspects of the disease processes.
Ashtanga Sangraha is written in prose whereas the Ashtanga Hridaya is in poetry
for recitation of the Verses.
The Ancient ayurvedic Physician
Originally only Brahmins (a certain caste) were practicing physicians. Later
people from other castes became well versed in the art of healing and a term
Vaidya came to be applied to the practitioners. Merely by their art and
knowledge, the physicians gained high social status regardless of their caste
of birth. The court physician was of political importance and sat on the right
side of the throne, an important symbolic place. Though the physician, patient,
the nurse and the medicine were all important in curing a disease, the
physician was thought to be the most important.
The codes of conduct for
physicians and medical students were laid down by the texts. The poor and
downtrodden were to be treated free of charge. Others were charged according to
their ability to pay.
The physician was expected to
behave in an exemplary manner, conforming to the highest ideals of professional
and personal life. His dress, manner and speech were expected to be beyond
reproach. Medical education was arduous, consisting of many years of sacrifice
learning the art of healing. Visiting the sick, collecting herbs and
preparation of drugs, memorizing the Vedic texts of Ayurveda, performing procedures
on dead animals, melons, and leather bottles and bladders were part of the
training. These exercises helped refine both theoretical and practical training
of the student. When finally, the student is deemed ready to practice on his
own, he was certified by the ruler.
Recent History before Ayurveda
began its recent renewal in the West, it went through a period of decline in
India when Western medical education became dominant during the era of British
rule.
Ayurveda became a second-class
option used primarily by traditional spiritual practitioners and the poor.
After India gained its independence in 1947, Ayurveda gained ground and new
schools began to be established. Today more than five hundred Ayurvedic
companies and hospitals have opened in the last ten years, and several hundred
schools have been established. Although Ayurveda remains a secondary system of
health care in India, the trend toward complementary care is emerging, and
Western and Ayurvedic physicians often work side by side.
Interest in Ayurveda in the West
began in the mid 1970's as Ayurvedic teachers from India began visiting the
United States and Europe. By sharing their knowledge, they have inspired a vast
movement toward body-mind-spirit medicine. Today Ayurvedic colleges are opening
throughout Europe, Australia, and the United States.
OUR COSMIC BEGINNING
TRIGUNA
Three primordial forces, or
principles (GUNAS) namely Sattva, Rajas & Tamas, interweaving to create the
five elements - space, air, fire, water and earth � birth the entire creation.
The principle of stillness,
tamas, replenishes the universe and its beings and is the main principle of
support within the physical universe. The principle of self-organizing
activity, rajas, gives motility and co-ordination to the universe and human
life. The Principal of harmonic and cosmic intelligence, sattva, maintains
universal and individual stasis and awareness. These three cosmic principles,
called gunas, operating through the five elements they have created, directly
interface with human existence.
On the physical plane, tamas
works closely with the physical functions of the body, summarized as bodily
humors called doshas, tissues and wastes. Tamas is said to exercise the
greatest influence on the body�s water aspect, or Kapha dosha(humour)* human
and gives the body its ability to cogitate and to endure long periods of
gestation. Rajas influences the psychic plane of existence and works closely
with the psychological functions of the body. On the physical level, rajas is
said to exercise the most influence on the body�s air aspect, Vata Dosha
(humour)*. It gives us our power to transform what is being perceived
externally into thoughts, concepts, visions, and dreams.
Referred to as the universe�s
cosmic intelligence, the third principle sattva, permeates each and every
minute cell of our being. It functions through our existential states of
awareness, although it also influences the physical organism to some extent.
Within the physical body, sattva is said to exercise the most influence on its
fire aspect, Pitta dosha (humour)*. Closely linked to the universal subtle
fire, tejas, the sattva principle maintains the cosmic memory of the entire
creation- the collective memory of every human- each individual�s memory
accumulated from the beginning of time through each rebirth until the present
time i.e.� our personal wisdom.
*all the above mentioned doshas
will be explained in detail in the coming chapter (tridosh)The Panchamahabhutas
As mentioned earlier the three
primordial forces (sattva, rajas & tamas) interweave to create the five
elements (panchmahabhutas) which birth the entire creation.
According to Ayurveda everything
in life is composed of the Panchamahabhutas � Akash (Space), Vayu (Air), Jal
(Water), Agni (Fire) and Prithvi (Earth). Omnipresent, they are mixed in an
infinite variety of relative proportions such that each form of matter is
distinctly unique. Constantly changing and interacting with each other, they
create a situation of dynamic flux that keeps the world going.
This is a small example: Within a
simple, single living cell for example the earth element predominates by giving
structure to the cell. The water element is present in the cytoplasm or the
liquid within the cell membrane. The fire element regulates the metabolic
processes regulating the cell. While the air element predominates the gases
therein. The space occupied by the cell denoting the last of the elements.
In the case of a complex,
multi-cellular organism as a human being for instance, akash (space) corresponds
to spaces within the body (mouth, nostrils, abdomen etc.); vayu (air) denotes
the movement (essentially muscular); agni (fire) controls the functioning of
enzymes (intelligence, digestive system, metabolism); jal (water) is in all
body fluids (as plasma, saliva, digestive juices); and prithvi (earth)
manifests itself in the solid structure of the body (bones, teeth, flesh, hair
et al).
The Panchmahabhutas therefore
serve as the foundation of all diagnosis treatment modalities in Ayurveda and
has served as a most valuable theory for physicians to detect and treat illness
of the body and mind successfully. For example, if a person has more of the
fire element in the body he may suffer from more acid secretion (gastric/
digestive), which if causing harm in the form of hyperacidity etc., can be
controlled by giving him food which contains more of jala (water) mahabhuta in
it like sugarcane juice etc. ������������������������������������������������������������������������������
(back to content)
1.2.6.4 Yoga Therapy: An Overview �
�Yoga Chikitsa is virtually as
old as Yoga itself, indeed, the �return of mind that feels separated from the
Universe in which it exists� represents the first Yoga therapy. Yoga Chikitsa
could be termed as �man�s first attempt at unitive understanding of
mind-emotions-physical distress and is the oldest wholistic concept and therapy
in the world.� - Yogamaharishi Dr. Swami Gitananda Giri, ICYER at Ananda
Ashram, Pondicherry.
Yoga may be said to be as ancient
as the universe itself, since it is said to have been originated by
Hiranyagarba, the causal germ plasm itself. This timeless art and science of
humanity sprouted from the fertile soil of Sanathana Dharma, the traditional
pan-Indian culture that continues to flourish into modern times.
Today, Yoga has become popular as
a therapy, and most people come to it seeking to alleviate their physical,
mental and emotional imbalances. We must understand, however, that the use of
Yoga as a therapy is a much more recent happening in the wonderful long history
of Yoga�which has historically served to promote spiritual evolution. Yoga
helps unify all aspects of our very being: the physical body, in which we live
our daily life; the energy body, without which we will not have the capacity to
do what we do; the mind body, which enables us to do our tasks with
mindfulness; the higher intellect, which gives us clarity; and, finally, the
universal body, which gives us limitless bliss. �
All aspects of our
life--physical, energetic, mental, intellectual and universal--are unified
through the practice of Yoga, which may also be described as the science of
right-use-ness, that is, of using our body, emotions, and mind responsibly and
in the most appropriate manner. One of the best definitions of Yoga given by
Swami Gitananda Giri is that it is a �way of life�. It is not something you do
for 5 minutes a day or 20 minutes a day. It is indeed a 24 � 7 � 365.
lifestyle.
Illness, disease and disorders
are so common in this world, and people everywhere are desperately seeking
relief from their suffering. Yoga helps us to think better and to live better;
indeed, it helps us improve ourselves in everything we do. Hence it holds out
the promise of health, well-being and harmony. According to the Bhagavad Gita,
an ancient text which can be said to be a Yoga Shastra (seminal textual source
of Yoga), Lord Krishna the Master of Yoga (Yogeshwar) defines Yoga as
�dukkhasamyogaviyogam yoga samjnitham� meaning thereby that Yoga is the
disassociation from the union with suffering. Pain, suffering, disease - Yoga offers
a way out of all of these.
One of the foremost concepts of
Yoga therapy is that the mind, which is called adhi, influences the body, thus
creating vyadhi, the disease. (Fig 1)
This is known as the adhi vyadhi
or adhija vyadhi, where the mind brings about the production of disease in the
physical body. In modern language, this is called psychosomatic illness.
Virtually every health problem that we face today either has its origin in
psychosomatics or is worsened by the psychosomatic aspect of the disease. The
mind and the body seem to be continuously fighting each other.
What the mind wants, the body
won�t do, and what the body wants, the mind won�t do. This creates a dichotomy,
a disharmony, in other words, a disease.
Yoga helps restore balance and equilibriumby
virtue of the internal process of unifying mind, body and emotions. The
psychosomatic stress disorders that are so prevalent in today�s world can be
prevented, controlled and possibly even cured via the sincere and dedicated
application of Yoga as a therapy.
Psychosomatic disorders go
through four major phases. The first is the psychic phase, in which the stress
is located essentially in the mind. There is jitteriness, a sense of unnatural
tension, a sense of not being �at ease�.
If the stress continues, the
psychic stage then evolves into the psychosomatic stage. At this point, the
mind and body are troubling each other and fluctuations, such as a dramatic
rise in blood pressure, blood sugar or heart rate, begin to manifest
intermittently. If this is allowed to continue, one reaches the somatic stage,
where the disease settles down in the body and manifests permanently. At this
stage, it has become a condition that requires treatment and therapy. In the
fourth, organic stage, the disease settles permanently into the target organs.
This represents the end stage of the disease.
Yoga as a therapy works very well
at both the psychic and psychosomatic stages. Once the disease enters the
somatic stage, Yoga therapy as an adjunct to other therapies may improve the
condition. In the organic stage, Yoga therapy�s role is more of a palliative,
pain relieving and rehabilitative nature. Of course the major role of Yoga is
as a preventive therapy, preventing that which is to come. Maharishi Patanjali
tells us in his Yoga Darshan, �heyamdukkhamanagatham�-prevent those miseries
that are yet to come�. �
If the practice of Yoga is taken
up during childhood, we can prevent so many conditions from occurring later on
in life. This is primary prevention. Once the condition occurs, once the
disease has set in, we have secondary prevention, which is more in the nature
of controlling the condition to whatever extent we can. Tertiary prevention is
done once the condition has occurred, as we try to prevent the complications,
those that affect the quality, and even the quantity, of a patient�s life.
When we use Yoga as a therapy, we
need to consider both the nature of the person�his or her age, gender and
physical condition�and the nature and stage of the disorder. A step-by-step
approach must include a detailed look at all aspects of diet, necessary
lifestyle modifications, attitude reconditioning through Yogic counseling, as
well as the appropriate practices. All of these are integral components of
holistic, or rather, wholesome Yoga therapy. When such an approach is adopted,
tremendous changes will manifest in the lives of the patients and their
families. The quality of life improves drastically and, in many cases, so does
the quantity.
As human beings, we fulfill ourselves
best when we help others. Yoga is the best way for us to consciously evolve out
of our lower, sub-human nature, into our elevated human and humane nature.
Ultimately, this life giving, life enhancing and life sustaining science of
humanity allows us to achieve in full measure the Divinity that resides within
each of us.
I would like to conclude this
overview of Yoga therapy with a word of caution. Yoga therapy is not a magic
therapy! It is not a �one pill for all ills�. There should be no false claims
or unsubstantiated tall claims made in this field. Yoga therapy is also a
science and must therefore be approached in a scientific, step-bystep manner.
It should be administered primarily as a �one on one� therapy that allows the
therapist to modify the practices to meet the needs of the individual. It is
not a �one size fits all� or �one therapy fits all� approach!
(back
to content)
1.2.6.5 Siddha medicine w
Siddha medicine is a traditional
medicine originating in Southern India. It is one of the oldest systems of
medicine in India.
In rural India, siddhars have
learned methods traditionally through master-disciple relationships to become
local "healers". Siddhars are among an estimated 400,000 traditional
healers practicing medicine in India, comprising some 57% of rural medical
care. Siddha practitioners believe that five basic elements � earth, water,
fire, air, sky � are in food, "humours" of the human body, and
herbal, animal or inorganic chemical compounds, such as sulfur and mercury,
used as therapies for treating diseases.
The Ministry of Ayurveda, Yoga
and Naturopathy, Unani, Siddha and Homoeopathy of the Government of India
regulates training in Siddha medicine and other traditional practices grouped
collectively as AYUSH. Practitioners are called siddhars (vaithiyars in Tamil),
and may have formal training with advanced degrees, such as BSMS (Bachelor in
Siddha Medicine and Surgery), MD (Medical Doctor, Siddha) or Doctor of
Philosophy (PhD). The Central Council of Indian Medicine, a statutory body
established in 1971 under AYUSH, monitors education in areas of rural Indian
medicine, including Siddha medicine. The Indian Medical Association regards
Siddha medicine degrees as "fake" and Siddha therapies as quackery,
posing a danger to national health due to absence of training in science-based
medicine. Identifying fake medical practitioners without qualifications, the
Supreme Court of India stated in 2018 that "unqualified, untrained quacks
are posing a great risk to the entire society and playing with the lives of
people without having the requisite training and education in the science from
approved institutions".
HISTORY
Siddha is an ancient Indian
traditional treatment system which evolved in South India, and is dated to the
times of 3rd millennium BCE Indus Valley Civilization or earlier. According to
ancient literature of Siddha, it is said that the system of this medicine
originated from Hindu God Shiva who taught it to his consort Parvati. Parvati
then passed it on to Nandi and Nandi taught about it to nine Devtas.
Though the origin of this system
is considered to be divine, Siddhar Agasthyar is considered as the founding
father of this medical system. There are 18 prominent siddhars who are the main
contributors to this system of medicine. The original texts and treatise for
siddha are written in Tamil language.
CONCEPT OF DISEASE AND CAUSE
When the normal equilibrium of
the three humors � Vaadham, Pittham and Kapam � is disturbed, disease is
caused. The factors assumed to affect this equilibrium are environment,
climatic conditions, diet, physical activities, and stress. Under normal
conditions, the ratio between Vaadham, Pittham, and Kapam are 4:2:1,
respectively.
According to the Siddha medicine
system, diet and lifestyle play a major role in health and in curing diseases.
This concept of the Siddha medicine is termed as pathiyam and apathiyam, which
is essentially a rule based system with a list of "do's and don'ts".
HERBALISM
The herbal agents used by the
siddhars could be classified into three groups: thavaram (herbal product),
thadhu (inorganic substances) and jangamam (animal products). The thadhu agents
are further classified as: uppu (water-soluble inorganic substances that give
out vapour when put into fire), pashanam (agents not dissolved in water but
emit vapour when fired), uparasam (similar to pashanam but differ in action),
loham (not dissolved in water but melt when fired), rasam (substances which are
soft), and ghandhagam (substances which are insoluble in water, like sulphur).
SIDDHA TODAY
The Tamil Nadu state runs a
5.5-year course in Siddha medicine (BSMS: Bachelor in Siddha Medicine and Surgery).
The Indian Government also gives its focus on Siddha, by starting up medical
colleges and research centers like National Institute of Siddha. and Central
Council for Research in Siddha. Commercially, Siddha medicine is practiced by
siddhars referred in Tamil as vaithiyars.
Practicing Siddha medicine and
similar forms of rural alternative medicine in India was banned in the
Travancore-Cochin Medical Practitioners' Act of 1953, then reinforced in 2018
by the Supreme Court of India which stated that "A number of unqualified,
untrained quacks are posing a great risk to the entire society and playing with
the lives of people." The Act requires that qualified medical
practitioners be trained at a recognized institution, and be registered and
displayed on a list of valid physician practitioners, as published annually in
The Gazette of India. The Gazette list does not recognize practitioners of
Siddha medicine because they are not trained, qualified or registered as valid
physicians.
Since 2014, the Supreme Court of
India and Indian Medical Association have described Siddha medicine as
quackery, and there is no governmental recognition of siddhars as legitimate
physicians. The Indian Medical Association regards the Indian institutions that
train people in Siddha medicine, the supposed degrees granted, and the graduates
of those programs as "fake". Since 1953, the Indian national
government has not recognized Siddha medicine or any alternative system of
medicine as valid, and there is no proposal to integrate Siddha medicine into
conventional medicine practiced in India.
There may be as many as one
million quack "doctors", including siddhars, practicing medicine in
the rural regions of India, a condition not actively opposed by the Indian
government out of concern for serving some health needs for the large rural
population. The Indian Medical Association emphatically opposed this position
in 2014. In 2018, licensed Indian physicians staged demonstrations and accused
the government of sanctioning quackery by proposing to allow rural quacks to
practice some aspects of clinical medicine without having complete medical
training.
(back
to content)
1.2.7 Thai massage w
Thai massage or Thai yoga massage
is a traditional therapy combining acupressure, Indian Ayurvedic principles,
and assisted yoga postures. The idea of Sen-lines alias energy-lines was first
used as "Thai yoga massage". These are similar to nadis as per the
philosophy of yoga by Gorakhnath.
Nuad Thai, traditional Thai massage
UNESCO Intangible Cultural Heritage
�
Thai massage
Country �������������������������������������������������������������������������������������������������������������� Thailand
Region ���������������������������������������������������������������������������������������������������������������� Asia
and the Pacific
Inscription
history
Inscription ��������������������������������������������������������������������������������������������������������� 2019
(14th session)
List ����������������������������������������������������������������������������������������������������������������������� Representative
In the Thai language it is
usually called nuat phaen thai (Thai: นวดแผนไทย,
pronounced [n�a̯t pʰɛ̌ːn tʰāj]; lit.
'Thai-style massage') or nuat phaen boran (นวดแผนโบราณ,
[n�a̯t pʰɛ̌ːn bōːrāːn]; lit.
'ancient-style massage'), though its formal name is nuat thai (นวดไทย,
[n�a̯t tʰāj]; lit. 'Thai massage') according to the Traditional
Thai Medical Professions Act, BE 2556 (2013).
The Thai Ministry of Public
Health's Department for Development of Thai Traditional and Alternative
Medicine regulates Thai traditional massage venues and practitioners. As of
2016 the department says 913 traditional clinics have registered nationwide in
Thailand. As of 2018, of the 8,000 to 10,000 spa and massage shops in Thailand;
only 4,228 are certified by the Health Ministry's Department of Health Service
Support (HSS).
UNESCO added traditional Thai
massage to its Cultural Heritage of Humanity list in December 2019.
Practice
The practice of Thai yoga massage
is said to be thousands of years old, but it is still part of Thailand's
medical system due to its perceived healing properties at both emotional and
physical level. There are differences in certain practices associated with the
massage when performed in the Western and Thai contexts. Western cultural
sensibilities might be different in terms of accepting shamanic healing practices
such as increasing the intensity of the massage or the giver jumping around the
massage table like the Hindu god Hanuman. Traditional Thai massage uses no oils
or lotions. The recipient remains clothed during a treatment. There is constant
body contact between the giver and receiver, but rather than rubbing on
muscles, the body is compressed, pulled, stretched and rocked. The concept of
metta (loving kindness), based on Buddhist teachings, is an integral part of
this practice. Well known practitioners also emphasize meditation and devotion
on part of the practitioner as integral to the effectiveness of this practice.
The recipient wears loose,
comfortable clothing and lies on a mat or firm mattress on the floor.
In Thailand, a dozen or so
subjects may receive massage simultaneously in one large room. The true ancient
style of the massage requires that the massage be performed solo with just the
giver and receiver. The receiver will be positioned in a variety of yoga-like
positions during the course of the massage, that is also combined with deep
static and rhythmic pressures.
The massage generally follows
designated lines ("sen") in the body. The legs and feet of the giver
can be used to position the body or limbs of the recipient. In other positions,
hands fix the body, while the feet do the massaging. A full Thai massage
session may last two hours and includes rhythmic pressing and stretching of the
entire body. This may include pulling fingers, toes, ears, cracking knuckles,
walking on the recipient's back, by palm-press, thumb-press, fingers-press and
forearm-press in many different positions including HDS. There is a standard
procedure and rhythm to the massage, which the giver will adjust to fit the
receiver.
History
�
Drawings of acupressure points on sen lines at Wat Pho
Temple, Phra Nakhon district, Bangkok
The founder of Thai massage and
medicine is said to have been Chiwaka Komaraphat (ชีวกโก มารภัจจ์
Jīvaka Komarabhācca), who is said in the Pāli Buddhist canon to
have been the Buddha's physician over 2,500 years ago. He is recorded in
ancient documents as having extraordinary medical skills, his knowledge of
herbal medicine, and for having treated important people of his day, including
the Buddha himself.
In fact, the history of Thai
massage is more complex than this legend of a single founder would suggest.
Thai massage, like Thai traditional medicine (TTM) more generally, is a
combination of influences from Indian and Southeast Asian traditions of
medicine, and the art as it is practiced today is likely to be the product of a
19th-century synthesis of various healing traditions from all over the kingdom.
Even today, there is considerable variation from region to region across
Thailand, and no single routine or theoretical framework that is universally
accepted among healers.
(back
to content)
1.2.8 Japan w
Kampo
Kanpō medicine (漢方医学,
Kanpō igaku), often known simply as Kanpō (漢方,
Chinese [medicine]), is the study of traditional Chinese medicine in Japan
following its introduction, beginning in the 7th century. then adapted and
modified to suit Japanese culture and traditions. Traditional Japanese medicine
(TJM) uses most of the Chinese therapies including acupuncture, moxibustion,
traditional Chinese herbology and traditional food therapy.
Kampo
Japanese name
Kanji���������������������������������������������������������������������
漢方医学
Transcriptions
Romanization ��������������������������������������������������� Kanpō
igaku
Chinese name
Traditional Chinese ��������������������������������������� 日本漢方醫學
Simplified Chinese ��������� ������������������������������� 日本汉方医学
Literal meaning ������������������������������� "Han
[Chinese] medicine in Japan"
Transcriptions
Standard Mandarin
Hanyu Pinyin ���������������������������������������������������� R�běn
H�nfāng yīxu�
Yue: Cantonese
Yale Romanization ����������������������������������������� Yaht-b�n
Hon-fōng yī-hohk
|
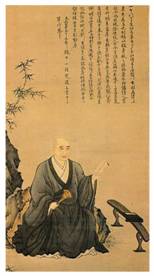
|
Shennong (Japanese: Shinnō) tasting herbs to ascertain their
qualities (19th-century Japanese scroll)
|
|

|
Manase Dōsan (1507�94) who laid the foundations for a more
independent Japanese medicine
|
|
|
|
Origins
According to Chinese mythology,
the origins of traditional Chinese medicine are traced back to the three
legendary sovereigns Fuxi, Shennong and Yellow Emperor. Shennong is believed to
have tasted hundreds of herbs to ascertain their medicinal value and effects on
the human body and help relieve people of their sufferings. The oldest written
record focusing solely on the medicinal use of plants was the Shennong Ben Cao
Jing which was compiled around the end of the first century B.C. and is said to
have classified 365 species of herbs or medicinal plants. Chinese medical
practices were introduced to Japan during the 6th century A.D. In 608, Empress
Suiko dispatched E-Nichi, Fuku-In and other young physicians to China. It is
said that they studied medicine there for 15 years. Until 838, Japan sent 19
missions to Tang China. While the Manase Dōsan (1507�94) who laid the
foundations for a more independent Japanese medicine History officials studied
Chinese government structures, physicians and many of the Japanese monks
absorbed Chinese medical knowledge.
Early Japanese adaptation
In 702 A.D., the Taihō Code
was promulgated as an adaptation of the governmental system of China's Tang
Dynasty. One section called for the establishment of a university (daigaku)
including a medical school with an elaborate training program, but due to
incessant civil war this program never became effective. Empress
Kōmyō (701�760) established the Hidenin and Seyakuin in the
Kōfuku-Temple (Kōfuku-ji) in Nara, being two Buddhist institutions
that provided free healthcare and medicine for the needy. For centuries to come
Japanese Buddhist monks were essential in conveying Chinese medical know-how to
Japan and in providing health care for both the elite and the general
population.
In 753 A.D., the Chinese priest
Jianzhen (in Japanese Ganjin), who was well-versed in medicine, arrived in
Japan after five failed attempts in 12 years to cross the East China Sea. As he
was blind, he used his sense of smell to identify herbs. He brought medical
texts and a large collection of materia medica to the imperial palace in Nara,
which he dedicated to the Emperor Shōmu in 756, 49 days after the
emperor's death. They are kept in a log-cabin-style treasure house of the
Tōdai-Temple (Tōdai-ji) known as Shōsōin.
In 787 A.D., the "Newly
Revised Materia Medica" (Xinxiu Bencao, 659 A.D.), which had been
sponsored by the Tang Imperial Court, became an obligatory text in the study of
medicine at the Japanese Health Ministry, but many of the 844 medicinal
substances described in this book were not available in Japan at the time.
Around 918 A.D., a Japanese medical dictionary entitled "Japanese names of
(Chinese) Materia Medica" (Honzō-wamyō) was compiled, quoting
from 60 Chinese medical works.
During the Heian Period, Tanba
Yasuyori (912�995) compiled the first Japanese medical book, Ishinpō
("Prescriptions from the Heart of Medicine"), drawing from numerous
Chinese texts, some of which have perished later. During the period from 1200
to 1600, medicine in Japan became more practical. Most of the physicians were
Buddhist monks who continued to use the formulas, theories and practices that
had been introduced by the early envoys from Tang China.
EARLY REVISION
During the 15th and 16th
centuries, Japanese physicians began to achieve a more independent view on
Chinese medicine. After 12 years of studies in China Tashiro Sanki (1465�1537)
became the leading figure of a movement called "Followers of Later
Developments in Medicine" (Gosei-ha). This school propagated the teachings
of Li Dongyuan and Zhu Tanxi that gradually superseded the older doctrines from
the Song dynasty. Manase Dōsan, one of his disciples, adapted Tashiro's
teachings to Japanese conditions. Based on his own observation and experience,
he compiled a book on internal medicine in eight volumes (Keiteki-shū) and
established an influential private medical school (Keiteki-in) in Kyōto.
His son Gensaku wrote a book of case studies (Igaku tenshō-ki) and
developed a considerable number of new herb formulas.
From the second half of the 17th
century, a new movement, the "Followers of Classic Methods" (Kohō-ha),
evolved, which emphasized the teachings and formulas of the Chinese classic
"Treatise on Cold Damage Disorders" (Shanghan Lun, in Japanese
Shōkan-ron). While the etiological concepts of this school were as
speculative as those of the Gosei-ha, the therapeutic approaches were based on
empirical observations and practical experience. This return to "classic
methods" was initiated by Nagoya Gen'i (1628�1696), and advocated by
influential proponents such as Gotō Gonzan (1659�1733), Yamawaki
Tōyō (1705�1762), and Yoshimasu Tōdō (1702�1773). Yoshimasu
is considered to be the most influential figure. He accepted any effective
technique, regardless of its particular philosophical background. Yoshimasu's
abdominal diagnostics are commonly credited with differentiating early modern
Traditional Japanese medicine (TJM) from Traditional Chinese medicine (TCM).
During the later part of the Edo
period, many Japanese practitioners began to utilize elements of both schools.
Some, such as Ogino Gengai (1737�1806), Ishizaka Sōtetsu (1770�1841), or
Honma Sōken (1804�1872), even tried to incorporate Western concepts and
therapies, which had made their way into the country through physicians at the
Dutch trading-post Dejima (Nagasaki). Although Western medicine gained some ground
in the field of surgery, there was not much competition between
"Eastern" and "Western" schools until the 19th century,
because even adherents of "Dutch-Studies" (Rangaku) were very
eclectic in their actual practice.
Traditional medicine never lost its
popularity throughout the Edo period, but it entered a period of rapid decline
shortly after the Meiji Restoration. In 1871, the new government decided to
modernize medical education based on the German medical system. Starting in
1875, new medical examinations focused on natural sciences and Western medical
disciplines. In October 1883, a law retracted the licenses of any existing
traditional practitioner. Despite losing legal standing, a small number of
traditional physicians continued to practice privately. Some of them, such as
Yamada Gyōkō (1808�1881), Asada Sōhaku (1813�1894), and Mori
Risshi (1807� 1885), organized an "Association to Preserve [Traditional]
Knowledge" (Onchi-sha) and started to set up small hospitals. However, by
1887, the organization was disbanded due to internal policy dissent and the
death of leading figures. The "Imperial Medical Association" (Teikoku
Ikai), founded in 1894, was short-lived too. In 1895, the 8th National Assembly
of the Diet vetoed a request to continue the practice of Kampō. When Azai
Kokkan (1848�1903), one of the main activists, died, the Kampō movement
was almost stamped out.
ERA OF WESTERN INFLUENCE
Any further attempt to save
traditional practices had to take into account Western concepts and therapies. Therefore,
it was graduates from medical faculties, trained in Western medicine, who began
to set out to revive traditional practices. In 1910, Wada Keijūrō
(1872�1916) published "The Iron Hammer of the Medical World" (Ikai no
tettsui). Yumoto Kyūshin (1876�1942), a graduate from Kanazawa Medical
School, was so impressed by this book that he became a student of Dr. Wada. His
"Japanese-Chinese Medicine" (Kōkan igaku), published in 1927,
was the first book on Kampō medicine in which Western medical findings were
used to interpret classical Chinese texts. In 1927, Nakayama Tadanao
(1895�1957) presented his "New Research on Kampō-Medicine"
(Kampō-igaku no shin kenkyū). Another "convert" was
Ōtsuka Keisetsu (1900�1980), who became one of the most famous Kampō
practitioners of the 20th century.
This gradual revival was
supported by the modernization of the dosage form of herbal medicine.
During the 1920s, the Nagakura
Pharmaceutical Company in Osaka began developing dried decoctions in a granular
form. At about the same time, Tsumura Juntendō, a company founded by
Tsumura Jūsha (1871�1941) in 1893, established a research institute to
promote the development of standardized Kampō medicine. Gradually, these
"Japanese-Chinese remedies" (wakan-yaku) became a standard method of
Kampō medicine administration.
In 1937, new researchers such as
Yakazu Dōmei (1905�2002) started to promote Kampō at the so-called
"Takushoku University Kampo Seminar". More than 700 people attended
these seminars that continued after the war. In 1938, following a proposal of
Yakazu, the "Asia Medicine Association" was established. In 1941,
Takeyama Shinichirō published his "Theories on the Restoration of
Kampō Medicine" (Kampō-ijutsu fukkō no riron, 1941). In
that same year, Yakazu, Ōtsuka, Kimura Nagahisa, and Shimizu Fujitarō
(1886�1976) completed a book entitled "The Actual Practice of Kampō
Medicine" (Kampō shinryō no jissai). By including Western
medical disease names he greatly expanded the usage of Kampō formulas. A
new version of this influential manual was printed in 1954. This book was also
translated into Chinese. A completely revised version was published in 1969
under the title "Medical Dictionary of Kampō Practice"
(Kampō Shinryō Iten).
In 1950, Ōtsuka Keisetsu,
Yakazu Dōmei, Hosono Shirō (1899�1989), Okuda Kenzō (1884�1961),
and other leaders of the pre- and postwar Kampō revival movement
established the "Japan Society for Oriental Medicine" (Nippon
Tōyō Igakkai) with 89 members (2014: more than 9000 members). In
1960, raw materials for crude drugs listed in the Japanese Pharmacopoeia
(Nippon Yakkyoku-hō) received official drug prices under the National
Health Insurance (NHI, Kokumin kenkō hoken).
Today in Japan, Kampō is
integrated into the Japanese national health care system. In 1967, the Ministry
of Health, Labour and Welfare approved four Kampō medicines for
reimbursement under the National Health Insurance (NHI) program. In 1976, 82
kampo medicines were approved by the Ministry of Health, Labour and Welfare.
This number has increased to 148 Kampo formulation extracts, 241 crude drugs, and
5 crude drug preparations.

Rather than modifying formulae as
in Traditional Chinese medicine, the Japanese Kampō tradition uses fixed
combinations of herbs in standardized proportions according to the classical
literature of Chinese medicine. Kampō medicines are produced by various
manufacturers.
However, each medicine is
composed of exactly the same ingredients under the Ministry's standardization
methodology. The medicines are therefore prepared under strict manufacturing
conditions that rival pharmaceutical companies. In October 2000, a nationwide
study reported that 72% of registered physicians prescribe Kampō
medicines. New Kampō medicines are being evaluated using modern techniques
to evaluate their mechanism of action.
The 14th edition of the Japanese
Pharmacopoeia (JP, Nihon yakkyokuhō) lists 165 herbal ingredients that are
used in Kampō medicines. Lots of the Kampō products are routinely
tested for heavy metals, purity, and microbial content to eliminate any
contamination. Kampō medicines are tested for the levels of key chemical
constituents as markers for quality control on every formula. This is carried
out from the blending of the raw herbs to the end product according to the
Ministry's pharmaceutical standards.
Approved Kampō medicines
Herbs
Medicinal mushrooms like Reishi
and Shiitake are herbal products with a long history of use. In Japan, the
Agaricus blazei mushroom is a highly popular herb, which is used by close to 500,000
people. In Japan, Agaricus blazei is also the most popular herb used by cancer
patients.
The second most used herb is an
isolate from the Shiitake mushroom, known as Active Hexose Correlated Compound.
In the United States, Kampō
is practiced mostly by acupuncturists, Chinese medicine practitioners,
naturopath physicians, and other alternative medicine professionals. Kampō
herbal formulae are studied under clinical trials, such as the clinical study
of Honso Sho-saiko-to (H09) for treatment of hepatitis C at the New York
Memorial Sloan-Kettering Cancer Center, and liver cirrhosis caused by hepatitis
C at the UCSD Liver Center. Both clinical trials are sponsored by Honso USA,
Inc., a branch of Honso Pharmaceutical Co., Ltd., Nagoya, Japan.
One of the first sources showing
the term "Kampō" in its modern sense (James Curtis Hepburn: A
Japanese and English Dictionary; with an English and Japanese Index. London:
Tr�bner & Co., 1867, p. 177.)
(back
to content)
1.2.8.1 Reiki w
Reiki (霊気,
/ˈreɪki/) is a Japanese form of energy healing, a type of alternative
medicine. Reiki practitioners use a technique called palm healing or hands-on
healing through which a "universal energy" is said to be transferred
through the palms of the practitioner to the patient in order to encourage
emotional or physical healing.
Reiki
Chinese name
Traditional Chinese ����������������������������������������������������������������������� 靈氣
Simplified Chinese ������������������������������������������������������������������������� 灵气
Transcriptions
Standard Mandarin
Hanyu Pinyin ������������������������������������������������������������������������������������ l�ngq�
Wade�Giles �������������������������������������������������������������������������������������� ling2-ch'i4
Yue: Cantonese
Jyutping ��������������������������������������������������������������������������������������������� ling4-hei3
Vietnamese name
Vietnamese alphabet ������������������������������������������������������������������� linh
kh�
Korean name
Hangul �������������������������������������������������������������������������������� 영기
Hanja �������������������������������������������������������������������������������������������������� 靈氣
Transcriptions
Revised Romanization �������������������������������������������������� yeonggi
McCune�Reischauer ��������������������������������������������������������������������� yŏngki
Japanese name
Hiragana �������������������������������������������������������������������������������������������� れいき
Kyūjitai ������������������������������������������������������������������������������� 靈氣
Shinjitai ���������������������������������������������������������������������������������������������� 霊気
Reiki is a pseudoscience, and is
used as an illustrative example of pseudoscience in scholarly texts and
academic journal articles. It is based on qi ("chi"), which
practitioners say is a universal life force, although there is no empirical
evidence that such a life force exists.
Clinical research does not show
reiki to be effective as a treatment for any medical condition, including
cancer, diabetic neuropathy, anxiety or depression; therefore, it should not
replace conventional medical treatment. There is no proof of the effectiveness
of reiki therapy compared to placebo. Studies reporting positive effects have
had methodological flaws.
Etymology
Mikao Usui (1865�1926)
According to the Oxford English Dictionary, the English alternative
medicine word reiki comes from Japanese reiki (霊気)
"mysterious atmosphere, miraculous sign", combining rei "soul,
spirit" and ki "vital energy"�the Sino-Japanese reading of
Chinese l�ngq� (靈氣) "numinous atmosphere".
According to the inscription on
his memorial stone, Mikao Usui taught his system of reiki to more than 2,000
people during his lifetime. While teaching reiki in Fukuyama, Usui suffered a
stroke and died on 9 March 1926. The first reiki clinic in the United States
was started by Chujiro Hayashi's student Hawayo Takata in 1970.
Basis
Reiki's teachings and adherents
claim that qi is physiological and can be manipulated to treat a disease or
condition. The existence of qi has not been established by medical research.
Therefore, reiki is a pseudoscientific theory based on metaphysical concepts.
The existence of the proposed
mechanism for reiki�qi or "life force" energy�has not been
scientifically established. Most research on reiki is poorly designed and prone
to bias. There is no reliable empirical evidence that reiki is helpful for
treating any medical condition,
Chujiro Hayashi (1880�1940)
Origins
Research and critical evaluation
although some physicians have said it might help promote general well-being. In
2011, William T. Jarvis of The National Council Against Health Fraud stated
that there "is no evidence that clinical reiki's effects are due to
anything other than suggestion" or the placebo effect.
The April 22, 2014, Skeptoid
podcast episode titled "Your Body's Alleged Energy Fields" relates a
reiki practitioner's report of what was happening as she passed her hands over
a subject's body:
What we'll be looking for here,
within John's auric field, is any areas of intense heat, unusual coldness, a
repelling energy, a dense energy, a magnetizing energy, tingling sensations, or
actually the body attracting the hands into that area where it needs the reiki
energy, and balancing of John's qi.
Evaluating these claims
scientific skeptic author Brian Dunning reported: ... his aura, his qi, his
reiki energy. None of these have any counterpart in the physical world.
Although she attempted to describe their properties as heat or magnetism, those
properties are already taken by �well, heat and magnetism. There are no
properties attributable to the mysterious field she describes, thus it cannot
be authoritatively said to exist."
Scholarly evaluation
Reiki is used as an illustrative
example of pseudoscience in scholarly texts and academic journal articles.
In criticizing the State
University of New York for offering a continuing education course on reiki, one
source stated, "reiki postulates the existence of a universal energy
unknown to science and thus far undetectable surrounding the human body, which
practitioners can learn to manipulate using their hands," and others said,
"In spite of its [reiki] diffusion, the baseline mechanism of action has
not been demonstrated ..." and, "Neither the forces involved nor the
alleged therapeutic benefits have been demonstrated by scientific
testing."
Several authors have pointed to
the vitalistic energy which reiki is claimed to treat, with one saying,
"Ironically, the only thing that distinguishes reiki from therapeutic
touch is that it [reiki] involves actual touch," and others stating that
the International Center for Reiki Training "mimic[s] the institutional
aspects of science" seeking legitimacy but holds no more promise than an
alchemy society.
A guideline published by the
American Academy of Neurology, the American Association of
Neuromuscular &
Electrodiagnostic Medicine, and the American Academy of Physical Medicine and
Rehabilitation states, "Reiki therapy should probably not be considered
for the treatment of PDN [painful diabetic neuropathy]." Canadian
sociologist Susan J. Palmer has listed reiki as among the pseudoscientific
healing methods used by cults in France to attract members.
Evidence quality
A 2008 systematic review of nine
randomized clinical trials found several shortcomings in the literature on
reiki. Depending on the tools used to measure depression and anxiety, the
results varied and were not reliable or valid. Furthermore, the scientific
community has been unable to replicate the findings of studies that support
reiki. The review also found issues in reporting methodology in some of the
literature, in that often there were parts omitted completely or not clearly
described. Frequently in these studies, sample sizes were not calculated and
adequate allocation and double-blind procedures were not followed. The review
also reported that such studies exaggerated the effectiveness of treatment and
there was no control for differences in experience of reiki practitioners or
even the same practitioner at times produced different outcomes. None of the
studies in the review provided a rationale for the treatment duration and no
study reported adverse effects.
Safety
Safety concerns for reiki sessions are very low and are akin to those
of many complementary and alternative medicine practices. Some physicians and
health care providers, however, believe that patients may unadvisedly
substitute proven treatments for life-threatening conditions with unproven
alternative modalities including reiki, thus endangering their health.
Catholic Church concerns
In March 2009, the Committee on Doctrine of the United States Conference
of Catholic Bishops issued the document Guidelines for Evaluating Reiki as an
Alternative Therapy, in which they declared that the practice of reiki was
based on superstition, being neither truly faith healing nor science-based
medicine. They stated that reiki was incompatible with Christian spirituality
since it involved belief in a human power over healing rather than prayer to
God, and that, viewed as a natural means of healing, it lacked scientific
credibility. The 2009 guideline concluded that "since reiki therapy is not
compatible with either Christian teaching or scientific evidence, it would be
inappropriate for Catholic institutions, such as Catholic health care
facilities and retreat centers, or persons representing the Church, such as
Catholic chaplains, to promote or to provide support for reiki therapy."
Since this announcement, some Catholic lay people have continued to practice
reiki, but it has been removed from many Catholic hospitals and other
institutions.
In a December 2014 article from the
USCCB's Committee on Divine Worship on exorcism and its use in the Church,
reiki is listed as a practice "that may have [negatively] impacted the
current state of the afflicted person".
(back
to content)
1.2.9 Rolfing w
Rolfing (/ˈrɔːlfɪŋ,
ˈrɒl-/) is a form of alternative medicine originally developed by Ida
Rolf (1896�1979) as Structural Integration. Rolfing is marketed with unproven
claims of various health benefits. It is based on Rolf's ideas about how the
human body's "energy field" can benefit when aligned with the Earth's
gravitational field.
Rolfing is typically delivered as
a series of ten hands-on physical manipulation sessions sometimes called
"the recipe". Practitioners combine superficial and deep manual therapy
with movement prompts. The process is sometimes painful. The safety of Rolfing
has not been confirmed.
The principles of Rolfing
contradict established medical knowledge, and there is no good evidence Rolfing
is effective for the treatment of any health condition. It is recognized as a
pseudoscience and has been characterized as quackery.
Science writer Edzard Ernst
offers this definition: "Rolfing is a system of bodywork invented byIda
Pauline Rolf (1896�1979) employing deep manipulation of the body's soft tissue
allegedly to realign and balance the body's myofascial structures."
Rolfing is based on the unproven
belief that such alignment results in improved movement, breathing, pain reduction,
stress reduction, and even emotional changes.
Conceptual basis
Rolf described the body as
organized around an axis perpendicular to the earth, pulled downward by
gravity, and she believed the function of the body was optimal when it was
aligned with that pull. In her view, gravity tends to shorten fascia, leading to
disorder of the body's arrangement around its axis and creating imbalance,
inefficiency in movement, and pain.
Rolfers aim to lengthen the
fascia in order to restore the body's arrangement around its axis and
facilitate improved movement. Rolf also discussed this in terms of
"energy" and said:
Rolfers make a life study of
relating bodies and their fields to the earth and its gravity field, and we so
organize the body that the gravity field can reinforce the body's energy field.
This is our primary concept.
The manipulation is sometimes
referred to as a type of bodywork, or as a type of massage. Some osteopaths
were influenced by Rolf, and some of her students became teachers of massage,
including one of the founders of myofascial release.
Rolf claimed to have found an
association between emotions and the soft tissue, writing "although
rolfing is not primarily a psychotherapeutic approach to the problems of
humans", it does constitute an "approach to the personality through
the myofascial collagen components of the physical body". She claimed
Rolfing could balance the mental and emotional aspects of subjects, and that
"the amazing psychological changes that appeared in Rolfed individuals were
completely unexpected". Rolfers suggest their manipulations can cause the
release of painful repressed memories. Rolfers also hold that by manipulating
the body they can bring about changes in personality; for example, teaching
somebody to walk with confidence will make them a more confident person. The
connection between physical structure and psychology has not been proven by
scientific studies.
History
Ida Rolf began working on clients
in New York City in the 1940s with the premise that the human structure could
be organized "in relation to gravity". She developed structural
integration with one of her sons and by the 1950s she was teaching her work
across the United States. In the mid-1960s she began teaching at Esalen
Institute, where she gathered a loyal following of students and
practitioners.[35] Esalen was the epicenter of the Human Potential Movement,
allowing Rolf to exchange ideas with many of their leaders, including Fritz
Perls. Rolf Effectiveness and reception incorporated a number of ideas from
other areas including osteopathic manipulation, cranial osteopathy, hatha yoga,
and the general semantics of Alfred Korzybski. In 1971 she founded the Rolf
Institute of Structural Integration. The school has been based in Boulder,
Colorado, since 1972, and as of 2010 included five institutes worldwide.
(back
to content)
1.2.10 Greco-Roman Medicine w
Greek medicine derived its
earliest beliefs and practices from Egypt and West Asia. Greek medicine later
spread around the Mediterranean during Roman times and was to form the basis of
the medical knowledge of Medieval Europe. Our knowledge of Greek medicine
mainly comes from the Hippocratic writings and from Galen writing in the second
century CE.
The earliest Greek medicine was
based on religion. Asclepius, the son of Apollo, was able to cure disease and
patients sleeping at his shrines would see the God in their dreams and receive
advice on appropriate treatments. Around the sixth century BCE Greek medicine
began to change with a greater emphasis on rational explanations of disease
involving natural rather than supernatural causes. The Hippocratic writings,
probably written by a number of authors, suggested liquids were the vital
element in all living things. The human body contained four fluids or humors,
phlegm, yellow bile, black bile and blood. Disease was caused by an imbalance
of these fluids in the body. Such an imbalance could be caused by the weather
or by extreme behaviour such as over eating or excessive drinking. The medical
practice of bleeding, which was to persist for several thousand years,
originated from the belief there was an excess of blood which could be cured by
releasing some blood from the body. Correct diet, bathing, exercise, sleep and
sex would prevent illness. According to Hippocrates sex should be more frequent
in winter and older men should have sex more frequently than younger men. He
considered epilepsy was caused by an excess of phlegm. Hippocrates however
tells us little about infectious diseases and anatomy as the dissection of
bodies was taboo as it was considered to be a violation of the sanctity of the
human body.
The classical era taboo on human
dissection led to some quite erroneous views of the human body. Aristotle
considered the heart was where the soul was located and was the center of
thought, sense perception and controlled bodily movements. He considered the
brain cooled the heart and the blood. There was however a brief period in
Alexandria where due to the ancient Egyptian practice of embalming and the more
recent Platonic view that the soul and not the body, was sacred, human
dissection was allowed. Herophilus and Erasistratus carried out dissections
that led them to discover the nerves leading to the brain. They discovered
there were two different types of nerves, one, dealing with sense perception
and the other with body movement. When studying the brain, they discovered the
cerebrum and the cerebellum and suggested the heavily folded human brain
indicated humans� higher intelligence compared to animals. They considered the
lungs took in air that was then transferred to the arteries, the veins held
blood and the heart worked like a bellows. After making significant discoveries
that could only be made by human dissection, the taboo against dissection rose
again delaying further progress until the 16th century. Until then, knowledge
of the interior of the human body could only be guessed at from its external
behaviour or by comparison with animal anatomy.
Two further theories created by
the ancient Greeks were the methodic theory and the pneumatic theory. The
methodic theory considered disease to be caused by a disturbance of atoms in
the body and treatment involved manipulating the body by massage, bathing or
exercise. The pneumatic theory considered breath to be a crucial factor in
human health.
The high point of Greco-Roman
medical knowledge came with Galen in the second century CE. Galen�s two main
areas of study were anatomy and physiology. As human dissection was illegal his
anatomical studies were based on dissections of animals, particularly the
Barbary ape. He did however have the assistance of his study of gladiator�s
wounds, a human skeleton he had seen in Alexandria and of human bodies exhumed
by natural events, such as floods. Galen�s work on the bone structure and
muscular system were a significant advance on anything else in antiquity. His
belief in Aristotle�s idea that everything had a purpose led him to assume
every bone, muscle and organ had a particular function and he set out to
describe each bone, muscle and organ and their particular function. He
described the human skeleton and muscular system with some accuracy. He put an
end to Aristotle�s idea that the mind was located in the heart, locating it in
the brain. Galen discovered seven pairs of cranial nerves, the sympathetic
nervous system and he distinguished between the sensory and motor nerves.
However, he also found things that did not exist. The rete mirabile (wonderful
network) is located under the brain of many hoofed animals but is not found in
humans. Yet Galen�s claim that it exists in humans was accepted for some
thirteen centuries.
Galen�s physiology, his concept
of how the human body worked, began with a vital spirit, pneuma taken into the
body by breathing. The pneuma entered the lungs where it met some blood before
passing into the left ventricle of the heart. The blood then flowed into the
arteries and spread through the body feeding the flesh. When food entered the
body it converted into blood in the liver, some of the blood then entered the
veins and spread through the body and was feed into the flesh. Other blood
flowed from the liver into the right ventricle of the heart from where some of
the blood entered the lungs to absorb the pneuma. Some of the blood in the
right ventricle however passed directly into the left ventricle and from there
flowed into the arteries. One problem for Galen, was that he was unable to
discover how blood moved from the right ventricle to the left ventricle, which
were divided by a solid muscular wall. He eventually concluded there must be
tiny holes in the wall, so small they could not be seen by the human eye.
Galen�s system correctly realized the heart caused blood to flow through the
body and that the arteries contained blood. Previously Erasistratus suggested
the arteries only contained air, as the arteries of a dead body do not contain
blood. Galen did not realize that the blood circulated and his suggestion of
minute holes in the wall between the right and left ventricles of the heart was
wrong.
 b
b
Galen�s pathology, his concept of
illness, brought together Hippocrates theory of the four humors and Aristotle�s
idea of the four elements, air, fire, earth and water. Blood was considered to
be warm and moist, yellow bile warm and dry, black bile cold and dry and phlegm
cold and moist. Blood is associated with the heart, yellow bile with the liver,
black bile with the spleen and phlegm with the brain. The following table shows
how Galen brought the two ideas together.
|
Humor
|
Element
|
Organ
|
Qualities
|
|
Phlegm
|
Water
|
Brain
|
Cold &
Wet
|
|
Blood
|
Air
|
Heart
|
Hot &
Wet
|
|
Yellow bile
|
Fire
|
Liver
|
Hot &
Dry
|
|
Black bile
|
Earth
|
Spleen
|
Dry & Cold
|
The table indicates the symptoms
of the disease, the cause of the disease and the cure for the disease. If the
patient has the symptom of being hot and perspiring, this is the quality of
being hot and wet; this suggests there is an imbalance in the blood, so that
bleeding is the cure. If they have a hot and dry fever, this suggests the
yellow bile is out of balance, so that vomiting up the yellow bile is the cure.
The humors could also affect a person�s personality. An excess of phlegm would
make one phlegmatic, of blood, one would be sanguine, of yellow bile, one would
be choleric and of black bile, one would be melancholic.
An imbalance in the humors in
particular organs could result in illness. Excessive phlegm in the bowels
resulted in dysentery and an excess in the lungs caused tuberculosis. Cancer
was caused by a massive imbalance in the humors. Stroke was caused by an excess
of blood, jaundice by excessive yellow bile and depression by too much black
bile.
(back
to content)
1.2.10.1 Asahi Health w
Asahi (or Asahi Health) is a
Finnish health exercise based on the eastern traditions of T'ai chi
ch'uan, qigong, yiquan and yoga,
with a western scientific viewpoint. Asahi is designed to suit everybody,
regardless of physical condition or age.
Asahi exercise is taught and
performed in instructed groups, but Asahi can also be performed alone as a form
of daily self-treatment. Asahi exercise is ideal for short breaks. This
exercise is equally effective in a group or alone.
The History of Asahi
Asahi was created in Finland 2004
by professional sports instructors and martial artists Timo Klemola, Ilpo
Jalamo, Keijo Mikkonen and Yrj� M�h�nen. They all had high regards towards
classical body development techniques such as karate, T'ai chi ch'uan, yiquan
and yoga, but these styles, as rewarding as they are, seemed to attract only a
small marginal of the Finnish population.
These classical styles are quite
complex and therefore may have a high starting level. They use concepts such as
qi and prana, which may seem mystical to western people.
The purpose of Asahi was to get
the best out of these techniques, put it in the most simplified form, make it
overall scientific and turn it into an easily approachable form - a health
exercise for everybody with no starting level at all.
Asahi is designed to treat and
prevent shoulder- and back problems, fractures due to falling down and
stress-related psychosomatic problems.
Asahi is a series of slow
movements, completed in silence. It looks harmonious and beautiful, a bit like
qigong.
The basic six principles of Asahi
are:
1. The linking of movement and
breath
2. Practicing vertically erect
body alignment
3. Whole body movement
4. Listening to the slow motion
5. Cultivating the mind with
mental images
6. The exercise as a continual,
flowing experience The Asahi movements are soft and performed in the rhythm of
breathing. The series is simple and easy to learn. The movements have also a
practical function, for example picking up a ball from the floor or improving
one�s balance by standing on one foot. Advanced levels are designed for
long-term trainees, yet they are equally simple to learn.
The Principles of Asahi Distribution
Asahi can be practiced in major
areas of Finland. Asahi Health Ltd has also been accepted as an Education
Partner to Federation of International Sports, Aerobics and Fitness as the
first Body Mind -product to be recognized and recommended by this organization.
These exercises can be help my a teacher guiding a class, or through video instruction.
Others that have experience can practice their own routine after learning from
instruction.
(back
to content)
1.2.10.2 Biodanza w
Biodanza (a neologism jointed the
Greek bio [life] and the Spanish danza, literally "the dance of
life") is a system of self-development utilizing music, movement and
positive feelings to deepen self-awareness. It seeks to promote the ability to
make a holistic link to oneself and one's emotions and to express them.
Practitioners believe that Biodanza opens the space for one to deepen the bonds
with others and nature and to express those feelings in a congenial manner.
It was created in the 1960s by
the Chilean anthropologist and psychologist Rolando Toro Araneda. The Biodanza
system is now found in 54 countries, including Argentina, Belgium, Brazil,
Chile, Colombia, Czech Republic, Ecuador, France, Germany, Israel, India,
Italy, Netherlands, New Zealand, Norway, Portugal, Spain, Switzerland, United
Kingdom, Uruguay, Venezuela, Australia, Japan, South Africa, United States,
Ireland and Russia. Practitioners describe Biodanza as a "human
integration system of organic renewal, of affective re-education, and of
relearning of Life's original functions. Its application consists in leading
vivencias through music, singing, movements and group encounter
situations". Proponents claim it can be used to develop our human
capacities, communication skills, and relationships, including the feeling of
happiness.
Origins and popularity
Purpose and process
Biodanza has been featured on CNN
Chile, on BBC TV and national newspapers in the UK, and in lifestyle magazines
in the UK and South Africa.
The Daily Telegraph describes
Biodanza as "a series of exercises and moves that aim to promote
self-esteem, the joy of life and the expression of emotions. Lots of bounding
around and hugs".
Following the death of its
founder in February 2010, two governing bodies of Biodanza currently exist, by
means of which students may receive official certificates. The International Biodanza
Federation (IBF) governs the Biodanza system in Europe, Australia, New Zealand,
the United States and Canada. The US has official schools located in San
Francisco, Los Angeles and Maryland. The International Organization of Biodanza
SRT governs the Biodanza system in South America.
1.2.10.3 Speleotherapy w
Speleotherapy (Greek
σπήλαιον spḗlaion
"cave") is an alternative medicine respiratory therapy involving
breathing inside a cave.
Speleotherapy
History
Hippocrates believed that
salt-based therapies, including inhaling steam from saltwater, provided relief
of respiratory symptoms. There are claims of improvements in the breathing of
miners in Roman times and medieval times. Speleotherapy hospitals existed in
Italy in the 19th century. In the middle of the 19th century, a clinic, founded
in Mammoth Cave (Kentucky, USA), was intended for tuberculosis patients.
However, a few months after the death of five of the patients, the hospital was
closed.
The history of modern
speleotherapy dates back to the 1950s. At this time, speleotherapeutic
hospitals arose in several Eastern and Central European countries.
Residents of Ennepetal in Germany
used the Kluterth�hle cave as a bomb shelter during WW2.
Karl Hermann Spannagel began
researching the therapeutic effect of caves.
Speleotherapeutic facilities in
karst caves were started in Hungary and Czechoslovakia.
In 1968, in Solotvyn (now in
Ukraine), the first speleotherapy clinic was opened on the territory of the
USSR. In 1982, a climate chamber was patented, equipped with a salt
filter-saturator to recreate the conditions of salt mines on the earth's
surface.
Indications
The treatment is claimed to be used for bronchial asthma, bronchitis,
allergic and chronic runny nose, allergic and chronic sinus diseases, various
allergies and skin diseases, fibrosing alveolitis and croup. However, as of
2022, there is no evidence to support these claims.
Speleotherapy in the Czech Republic
The first speleotherapy in the Czechoslovakia was carried out by Mgr. �tefan
Roda in Slovakia in the Tomba�ek Cave in the High Tatras (1969). In 1973-1976,
doctors Timov� and Valtrov� from the Children's Clinic in Bansk� Bystrica
treated childhood asthmatics with speleotherapy with favourable results, which
were published in the medical literature. From 1981 to 1985, speleotherapy
became the subject of official scientific research tasks, carried out under the
responsibility of the Ministry of Health and the Geographical Institute of the
Czechoslovak Academy of Sciences. In 1985, speleotherapy was recognized as an
official climatic treatment method.
According to the chairman of the
International Union of Speleology's Standing Commission on Speleotherapy, Prof.
Svetozar Dluholucky, M.D., speleotherapy is "a natural way of treating
asthma and allergies, which it would be a sin not to use." He has
conducted research in Bystrianska Cave since 1974, according to which there has
been a fivefold decrease in respiratory diseases and asthma in the children
studied. In 1997, he conducted further research on 111 asthmatic children with
the same results.
Allergists and immunologists
remain sceptical, however.
There are two speleotherapy
centres in the Czech Republic: the Children's Treatment Centre in Ostrov u
Macochy and the Children's Treatment Centre for Respiratory Diseases in Zlat�
Hory. The children's sanatorium in Mladč-Vojtěchov was closed in
2014.
Research
Hoyrm�r Malota led a research team that tested patients of the
speleotherapeutic sanatorium in Mladeč in 1985-1987 and came to the
clinically verified knowledge "that individual factors of the underground
environment, or their complex connected by internal and external interactions,
stimulate and modulate the immune system of the human organism directly. He
confirmed that repeated exposure to the underground environment - without the
use of anti-asthmatic, antihistamine, or immunomodulatory pharmaceutical
preparations - induces positive and measurable changes in secretory and
lymphatic lysosomes and immunoglobins after only a few days of exposure to the
degree that any existing artificial immunomodulators cannot achieve."
Some factors characterizing cave endoclimates are controversial. While
cave aerosols may theoretically contain high Ca and Mg ions, in practice, they
are not present in the treatment sites known to date; Ca and Mg concentrations
are everywhere the same as in the ambient air. It has been shown that the
concentrations of Ca and Mg in cave air are not so significantly elevated as to
be considered a therapeutic factor.
The elevated CO2 concentration, or the absence of allergens in the cave
(the presence of some molds in very small amounts), or the absence of ozone is
also questionable.
According to the Cochrane Collaboration, three studies involving 124
children with asthma met the inclusion criteria for the 2001 meta-study. Still,
only one study was of adequate methodological quality. Two studies reported
that speleotherapy had a beneficial short-term effect on lung function. The
other results could not be reliably evaluated. Due to the small number of
studies, no reliable conclusion can be drawn from the available evidence on
whether speleotherapy interventions are effective in treating chronic asthma.
Randomized controlled trials with long-term follow-up are needed.
No evidence of the effectiveness of speleotherapy was found from
randomized controlled trials and further research is needed.
According to a 2017 Romanian systematic review, speleotherapy is a
valuable treatment method for asthma and other respiratory problems. Still,
only a few studies can be found in international databases, reflecting the
specificity of this field. On the other hand, basic studies in laboratory
animals and in vitro cell cultures have demonstrated the efficacy and
usefulness of speleotherapy.
Quote
There are not so many karst
caves, so salt mines have been used for treatment for a long time. So
sanatoriums were created there, and it's called halotherapy. Wieliczka in
Poland is very well known. Later on, there was an attempt to make halocaves
artificially and they built a kind of igloo out of the salt that was mined. In
various studies in the mid-1980s they compared the effect underground and in
these salt chambers placed outside. It turned out that the above-ground salt
caves had virtually no effect. And even, very easily contaminated with
microbes, it can be dangerous. Many of the bacteria that causes severe
respiratory infections love salt and settle in the surface layers of salt
walls. Even salt mines that operate underground have very strict criteria to
ensure that people do not contaminate the salt chamber with germs. Even in
some, every three to four months, they grind off a few millimeters of the wall
because of the bacilli. When their use was abandoned, it was quiet for about
five years, and it started again. If it's not kept clean, it can be detrimental
to health; some types of pneumococcus also stick in there. In our case, they
tried to mitigate this by putting in air conditioning systems. But an
artificial salt cave system that is fully air-conditioned cannot work. That's
about like trying to replicate the Tatra air in a seventh-floor apartment
block, it's stupid.
� Prof. MUDr. Svetoz�r DLUHOLUCK�, CSc���������������������������������������������������������
(back to content)
1.2.10.1 Dark Ages f
The fall of the Roman Empire
marked the beginning of the Dark Ages in Europe. The later stages of the Roman
Empire were a period of epidemic disease and population decline. The population
of cities in particular was to fall and the cities paved roads, drains, aqueducts
and public baths soon fell into disrepair. The decline of the cities was
accompanied by a decline in classical learning which was opposed by the new
Christian church. In 391 CE a Christian mob set fire to the great library of
Alexandria and murdered the pagan philosopher Hypathia. The last pagan school
of learning, the academy in Athens was closed in 529 CE by order of the Emperor
Justinian.
Medicine was not to escape the
general decline of learning which accompanied the fall of the Roman Empire and
the arrival of Christianity. There was a return to the belief that the cause of
much illness was supernatural. Illness was a punishment from God for people�s
sins. The curing of such disease by medical practices was contrary to Gods
will. The only appropriate treatment was prayer and penitence. Diseases might
also be caused by witchcraft, possession by demons or spells made by elves and
pixies. Some of the old learning did survive, ironically in Christian
monasteries where monks copied and translated classical writings. Their work
mixed superstition and religion with classical learning and knowledge. Bede,
(born 673 CE) an English monk famous for his Ecclesiastical History of the
English People and one of the most learned men of the Dark Ages, also wrote on
medical matters. He referred to Hippocrates and the theory of the four humors
and prescribed bleeding as the appropriate treatment for hot fevers caused, as
he believed by an excess of blood. But he also considered magic incantations
and the wearing of magic amulets as the way to deal with spells made by pixies.
There are also stories of miraculous cures such as a leper sleeping where a
saint died and being cured when waking the next morning.
 b
b
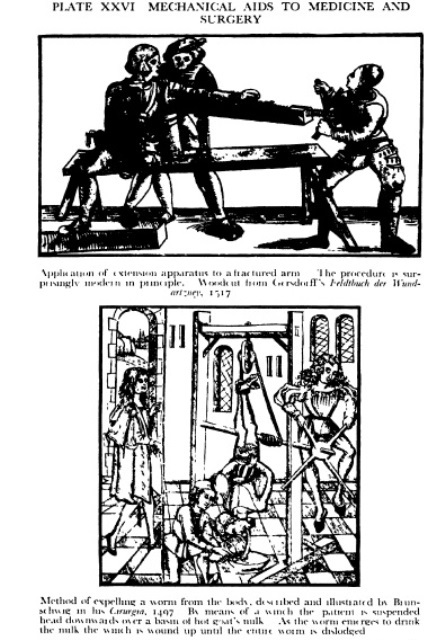 b
b
�
Not much had changed by the 12th
century CE when Hildegard of Bingen began to bring together classical medical
beliefs with 12th century religious beliefs. She considered the imbalance of
the four humors resulted from mans ejection from the Garden of Eden. The eating
of the forbidden fruit destroyed the balance of the four humors in the human
body. Sin was to cause the imbalance of the humors and was therefore the cause
of disease. Some of her medical beliefs could not be regarded as scientific or
rational. Her cure for jaundice was to tie a live bat, first to the patient�s
back and then to the patient�s stomach. Failing eyesight, caused by excessive
lust, was to be cured by placing the skin of a fish�s bladder over the patients
eyes when he goes to sleep, but it had to be taken off by midnight.
(back
to content)
1.2.10.2
Arab medicine w
The Moslem prophet Mohammed was
born in 570 CE and he and his successors were to conquer an empire extending
from Spain to India. The early Moslems had a tolerant attitude to Christian and
Jewish minorities who were allowed to freely practice their religions. The
origins of Arabian medicine lay with a heretical Christian sect known as the
Nestorians. The Nestorians under threat of persecution from orthodox Christians
fled eastwards toward present day Iraq and Iran. They brought with them
classical texts from a range of authors including Hippocrates, Aristotle and Galen
which they proceeded to translate into Arabic. At this time the Arab world had
a positive attitude to new ideas and was happy to adopt the ideas of classical
scholars like Aristotle and Galen.
The first great Arab medical
authority was Rhazes who was born in 854 CE. Rhazes believed illness had
nothing to do with evil spirits or God and that classical authorities were not
above criticism. He was in frequent disagreement with Galen. He considered
Galen�s cure for asthma consisting of a mixture of owl�s blood and wine did not
work as he had tried it and found it to be useless. He questioned the belief
that disease could be diagnosed by studying the patient�s urine and was the
first medical authority to understand the difference between measles and
smallpox. Rhazes gave a full description of diseases he encountered giving his
diagnosis, prognosis and treatment. His understanding of the workings of the
human body were however, hindered by the Islamic prohibition on dissections of
the human body. Arabian medicine�s second great authority was Avicenna
(980-1037) whose book the Cannon of Medicine was to become the leading medical
work in both Europe and the Middle East for some 600 years. Avicenna�s Cannon
includes many of the ideas of Hippocrates, Aristotle and Galen but also
includes many of Avicenna�s own ideas. The Cannon deals with a range of
diseases and describes their diagnosis, prognosis and treatment.� Avicenna accepted Hippocrates and Galen�s
theory of the four humors. Treatments included bleeding, enemas and purges
while diagnosis included examining the pulse and urine. Over 700 drugs were
recognized by Avicenna and the Cannon provided instructions on how they were to
be prepared, which drugs should be used for which illness and their effects.
Wounds were dealt with by cauterizing, a treatment that dates back to Ancient
Egypt.
Surgery in the Arab world was not
respected and surgeons were usually craftsmen. One exception to this is
Albucasis (936-1013) who practiced in Cordoba in southern Spain. Albucasis
wrote a book called Tasrif or the Collection which provided full accounts of surgery
practiced at the time. The Collection was to become the standard book on
surgery during medieval times. The book prescribes a range of surgical
procedures including trepanning, dentistry, mastectomy and lithotomy and
advocates cauterization as a treatment for a wide range of problems.
�
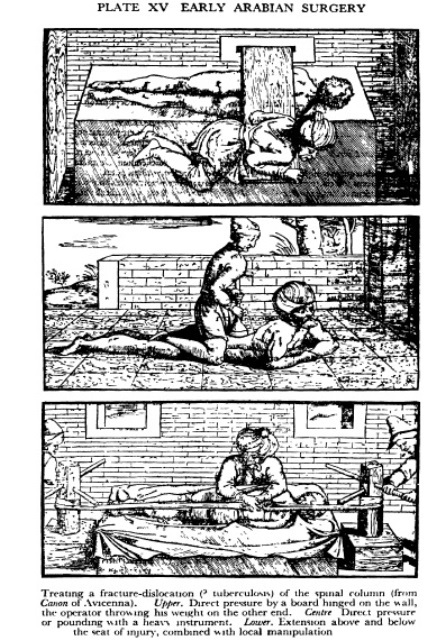 b
b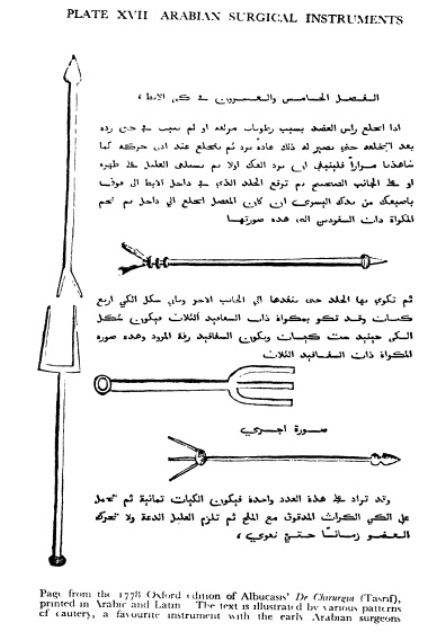 b
b
(back
to content)
1.2.10.2.1
Unani medicine w
Unani or Yunani medicine (Urdu: طب یونانی
tibb yūnānī) is Perso-Arabic traditional medicine as practiced
in Muslim culture in South Asia and modern day Central Asia. Unani medicine is
pseudoscientific. The Indian Medical Association describes Unani practitioners
who claim to practice medicine as quacks.
�
Birbahuti (Trombidium red velvet mite) is used as Unani
Medicine
The term Yūnānī
means "Greek", as the Perso-Arabic system of medicine was based on
the teachings of the Greek physicians Hippocrates and Galen.
The Hellenistic origin of Unani
medicine is still visible in its being based on the classical four humours:
phlegm (balgham), blood (dam), yellow bile (ṣafrā) and black bile
(saudā'), but it has also been influenced by Indian and Chinese
traditional systems.
History
Arab and Persian elaborations
upon the Greek system of medicine by figures like Ibn Sina and al- Razi
influenced the early development of Unani.
Unani medicine interacted with
Indian Buddhist medicine at the time of Alaxander's invasion of India. There
was a great exchange of knowledge at that time which is visible from the
similarity of the basic conceptual frames of the two systems. The medical
tradition of medieval Islam was introduced to India by the 12th century with
the establishment of the Delhi Sultanate and it took its own course of
development during the Mughal Empire, influenced by Indian medical teachings of
Sushruta and Charaka. Alauddin Khalji (d. 1316) had several eminent physicians
(Hakims) at his royal courts. This royal patronage led to the development of
Unani in India, and also the creation of Unani literature.
Education and recognition
There are several Indian universities
devoted to Unani medicine, in addition to universities that teach traditional
Indian medical practices in general. Undergraduate degrees awarded for
completing an Unani program include the Bachelor of Unani Medicine and Surgery,
Bachelor of Unani Tib and Surgery, and Bachelor of Unani Medicine with Modern
Medicine and Surgery degrees. A small number of universities offer
post-graduate degrees in Unani medicine.
The Central Council of Indian
Medicine (CCIM), a statutory body established in 1971 under the Department of
Ayurveda, Yoga and Naturopathy, Unani, Siddha and Homoeopathy (AYUSH), monitors
higher education in areas of Indian medicine including Ayurveda, Unani, and other
traditional medical systems. Another subdivision of AYUSH, the Central Council
for Research in Unani Medicine (CCRUM), aids and co-ordinates scientific
research in the Unani system of medicine through a network of 22 nationwide research
institutes and units.
To fight biopiracy and unethical
patents, the Government of India set up the Traditional Knowledge Digital
Library in 2001 as repository of formulations used in Indian traditional
medicine, including 98,700 Unani formulations.
In 1990, the total number of
hakims or tabibs (practitioners of Unani medecine) in Pakistan was 51,883. The
government of Pakistan's National Council for Tibb (NCT) is responsible for
developing the curriculum of Unani courses and registering practitioners of the
medicine.
Various private foundations
devote themselves to the research and production of Unani medicines, including
the Hamdard Foundation, which also runs an Unani research institution
The Qarshi Foundation runs a
similar institution, Qarshi University. The programs are accredited by Higher
Education Commission, Pakistan Medical and Dental Council, and the Pakistan
Pharmacy Council.
Critism and safety issues
Some medicines traditionally used
by Unani practitioners are known to be poisonous.
The Indian Journal of
Pharmacology notes:
According to WHO,
"Pharmacovigilance activities are done to monitor detection, assessment,
understanding and prevention of any obnoxious adverse reactions to drugs at
therapeutic concentration that is used or is intended to be used to modify or
explore physiological system or pathological states for the benefit of recipient."
These drugs may be any substance
or product including herbs, minerals, etc. for animals and human beings and can
even be that prescribed by practitioners of Unani or Ayurvedic system of
medicine. In recent days, awareness has been created related to safety and
adverse drug reaction monitoring of herbal drugs including Unani drugs.
(back
to content)
1.2.10.3.1 Medieval European medicine w
European medicine began to move
away from the supernatural explanations of disease with the founding of a
medical school at Salerno. The school was probably founded in the ninth century
and reached its greatest heights between the tenth and thirteenth centuries.
Anatomy was taught at Salerno based on the dissection of pigs whose internal
organs were thought to be similar to those of humans. Passionarius, a book
written by Gariopontus, one of the teachers at the school, was based upon
classical Greek learning while the arrival in Salerno of Constantine the
African around 1075 with many Arab medical works was to greatly improve the
medical knowledge at Salerno and eventually all Europe. Constantine was to
spend the remainder of his life translating the Arabic texts into Latin and so
bring the classical Greek authors, upon whose work Arabic medicine was based,
to Europe.
The translation of Arabic medical
texts into Latin continued in early medieval times so that the works of
Hippocrates, Aristotle, Galen, Rhazes, Avicenna and Albucasis became well
known. They soon assumed a status of great authority and their initial impact
was to help free medicine from supernatural and magical explanations and cures.
Their status however was eventually to hold back the improvement of European
medicine as new ideas contrary to those of the Greek and Arab writers had great
difficulty in obtaining acceptance.
New medical schools at
Montpellier, Bologna, Paris and Padua were founded that significantly increased
medical knowledge.� The knowledge of
anatomy improved with the occasional human dissection being performed as
post-mortem examinations for judicial purposes and with occasional dissections
of the bodies of executed criminals. Anatomy was also improved by Mondino de
Luzzi or Mundinus who taught at Bologna. His book Anothomia brought a new level
of knowledge of anatomy, although he did repeat many of the errors of Galen.
Mundinus however did most of his dissections himself, unlike other teachers who
sat on a high chair somewhat above the body reading a book supposedly
describing the dissection, but probably only loosely related to it. Guy de
Chaulias, the leading surgeon of the 14th century was a pupil of Mundinus.
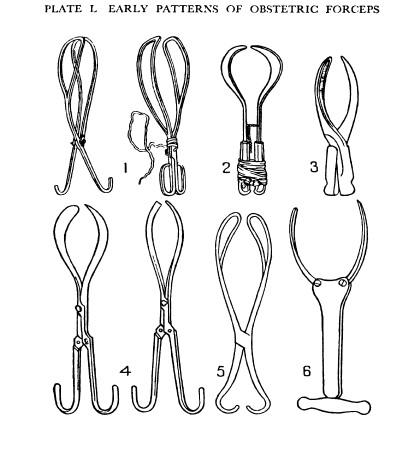
 b
b
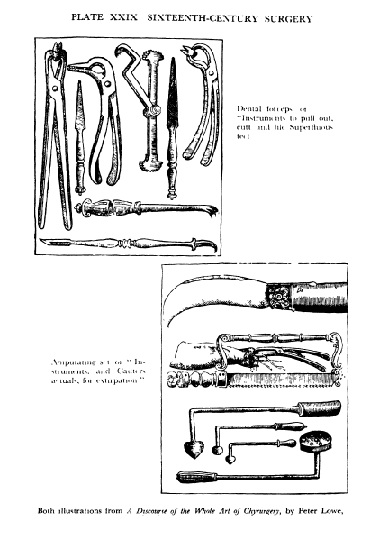 b
b

 b
b
The most dramatic medical event
of the 14th century in Europe was the arrival of the Black Death. It originated
in China killing up to two thirds of the population and then spread along trade
routes to Europe and the Arab world. It killed half the population of Cairo and
between a quarter and a third of the population of Europe. The medical
authorities in Europe had no solution to the Black Death. The idea of a
contagious disease was beyond the understanding of medical knowledge in either
the Arab or European world during the 14th century. The Arabs considered the
Black Death was caused by evil spirits; the Europeans blamed everything from
the Jews to Gods punishment for human�s sins. Jews were accused of poisoning
wells and entire Jewish communities were wiped out by vengeful Christians.
Flagellants travelled around Europe whipping themselves for their sins hoping
this would appease God. Conventional medicine of the time had no answers;
bleeding, cauterizing and cleaning the air with incense were all tried and
failed. Quarantining worked to some extent but the best advice was to run like
the wind. The failure of conventional medicine during the Black Death led to a
revival of supernatural explanations of disease.
(back
to content)
1.2.10.3.2
Traditional Mongolian medicine w
Traditional Mongolian medicine
developed over many years among the Mongolian people. Mongolian medical
practice spread across their empire and became an ingrained part of many other
people's medical systems.
History
The Mongols were part of a wider
network of Eurasian people who had developed a medical system of their own,
including the Chinese, Korean, Tibetan, Indian, Uighur, Islamic, and Nestorian
Christians. They took the medical knowledge of these people, adapted it to
develop their own medical system and at the same time organized an exchange of
knowledge between the different people in their empire. On their journeys
throughout Asia, the Mongols brought with them a team of doctors. Usually
foreign, these doctors themselves had brought medical knowledge from other
people in Asia to the Mongol court. They serve three purposes on the journeys
on which the accompanied Mongol princes. Their first purpose was to be the
personal physicians of the princes in case they required medical attention. The
second was to observe and obtain any new medical knowledge from the various
groups of people that they encounter.
Finally, they were to also spread
the medical knowledge that the Mongols had put together to the peoples they
encountered. The Mongols were also able to contribute new or more advanced
knowledge on topics such as bone setting and treatments of war wounds because
of their nomadic lifestyle. The Mongols were the first people to establish a
link between diet and health.
Traditional Mongolian doctors
were known as shaman, or holy men. They relied on magic and spiritual powers to
cure illness. They were called on to determine whether the illness was caused
by natural means or because of malicious wishes. Though they were often used as
healers, their main strength was in prophecy readings. Foreign physicians who
used herbs to treat illness were distinguished from the shamans by their name,
otochi, which meant herb user or physician. It was borrowed from the Uighur
word for physician, which was otachi. When Mongolian medicine began to
transition to using herbs and other drugs and had the service of foreign
doctors, the importance of shamans as medical healers began to decline.
Hu Sihui (1314�1330) was a Mongol
court therapist and dietitian during Mongol Yuan Dynasty reign in China. He is
known for his book Yinshan Zhengyao (Important Principles of Food and Drink),
that became a classic in Chinese medicine and Chinese cuisine. He was the first
to empirically discover and clearly describe deficiency diseases.
Treatment practices
Animal blood
Animal blood was used to treat a
variety of illness, from gout to blood loss. Recorded in the Yuan Shih, are
many incidents where the blood of a freshly killed animal, usually a cow or an
ox, was used to treat illness. Gout, which was a common affliction of the
Mongol people, was treated by immersing the afflicted body part into the belly
of a freshly killed cow. Placing a person in the stomach of an animal was also
used as a method of blood transfusion. On the battlefield, when a soldier
became unconscious due to massive amount of blood loss, he would be stripped
and placed into the stomach of a freshly killed animal until he became
conscious again. In less severe cases, the skin of a freshly killed ox was
combined with the masticated grass found in a cow's stomach to form a sort of
bandage and ointment to heal battle wounds. It was believed that the stomach
and fat of the freshly killed animal could absorb the bad blood and restore the
wounded to health.
Minerals
Mongolian medical literature
mentions the use of minerals in medicine, usually in the form of powdered
metals or stones. From the Chinese, Mongolians also used cinnabar or mercury
sulfide as treatment options, despite the high number of casualties it caused.
Both the Chinese and the Mongols believed that cinnabar and mercury sulfide
were the elixir of life.
Herbs
Herbs were the mainstay of
Mongolian medicine; legend had it that any plant could be used as a medicine.
An emchi is quoted as saying:
All those flowers, on which
butterflies sit, are ready medicine for various diseases. One can eat such
flowers without any hesitation. A flower rejected by the butterflies is
poisonous, but it can become medicine, when it is properly composed.
Acupuncture and moxibustion
The Mongolian adopted the
practice of acupuncture from the Chinese. They adapted this tradition and made
it a Mongolian form of treatment when they burned herbs over the various
meridian points rather than used a needle. The tradition of Moxibustion
(burning mugwort over acupuncture points) was developed in Mongolia and later
incorporated into Tibetan medicine.
Water
One unusual aspect of Mongolian
medicine is the use of water as a medicine. Water was collected from any
source, including the sea, and stored for many years until ready for use.
Acidity and other stomach upsets were said to be amenable to water treatments.
Bone setting
Bone setting is a branch of
Mongolian medicine carried out by Bariachis, specialist bone setters.
They work without medicines, as
anesthetics or instruments. Instead they rely on physiotherapy to manipulate
bones back to their proper position. This was done without any pain to the
patient.
Bariachis are laypeople, without
medical training, and are born into the job, following the family tradition.
They had the ability to fix any bone problem, no matter how severe or difficult.
When
Chinese physicians were brought
into the Mongolian empire, Wei Yilin, a famous Yuan orthopedic surgeon
established particular methods for setting fractures and treating shoulder,
hip, and knee dislocations. He also pioneered the suspension method for joint
reduction. He was not only an orthopedic surgeon but also an anesthesiologist
who used various folk medicine for anesthetics during his operations. It
appears that this traditional practice is in decline, and that no scientific
research has been carried out into it.
Pulse diagnosis
Pulse diagnosis is very popular
in Western Asia and especially Iran, and its introduction to the Islamic West
can be traced back to the Mongols. The Mongol word for pulse, mai, has Chinese
etymology. In China, pulse diagnosis was related to the balance between the yin
and yang.
Irregular pulses were believed to
be caused by an imbalance of the yin and the yang. However, when the Mongol
adopted this medical practice, they believed that the pulse was directly
related to moral order and that when the moral order was chaotic, so the pulse
would be chaotic and irregular as well. This belief is highlighted in a story
recounted in the Yuan Shih. In 1214, Ogodei Qa'an had an irregular pulse, and
was very ill. His most trusted physician ordered that a general amnesty be
declared all across the empire. Shortly afterwards, Ogodei Qa'an was restored
to health and his pulse regular once again. For the Mongol, this account gives
evidence to the direct relationship between pulse and moral order. Pulse
diagnosis soon became the primary diagnosis' tool and became the cornerstone of
Mongolian medicine. Qubilai decreed that Chinese manuals on pulse-based
medicine be translated to Mongolian. His successor, Tem�r, in 1305, ordered
that pulse diagnosis be one of the ten compulsory subjects in which Imperial
Academy of Medicine medical students be tested. In pulse diagnosis, there was a
distinction between measuring a child's pulse versus and adult's pulse, and
this distinction was greatly emphasized in the Chinese texts that were
translated, and later in the Mongolian texts.
Discovery of the link between
diet and health
In 1330, Hu Sihui, a Mongolian
physician published Yinshan Zhengyo (Important Principles of Food and Drink).
It was the first book of its kind. In this textbook, Hu Sihui preached the
importance of a balanced diet with a focus on moderation, especially in
drinking. He also listed beneficial properties of various common foods,
including fish, shellfish, meat, fruit, vegetables, and 230 cereals. Grapes
were recommended for character strengthening and boosting one's energy levels.
However, eating too many apples could cause distension and indulging in too
many oranges lead to liver damage. A common menu item, dog meat, was very beneficial
because it calmed the liver, spleen, heart, lungs, kidneys, and pericardium.
This link between diet and health was spread far and wide by the Mongols on
their journeys across the Eurasian steppe lands.
Dom
Dom is the tradition of household
cures, many based simply on superstition � one instance being that a picture of
a fox hung over a child's bed will help it sleep. Counting the frequency of
breathing is also stated to be a relief for psychological problems and
distress.
The practise apparently was part
of lamaist popular medicine.
Eating papers
Strip of Mongolian eating papers
with Tibetan (left) and Mongolian (right) text Traditional Mongolian medicine
today
A printing stock found in eastern
Mongolia in the 1920s documents a historical custom of eating a piece of paper
with words printed on it, in order to prevent or heal maladies. On fields of
about 24x29 mm magical incantations in Tibetan are printed, along with use
instructions in Mongolian.
Traditional Mongolain Medicine
Today
Today Mongolia is one of the few
countries which officially supports its traditional system of medicine.
Since 1949, the Chinese
government has steadily promoted advances in Mongolian medical care, research
and education. In 1958 the Department of Traditional Chinese and Mongolian
Medicine at the Inner Mongolia Medical College opened its doors to students. In
2007 it expanded, opening a state of the art campus just outside Hohhot City.
The Chinese government has also established scores of Mongolian medicine
hospitals since 1999, including 41 in Inner Mongolia, 3 in Xinjiang, and 1 each
in Liaoning, Heilongjiang, Gansu and Qinghai.
Coding (therapy)
Coding (also known as the
Dovzhenko method) is a catch-all term for various Russian and post-Soviet
alternative therapeutic methods used to treat addictions, in which the
therapist attempts to scare patients into abstinence from a substance they are
addicted to by convincing them that they will be harmed or killed if they use
it again. Each method involves the therapist pretending to insert a
"code" into patients' brains that will ostensibly provoke a strong
adverse reaction should it come into contact with the addictive substance. The
methods use a combination of theatrics, hypnosis, placebos, and drugs with
temporary adverse effects to instill the erroneous beliefs. Therapists may
pretend to "code" patients for a fixed length of time, such as five
years.
Coding was created by Aleksandr
Dovzhenko, a Soviet psychiatrist.
In the case of alcohol addiction,
the procedure may be carried out with a drug that temporarily affects the
respiratory system when mixed with alcohol, administered under hypnosis. The
therapist gives patients the drug, then allows them a small amount of alcohol,
which triggers an adverse reaction and makes them erroneously believe that the
therapy has had a long-term effect. Another method involves the therapist
giving patients hypnotic suggestions during a head massage, with the message
that alcohol will cause blindness or paralysis.
In one method, the therapist
numbs patients' mouths with local anaesthetic, then places electrodes with a
very weak current into their mouths. This is to make patients believe that the
"nerve points" in their mouth are being "manipulated" and
that it is no longer safe for them to drink alcohol. A further method involves
the therapist using a special helmet to persuade patients that the therapist's
suggestions are controlling their minds. Typically, therapists will also make
patients sign a disclaimer, supposedly absolving the therapist of any
responsibility should the patient use the addictive substance and suffer ill
effects or die.
(back
to content)
1.3.0 The Renaissance w
A revolution was to take place in
medicine at the time of the Renaissance. It was to involve the breaking of the
stranglehold classical and Arabic thought, especially Galen and Avicenna, had
on medicine and its replacement by a belief in observation and experiment. One
of the principal proponents of the new beliefs was Paracelsus who attacked
academic learning, especially Galen and Avicenna and advocated learning from
experience. His own ideas however were not much of an improvement on the
classical learning. He rejected the humoral theory, but considered everything
was made out of sulphur, mercury and salt. Sulphur caused inflammability,
mercury volatility and salt solidity in substances. He also believed in the
�doctrine of signatures� the idea that assumed plants capable of healing
visibly showed their healing qualities. Heart shaped lilac leaves would cure
heart disease and yellow celandine would cure jaundice.
However, Paracelsus�s interest in
alchemy led him to some significant discoveries. He noticed the anaesthetic
effects of ether and tincture of morphine which he called laudanum. He
recognised that particular substances had their own individual qualities and
that compounds including those substances often had some of those same
qualities. He considered that each disease needed to be cured by its own
remedy. The main value of Paracelsus�s ideas, were in his iconoclastic attack
on classical medical learning, which was held in vastly excessive reverence in
Paracelsus�s time. After Paracelsus it became easier to criticise established
medical learning and for new ideas to be accepted.
A contemporary of Paracelsus,
Fracastorius, suggested contagious disease was caused by tiny seeds invading
the human body. The seeds were too small to be seen with the human eye and
could find their way into the body from the air, from bodily contact or from
infected clothes or bed linen. Once they had entered the human body they could
multiply causing people to fall ill. Fracastorius also considered each disease
was caused by its own particular seed leading Fracastorius to clearly
distinguish between such contagious diseases as smallpox, measles, the plague,
syphilis and typhus. Previously contagious diseases were sometimes considered
to be versions of the same disease with varying degrees of intensity.
Fracastorius�s theory is virtually identical to the germ theory of disease but
in the 16th century, without microscopes, he was unable to prove the theory.
Physicians preferred other theories, such as the humoral theory, which while
also unprovable at least had the support of tradition and ancient authority.
The study of anatomy was to
undergo a revolution at the hands of Vesalius. Vesalius was able to dissect
human corpses and this enabled him to provide a generally accurate picture of
the human body. Previously anatomy had suffered from the prohibition on human
dissection that extended back to classical times, so that knowledge of human
anatomy was based on animal dissections. Before Vesalius the accepted authority
was Galen whose anatomical studies were based on animal dissection and whose
work had acquired such a status that to question it could involve accusations
of heresy.
Vesalius was able to obtain human
corpses for dissection; as public authorities were prepared to allow the
dissection of the corpses of executed criminals. Some physicians had previously
dissected the corpses of criminals, but such was the reputation of Galen that
they had not noticed or not dared to point out that the dissection of humans
showed that much of what Galen had said was wrong. Versalius�s strength was
that he was prepared to rely on his observations and where these contradicted
Galen he was prepared to say Galen was wrong. Vesalius�s great work was the De
Humani Corporis Fabrica usually called the Fabrica.� It consisted of seven books, the first
dealing with the skeleton, the second with the muscular system, the third with
the veins and arteries, the forth with the nervous system, the fifth with the
abdominal organs, the sixth with the heart and lungs and the seventh with the
brain. The Fabrica especially books 1 and 2 were illustrated with high quality
drawings showing the various human parts in considerable detail. In book 1
Vesalius emphasizes that the bones supported the human body, played an
important role in movement and provided protection for other parts of the body.
The illustrations in book 2 show the muscles in the order in which a person
dissecting a body would see them. The upper layer of muscles, are shown then
the layer below them and then the next layer and so on. Book 3 gives a good
description of the arteries and veins and book 7 describes some of the
structure of the brain for the first time.
The book corrected certain of
Galen�s errors. It questioned Galen�s suggestion that blood flowed from the
right ventricle of the heart to the left ventricle. Vesalius also showed that
the rete mirabile did not exist, that the liver was not divided into five
lobes, that the uterus had multiple chambers and that the pituitary was
directly connected to the nose. Vesalius�s expose of such errors by Galen
resulted in some criticism of Vesalius�s work from physicians who considered
any questioning of Galen to be outrageous.
Vesalius did make some errors.
His descriptions of the visceral organs (the liver, the kidney and the uterus)
were based upon those of pigs and dogs. He failed to notice the pancreas, the
ovaries and the adrenal glands. His description of female organs was poor,
probably due to there being fewer female bodies available for dissection.
Nevertheless, the book still represented an enormous advance in human knowledge
of anatomy.
(back
to content)
1.3.1 CIRCULATION OF THE BLOOD
Classical physicians were aware of the existence of
the heart, but had little idea of its function in the human body. They realized
when the heart stopped beating life would stop which led them to believe the
heart had a significant role during and at the end of life. They considered the
heart was where the soul was located when a person was living and the soul left
the body when a person died.
Classical physicians had little
understanding of the relationship between the heart and the blood. They did not
know how blood got to the heart, how it got from the right ventricle to the
left ventricle or what happened after it left the heart. They believed the
heart provided a �vital spirit� to blood passing through the heart. They also
believed the arteries did not contain blood as when a person or animal dies,
the heart stops pumping blood into the arteries, which then contract and drive
their blood into the veins. This only leaves air in the arteries of a dead
person or animal and classical physicians only dissected dead bodies and so
never discovered blood in the arteries. The veins in dead bodies are full of
blood, especially the veins connected to the liver. This led classical
physicians to believe that the liver created blood which was passed through the
veins to the rest of the body. It was also believed that the body somehow
absorbed the blood.
Galen, who had the opportunity to
observe the internal organs of living human beings while acting as physician to
injured gladiators had a better understanding of the heart and blood. He
understood the arteries contained blood in living people and that the heart was
a pump which pushed blood from the right ventricle of the heart into the lungs
which then flowed into the left ventricle and from there into the arteries.
This circulation from the right ventricle to the lungs and then to the left
ventricle was known as the pulmonary transit. Galen however still believed that
the liver created the blood, but also that it pumped the blood to the rest of
the body and that blood was passed directly form the right ventricle to the
left ventricle of the heart. The irony is that Galen�s work on the pulmonary
transit, which was at least partly right, was largely not noticed, while other
work which was quite erroneous like the humoral theory was treated as holy
writ.
The idea of the pulmonary transit
was revived by the Arab physician Ibn al-Natis in the 13th century when he
suggested that all the blood went from the right ventricle to the lungs and
then to the left ventricle and none travelled directly from the right ventricle
to the left ventricle. In the 16th century the same idea was suggested by
Michael Servetus and accepted by Realdo Colombo. Colombo also suggested the
heart could act as a pump and discovered the presence of valves in the veins
which ensured that the blood could move only in a single direction from the
right ventricle to the lungs and then to the left ventricle.
The classical ideas concerning
the heart and blood were beginning to be challenged in the 16th century. Ideas
of the pulmonary transit, the heart acting as a pump and valves in the veins
ensuring blood flowed only one way questioned the classical orthodoxy still largely
accepted in Renaissance Europe. Into this environment William Harvey proposed
his ideas of the continuous circulation of the blood.
Harvey had been carrying out
dissections on a wide range of living animals and it is from his observations
of their living organs that he was able to understand how the blood circulates
through the human body. His book De Motu Cordis begins by explaining the
structure of the heart and what it does. The heart consists of two upper parts
called the auricles and two lower parts called the ventricles. The left auricle
and the left ventricle were separated from the right auricle and the right
ventricle by an impenetrable muscular wall. The question of whether the
auricles or the ventricles beat first was difficult to resolve as hearts would
often beat too fast for normal observation to provide an answer. Harvey
answered the question by observing the hearts of cold blooded animals like fish
which beat slowly and then confirmed it by observing the slow beating hearts of
dying warm blooded animals. He observed the auricles beat first, pushing blood
into the ventricle which contracted pushing blood out of the heart.
The classical theory considered
blood was made by the liver, flowed through the heart and was absorbed by the
body. Harvey calculated the amount of blood that flowed through the heart of a
dog. He calculated the number of heart beats per minute, which was the number
of times the heart pumped blood out into the body. He also calculated the
quantity of blood that was pumped with each heart beat and concluded that the
heart pumped blood weighing three times the weight of the whole body each hour.
The question arose as to where all this blood came from, and where did it all
go. Blood equivalent to three times a person�s body weight per hour could not
come from food and drink consumed. No one could eat or drink that much per
hour. Nor could that quantity of blood be absorbed by the body every hour.
Veins, arteries and tissues would explode with that quantity of blood being
poured into them every hour. Harvey suggested the solution to this problem was
that blood was not being created by the liver or absorbed by the body, but that
the same blood was constantly circulating around the body.
Galen had suggested that the
blood moved in both directions in the veins and arteries. Harvey showed that
valves in the veins ensured that blood moved in only one direction. He showed
that blood in the veins always moved towards the heart, by pressing a vein,
blood accumulated in the vein on the side of the compression away from the
heart. The side of the compression close to the heart would be emptied of blood
as the blood flowed to the heart and away from the compression point. When an
artery was pressed the blood built up on the side of the compression closest to
the heart. This indicated the blood flowed in a single direction, in the veins
towards the heart, and in the arteries away from the heart.
The consequences of the blood all
flowing in one direction and the same blood constantly be circulated, without
blood being created by the liver or absorbed by the body was a revolution in
physiology. New ideas often receive considerable criticism and Harvey�s idea of
constantly circulating blood was attacked for daring to disagree with Galen.
One rational criticism of Harvey�s theory was that Harvey could not show how
blood flowing out of the heart to the arteries could connect to the veins and
flow back into the heart. Harvey suggested tiny connections, too small to be
seen with the naked eye, linked the arteries and the veins but he could not
prove their existence. This problem was solved by Marcello Malpighi, in 1661,
when using a microscope he was able to observe the existence of capillaries
linking the arteries and the veins which allowed blood to flow from the
arteries to the veins so that the idea of the circulation of the blood was
complete.
(back
to content)
1.3.2 JENNER AND VACCINATION
Smallpox goes back at least to
Ancient Egypt and was in Greece in the classical period and was present in
Ancient China and India. The symptoms of the disease were described by Al-Razi
in 910 CE and involved blisters filled with puss appearing on the eyes, face,
arms and legs. Twenty to forty percent of those who caught smallpox died from it
and the survivors were covered with disfiguring scars. In London in the 17th
and 18th centuries a third of the people had smallpox scars and the majority of
cases of blindness were caused by smallpox.
It had been observed that people
who survived smallpox did not usually catch it again. The idea developed that
if a mild case of smallpox could be produced it would protect a person from
future smallpox attacks. In the East dust from a smallpox scab was blown into
the nose to induce a mild case of smallpox to create immunity from future
attacks. In Ottoman Turkey smallpox material was rubbed into small cuts made in
a person�s arm. These methods of conferring immunity from smallpox were made
known in England in the early 18th century but were ignored.
The practice of deliberately
giving a person a mild case of smallpox began in England in the early18th
century with Lady Mary Montagu. The practice became known as variolation and
Lady Montagu who had learnt about the practice in Turkey had her own daughter
variolated in the presence of newspaper reporters which ensured substantial
publicity. Lady Montagu then persuaded the Prince and Princess of Wales to have
their children variolated which ensured even more publicity. Variolation also
took place in America where Zabdiel Boylston, a Boston physician, heard of
variolation from an African slave and faced with a smallpox epidemic variolated
244 people of whom only 6 died. Surgeons however demanded patients go through a
6 week period of bleeding, purging and dieting before variolation which limited
the popularity of the practice and resulted in patients being weakened before
variolation took place. Variolation turned out to be quite dangerous with
modern estimates that 12% of patients died; a lower death rate than the 20-40%
who might die in a smallpox epidemic, but certainly not a perfect treatment for
the problem of smallpox.
A better treatment was to come
with Edward Jenner, who while training as a surgeon in 1768, heard that
milkmaids who had contacted cowpox were immune from smallpox. Cowpox resulted
in lesions on the milkmaids hands, but had no other symptoms. Later Jenner met
a Mr Frewster who in 1765 had presented a paper to the London medical society
on the ability of cowpox to prevent future smallpox attacks. The paper was
never published but reminded Jenner of what he had heard of cowpox from the
milkmaids. Cowpox is part of a family of animal poxes, including horsepox,
cowpox, swinepox and smallpox all caused by the orthopox virus. All the animal
pox diseases can infect humans and an infection from anyone of them will
protect people from all the other animal poxes. In December 1789 Jenner began a
series of experiments. He inoculated three people including his son with
swinepox and later variolated them with smallpox and none of them produced the
rash that usually came from variolation with smallpox. Swinepox seemed to
protect them from smallpox. Later in 1796 Jenner put cowpox into a healthy 8
year old boy and after he developed normal cowpox symptoms variolated him with
smallpox. The boy did not develop any of the symptoms that normally occurred
with variolation with smallpox. Jenner then took fluid from the boy�s cowpox
pustle and used it to inoculate some more children and fluid from their cowpox
pustles was used to inoculate some more children. Two of these were later
variolated with smallpox, but did not develop any of the symptoms that normally
occurred with variolation, confirming the initial experiment. The experiment
showed that cowpox could provide protection against smallpox without any of the
risks of variolation. The practice of cowpox inoculations, which began to be
called vaccination, was soon done throughout the British Empire, the United
States and Europe although there was some opposition to it. The opposition
gradually disappeared and eventually late in the twentieth century smallpox was
completely eliminated.
1.3.3 THE DISCOVERY OF ANAESTHESIA
A vital component of modern
surgical operations is the use of anaesthesia. Without anaesthesia operations
would be excruciatingly painful and as a result many patients chose not to have
operations. The pain of having limbs amputated could result in patients dying
of shock and forced surgeons to perform operations with extreme speed. The best
surgeons could amputate a limb in less than a minute. The state of mind of a
person awaiting surgery would be similar to that of a person about to be
tortured or executed. When London hospital was built in 1791, and was to act as
a model for other hospitals, the design took into account the lack of effective
anaesthetics. The operating room was on the top floor, partly to allow sunlight
through a skylight to illuminate the operation, but also so the patient�s
screams would not travel through the hospital and could be muffled by extra
heavy doors. When an operation was to commence hospital staff would go to the
top floor and assist in holding the patient down and if necessary in gagging
the patient.
The problem with an effective
aesthetic that will allow major surgery is that it must place the patient in a
state where the central nervous system is depressed to an extent where painful
stimuli cause no muscular or other reflexes. This is far beyond ordinary sleep
as obviously performing surgery on a sleeping person will wake them. Effective
surgical anaesthesia must place the patient in a state close to that of death.
In the past various attempts were made to reduce or eliminate pain during
surgical procedures. Dioscorides, a Greek physician in the early Roman Empire,
used drugs such as henbane and mandrake root to relieve pain. These drugs
continued to be used into medieval times. Arab physicians seemed to have used
drugs such as opium and hyoscyamus. Alcohol was often used but was probably
more effective at making the patient easier to hold down than in relieving
pain.� Soporific sponges, involving the
inhalation of drugs such as opium, mandragora and hyoscyamus were used from
around the ninth century. However modern experiments with such sponges suggest
they had no aesthetic effect at all. The use of soporific sponges was
discontinued in the seventeenth century. It may well be due to the lack of
effectiveness of pre-modern anaesthetics that their use was not widespread.
Egyptian papyri and the Code of Hammurabi describe surgery without mention of
anaesthetics. Only one Chinese surgeon, one Indian surgeon and a few Greek,
Roman and Arab surgeons seem to have made any attempt to relieve pain during
surgery. Pre-modern attempts to relieve pain during surgical operations seem to
have been of little or no effect.
The first step in the development
of modern anaesthetics was the discovery of ether. In 1275, the Spanish
alchemist Raymundus Lullius produced ether by mixing alcohol with sulfuric
acid. Paracelsus used ether to relieve pain in 1605 in some of his medical
patients but not in surgery as he was not a surgeon.
Nitrous oxide, soon to be known
as laughing gas, was discovered by Joseph Priestly in 1772. Priestley however
did not realize nitrous oxide could act as an anaesthetic. Others however soon
discovered both nitrous oxide and ether had an intoxicating effect when inhaled
and soon �ether frolics� and �laughing gas parties� became a popular source of
amusement. It was soon observed that minor injuries such as bruises received at
the frolics and parties were not accompanied by any pain. In addition, Humphrey
Davy discovered that nitrous oxide relieved the pain of an inflamed gum and jaw
and suggested nitrous oxide could be used in surgery. Similar observations
concerning nitrous oxide were made by William Barton in the United States. In
1842 ether was used to painlessly extract a tooth, by a dentist, Dr.� Elija Pope, acting on the suggestion of
William Clark a chemistry student who had participated in ether frolics.
The first use of ether for
surgical purposes was by Crawford Long in Georgia, USA in 1842. Long had
attended ether frolics and had noticed bruises he had received while under the
influence of ether had involved no pain. Realizing that ether had stopped the
pain he used it in various surgical operations and in obstetrical procedures.
He did not however publish his work until 1849.
A dentist, Horace Wells, while
attending a nitrous oxide party in 1844 noticed a person injuring his legs
without suffering any pain. Realizing nitrous oxide could serve as a dental
anaesthetic Wells had one of his own decaying teeth removed by another dentist
while he was under the influence of nitrous oxide. Wells experienced no pain
and was soon performing dentistry using nitrous oxide on his own patients.
However, when he attempted a public demonstration at Massachusetts General
Hospital he used insufficient gas and the demonstration was not a success.
The public demonstration at
Massachusetts General Hospital had been arranged by Wells former dentistry
partner William Morton. Morton, who had possibly seen Long operate in Georgia,
became interested in ether as an anaesthetic and had discussed it with Charles
Jackson, a doctor in Harvard�s medical faculty and at Massachusetts General
Hospital. Intending to patent the anaesthetic Morton and Jackson disguised the
ether by mixing it with aromatic oils and called it Letheon. They then arranged
public demonstrations of the use of Letheon, in 1846, for pulling teeth and for
an operation removing a tumour from a patient�s jaw. Both the dentistry and the
operation were carried out painlessly. Jackson and Morton however were forced
to withdraw the patent for Letheon and reveal that Letheon was really ether by
pressure from the surgeons involved in the operations. By the end of 1846 news
of the use of ether as an anaesthetic had travelled across the Atlantic and in
December 1846 it was used in an operation in London.
Jackson, Morton and Wells all
claimed to be the discoverer of surgical anaesthesia and in 1847 the United
States Congress became involved in trying to sort out who was the true discoverer
of anaesthesia. Congress eventually dismissed Wells and Morton�s claims and
decided it was between Jackson and Long. The American Medical Association, in
1872, gave the credit to Wells, while in 1913 the electors of the New York
University Hall of Fame named Morton as the discoverer of surgical anaesthesia.
The American College of Surgeons, in 1921, decided Long should be credited with
the discovery.
Attempts were soon made to use
ether in obstetrics but it was found to be unsuitable. Ether often produced
vomiting patients, irritated lungs and a bad smell. Chloroform had been
discovered independently in 1831 by Samuel Gutherie in New York, by Eugene
Soubeiran in Paris and by Liebig. Initially its anaesthetic quality was not
recognised but Gutherie�s daughter had become unconscious for several hours
after tasting it. In 1847 Sir James Simpson while looking for an anaesthetic to
use in obstetrics tried chloroform on himself and having found it to be an
effective anaesthetic began using it in surgical operations. Its use was soon
extended to obstetrics provoking considerable opposition from the Calvinist
Church in Scotland on the grounds the Bible stated �In sorrow thou shalt bring
forth children� showed women must suffer when giving birth. The Calvinist
church opposition disappeared when Queen Victoria gave birth to her eighth
child under the influence of chloroform. However, chloroform was soon
discovered to have its own problems as it could cause liver damage and five
times as many people died under chloroform as died under ether.
The method of application of the
anaesthetic developed over time. Long had simply poured ether into a towel for
his patient to inhale. Morton used an inhaler made up of a round glass bottle
with two holes and a mouth piece. Air passed through one hole into the bottle
which contained a sponge soaked in the ether which was then inhaled by the
patient through the mouth piece which was attached to the other hole. Morton�s
inhaler did not allow the anaesthetist to have control over the amount of
anaesthetic. Soon John Snow, who had provided the chloroform to Queen Victoria,
created an improved inhaler which provided a 4% mix of chloroform in air.
Joseph Clover produced a further improved inhaler in which the chloroform and
air mixture was prepared in advance and held in an air tight bag. Sir Francis
Shipway created an apparatus which allowed the anaesthetist to control a
mixture of varying amounts of chloroform, ether and oxygen for inhalation by
the patient.
A significant improvement in the
provision of anaesthetics occurred with the introduction of the anaesthetic
directly into the windpipe or trachea. This was first attempted by Frederick
Trendelenburg, in 1869, who inserted the anaesthetic through a tube he inserted
into a hole he had cut into the patient�s windpipe. Sir Ian Macewan achieved
the same result without cutting into the windpipe, in 1880, by inserting a
metal pipe the throat and into the windpipe. This allowed the development of endotracheal
anaesthesia which was important for operations on the mouth and the jaw and for
many modern cardiac and pulmonary operations. Endotracheal anaesthesia was
further improved, in 1919, when Sir Ian Magill put tubes through the conscious
patient�s nose and mouth and down into the windpipe by anaesthetizing the
throat with cocaine before inserting the tubes.
General anaesthetics were often
not necessary for minor operations. A local anaesthetic which worked on a
particular part of the body and avoided the small risk of death and several
hours of recovery time involved with general anaesthetics was sought. Peruvian
Indians knew about the anaesthetic qualities of the coca plants and in the
nineteenth century cocaine was obtained from the plant. In 1872 Alexander
Bennett observed that cocaine had anaesthetic properties and in the 1880�s Carl
Koller experimented with cocaine using it to anaesthetize frog�s eyes. Soon
cocaine began to be used as a local anaesthetic for eyes, the mouth, nose and
throat and in the urethra. The use of cocaine was extended by injecting it into
the nerves relating to the area to be operated on and eventually into the
epidural space around the spinal cord which allowed a larger area to be
anaesthetized. The use of cocaine as a local anaesthetic has discontinued with
its replacement by novocaine which was synthesized as an aesthetic after 1905.
1.3.4 THE GERM THEORY OF DISEASE��������������������������������������������������������������������
(back to
content)
The first person to see
micro-organisms was Anthony Leeuwenhoek (1632-1723) a Dutch draper who was an
expert maker of microscopes. His microscopes gave a degree of magnification
which was not exceeded until the 19th century. He used his microscopes for
observing a wide variety of phenomena. In 1675 and 1676 he looked at drops of
rain water and found tiny animals within the water. Those animals would have
included what we now call bacteria and other micro-organisms. In 1683
Leeuwenhoek looked at plaque from his own teeth and found it contained large
numbers of small animals. Later samples of plaque did not contain the small
animals, which Leeuwenhoek suspected was because his drinking of hot coffee
killed the little animals. Leeuwenhoek also looked at scrapings from his tongue
when he was sick and at the decay in the roots of a rotten tooth he had
removed. In both cases he found vast numbers of the little animals. The
presence of these animals in such great numbers in places of illness and decay
raised the question as to whether the animals arose from the decay or whether
they were attracted to it or whether they caused the decay. The question of
whether the small animals were spontaneously generated from decaying materials
or were attracted to it was the subject of much controversy. Francesco Redi
(1626-1698) kept boiled meat in sealed containers and when maggots failed to
appear suggested this showed there was no spontaneous generation. However, in
1748 John Needham repeated the experiment and found small animals in the meat
which he considered proved spontaneous generation. Lazzaro Spallanzoni
suggested Needham had failed to seal his containers properly so that the small
animals arrived on the meat through the air, rather than being spontaneously
generated by the meat. Supporters of spontaneous generation argued that sealing
the containers prevented some gaseous substance, necessary for spontaneous
generation, from reaching the meat and so preventing the generation of the
living organisms.
Whether micro-organisms caused
the diseases they were so often found with, was investigated by Agostino Bassi.
In 1835 he showed that the silkworm disease, muscarine, was caused by bacteria.
When he inoculated healthy silkworms with the bacteria, he produced the
sickness in the silkworms. This suggested that other diseases may be caused by
bacteria.
The questions of spontaneous
generation and whether micro-organisms played any role in causing disease were
eventually settled by Louis Pasteur. He was to show that fermentation in wine,
putrefaction of meat and infection in human disease all involved the same
process and were all caused by the activities of micro-organisms. The
micro-organisms were generated not by decaying matter but were continually
present in the air and when they were present in great numbers and were of
unusual strength they could cause matter to decay and human beings to fall ill.
�
Pasteur began with fermentation in wine. At the time chemists such as
Wohler and Justus von
Liebig suggested fermentation was
solely a chemical process with living organisms playing no role in the process.
Fermentation in wine was a problem as sometimes the fermentation went wrong and
soured the wine. Pasteur showed that fermentation was caused by micro-organisms
in yeast and that round yeast cells produced good wine, but long yeast cells
created lactric acid which caused the wine to go sour. Pasteur showed that if
the wine was heated it would kill the yeast and stop any of the wine going
sour.
Pasteur next began to investigate
putrefaction in meat with an experiment that allowed air to reach boiled meat
via an undulating u shaped tube. The meat did not putrefy and Pasteur
considered this was because the dust particles containing the micro-organisms
were caught on the low bend of the tube as they could not travel up the tube
due to gravity. The micro-organisms did not reach the meat even though it was
exposed to air so the meat did not putrefy. This showed it was not air that
caused putrefaction, but micro-organisms in the air.
Pasteur then began to investigate
diseases in living organisms, first with silkworms and then anthrax which
affects sheep and cattle and occasionally humans. Pasteur showed the disease
killing silkworms were two different sorts of micro-organisms which caused two
different diseases in the silkworms. In relation to anthrax it was already
known that the blood of cattle, which had died from anthrax, contained
micro-organisms and that these micro-organisms were the cause of the disease.
Robert Koch had discovered the anthrax bacteria, had cultured it, and injected
it into animals which had immediately died. He also found that anthrax
micro-organisms could sometimes form spores, which were tiny organisms�
resistant to a range of environmental conditions. The spores were formed when
the temperature was right and oxygen was present. Once the spores were formed
they could survive for a considerable time and re-infect other animals making
the disease difficult to control. Pasteur, with some difficulty, then produced
an anthrax vaccine which he used to inoculate sheep which were later injected
with the anthrax bacteria. The sheep did not develop anthrax and Pasteur had
found a vaccine for anthrax.
Pasteur�s last great achievement
was to discover a vaccine for rabies. Rabies normally occurs in humans after
they have been bitten by a rabid dog with the symptoms appearing between 10
days and several months after the dog bites took place. Pasteur studied the
tissues of rabid dogs but could not find a micro-organism that could have
caused rabies. He decided the organism was too small to be detected with a
microscope. Pasteur considered the micro-organism entered the body through the
bite wound and over time moved to the brain, explaining the period of time
between the bite and the arrival of symptoms. After some time, Pasteur was able
to produce a vaccine for rabies which was able to be injected in the period
after the dog bite and before the onset of symptoms.
Pasteur�s work had followed a
logical path. He had first shown that fermentation was caused by
micro-organisms, and that those micro-organisms originated in the air rather
than from the fermenting matter and that micro-organisms also caused
putrefaction and infectious disease. He then showed how the diseases in both
animals and people could be cured by vaccination. Pasteur�s work established
the germ theory of disease and put an end to other theories of disease such as
the humoral theory.
Robert Koch, after isolating the
anthrax bacteria, began using an improved microscope with a light condenser and
an oil immersion lens. This enabled him to see bacteria that had previously
been too small to be seen even with the best microscopes available. He also
used new aniline dyes which helped him to distinguish between different types
of bacteria. Koch also found a way of producing pure cultures of different
types of bacteria by placing the bacteria on a solid culture medium, in place
of the liquid culture medium then currently used, which only worked well with
bacteria that moved in the blood stream. With his improved microscope and
better techniques for creating pure cultures of bacteria Koch began to search
for a tuberculosis bacterium, in the tissue of humans who had died of
tuberculosis. Using a microscope equipped with the oil immersion lens and
condenser that was five times as powerful as Leeuwenhoek�s microscopes he was
able to find a tiny bacterium which he called the tubercle bacillus. The
tubercle bacillus was much smaller than the anthrax bacteria and was too small
to be found without the use of his new improved microscope. To prove the
tubercle bacillus caused tuberculosis Koch needed to isolate it in a pure
culture and to inject it into various animals. If it produced tuberculosis in
those animals that would prove the tubercle bacillus was the cause of
tuberculosis. After some difficulty he was able to produce a pure culture of
the tubercle bacilli. He then injected this into animals which soon became sick
and when he examined their diseased tissues he found they had tuberculosis.
Koch had found the cause of tuberculosis giving hope that a cure would
eventually become possible.
If Pasteur established the germ
theory of disease, it was Koch who was to turn bacteriology into a science.
Koch formalized the methods for studying micro-organisms and proving their
relationship with particular diseases. To prove an organism was the cause of a
disease Koch proposed the following criteria, which came to be known as Koch�s
postulates:
1. The organism must be present
in every case of the disease.
2. It must be possible to prepare
a pure culture, maintainable over repeated generations.
3. The disease must be reproduced
in animals using the pure culture, several generations removed from the
organism originally isolated.
4. The organism must be able to
be recovered from the inoculated animal and be re-produced again in a pure
culture.
Clearly the third and fourth
postulates can only apply to diseases which apply to animals as well as humans
and the postulates were not able to be applied to all micro-organisms for
example viruses. Nevertheless, the postulates provided a set of procedures for
the investigation of diseases which were to establish the causes of a range of
diseases which opened up the possibility of finding cures and treatments for
the diseases. Between 1879 and 1906 the micro-organisms causing many diseases
were discovered. The diseases involved included gonorrhoea (1879), typhoid
fever (1880), suppuration (1881), glanders (1882), tuberculosis (1882),
pneumonia (1882 and 1883), erysipelas (1883), cholera (1883), diphtheria
(1883-4), tetanus (1884), cerebrospinal meningitis (1887), food poisoning
(1888), soft chancre (1889), influenza (1892), gas-gangrene (1892), plague
(1894), pseudo-tuberculosis of cattle (1895), botulism (1896), bacillary dysentery
(1898), paratyphoid fever (1900) syphilis (1905), and whooping cough (1906).
The discovery of the micro-organism causing the disease did not always result
in effective treatments.
1.3.5
ANTISEPTICS����������������������������������������������������������������������������������������������������������
(back to content)
The increase in surgery produced
by the use of anaesthetics simply highlighted another problem, the death of
large numbers of patients due to infection. Patients dying from infection had
long been a problem both in obstetrics and surgery. It was in obstetrics that
the first understanding of the causes of infection arose, but it was in surgery
that the solution to the problem was achieved.
Some doctors and surgeons sensed
that a lack of cleanliness may be the cause of infection. Charles White in 1773
in Manchester suggested the cleaning of the surgery room, clothing and articles
in contact with the patients but did not refer to cleansing of surgeons and
others involved in operations. Alexander Gordon (1752-1799) suggested infection
was carried from infected patients to uninfected patients. He suggested the
cleansing of surgeons but did not realize that infected matter was involved in
the spread of disease.
In the mid nineteenth century
Ignaz Semmelweis was working at the maternity clinic at Vienna General Hospital.� He noticed that the section of the hospital
used for training medical students in obstetrics had a much higher rate of
mortality, around 13% than the section used to train midwives, which was around
2-3%. Explanations considered for the variations in the mortality rates
included that the poor single mothers and prostitutes in the hospital were less
embarrassed when treated by women. Semmelweis noticed that the puerperal fever
which killed many of the women immediately after they had given birth seemed to
be the same disease that had killed the surgeon Jakob Kolletschka who died
after cutting his finger in a post mortem. Later Semmelweis realized that
medical students going to their section of the maternity clinic came from
anatomy classes involving dissections and the handling of diseased body parts.
Little attempt was made to clean up between the anatomy classes and the work
done in the maternity clinic. Semmelweis suspected the students coming from the
anatomy classes were bringing infection into the maternity clinic so he ordered
students to wash and scrub in a chlorine solution before entering the maternity
clinic. Within a month the mortality rate in the students� section dropped to
2% the same as for the midwives� section. Despite his success Semmelweis became
very unpopular with the medical students, his immediate superior and even the
patients who felt he was suggesting they were dirty. Semmelweis left Vienna for
a hospital in Budapest where he instituted similar hygienic reforms and again
the mortality rate dropped dramatically. He published a paper on his
discoveries, which was ignored, and then a book which was also ignored.
Semmelweis then began to behave erratically writing angry letters to those who
criticised his work. He was soon induced or forced to enter a mental hospital
and within two weeks was dead in circumstances that may have amounted to
murder.
Joseph Lister was a surgeon in
Glasgow who noticed that the mortality rate for compound bone fractures where
the bone was exposed to the air were much higher than for broken bones where
there was no exposure to the air. Broken bones exposed to the air often
developed gangrene which was usually blamed on �miasma� or bad air. Lister did
some experiments on frogs legs and concluded that gangrene was a form of
rotting, involving the decomposition of organic material. He also read
Pasteur�s work which suggested that putrefaction was the rotting of organic
material caused by bacteria in the air. Lister accepted Pasteur�s idea that it
was not the air that caused the gangrene but bacteria in the air.
The question was how to destroy
the bacteria both in the air and in the wounds. Carbolic acid or phenol had
been isolated in the 1830�s through coal tar distillation. It was used to clean
sewers and after various experiments with crude carbolic, which killed tissue,
Lister began to use carbolic acid. He would dress wounds in lint soaked with
carbolic acid and sprayed the air in the operating room with carbolic acid.
Lister published his work in 1867 in a paper entitled On the Antiseptic
Principle in the Practice of Surgery. The mortality rates from Lister�s
amputation operations fell from 45% to 15%, but despite this some doctors still
refused to believe that bacteria existed or could cause infection. However, the
results of using Lister�s methods soon became obvious and they began to be used
throughout Europe. Over time he refined his procedures getting rid of the
carbolic spray and putting greater emphasis on using heat to sterilize
dressings and instruments. There was also a move from anti-septic measures
which destroyed germs in wounds to aseptic measures which ensures that
everything that touches the wound such as instruments and the surgeon�s hands
are free from germs.
Towards the end of the 19th
century sterilized gowns, masks, caps and rubber gloves were introduced for
surgical operations.
1.3.6 ANTIBIOTICS����������������������������������������������������������������������������������������������������������
(back to content)
Scientists experimenting with
bacteria had on various occasions noticed that penicillin and other biological
organisms could inhibit the growth of bacteria. In 1875 John Tyndall had
observed penicillin had killed bacteria in some of his test tubes. In 1877
Pasteur had noted anthrax bacilli grew in sterile urine but the addition of
�common bacteria� stopped the growth.� In
1885 Arnaldo Canteri noted certain bacterial strains killed tubercle bacilli
and reduced fever in the throat of a tubercular child. In 1896 a French medical
student noted that animals inoculated with penicillin and a virulent bacterium
did better than animals inoculated with the virulent bacteria only. In 1925 D A
Gratia noted that penicillin could kill anthrax bacilli.
Alexander Fleming was
experimenting with bacteria in 1928 when he observed bacteria in his petri dish
had been killed by the Penicillium mould. Fleming began experimenting with the
mould and soon isolated the substance that killed the bacteria. He called the
substance penicillin and then tested its effectiveness against other bacteria.
He found penicillin could kill a range of bacteria but there were some bacteria
it did not affect. He injected it into animals and found that it did not do
them any harm. Fleming then published his results in 1929 and then in a briefer
report in 1932. Fleming�s work was largely ignored and he then turned his
research interests elsewhere. The prevailing scientific view at the time was
that anti-bacterial drugs would not work against infectious disease and would
be so toxic to use on humans.�
This belief to change 1935 when
it was that Prontosil could destroy streptococcal infection when given
intravenously. Research on penicillin only began again in 1940, in Oxford, when
Howard Florey and Ernest Chain discovered penicillin was an unstable simple
molecule. They were able to stabilize it by freeze drying it in a water
solution. This produced a powder that was tested on mice and did not harm them
and cured them of streptococci. It was also discovered that penicillin could
travel through the body to attack infections wherever they were. Their results
were published in August 1940 and Florey, Chain and their colleagues began to
manufacture penicillin as fast as possible.
The first human test of
penicillin was on a badly ill policeman. The policeman improved until he seemed
on the verge of total recovery when the supply of penicillin ran out and the
policeman relapsed and died. More penicillin was manufactured and tested on
humans and was found to regularly clean up infections. It was found to be
effective against most forms of pus forming cocci and against tetanus, anthrax,
syphilis and pneumonia. The manufacture of penicillin was greatly expanded when
the United States began to produce it and new manufacturing techniques
involving deep fermentation were developed. This involved submerging the mould below
the surface of the culture medium. Eventually semisynthetic penicillins and
penicillins that could be swallowed were produced.
Eventually a systematic search
began for other anti-biotics. Howard Florey outlined the procedure to be
followed which involved the investigation of micro-organisms to find out which
ones produced an anti-bacterial substance, the isolation of that substance,
testing the substance for toxicity, testing it in animal experiments and then
testing it on people. The search for new anti-biotics was to produce a
substantial number of new anti-biotics including streptomycin developed in 1944
which was effective against tuberculosis. Chloramphenicol, developed in 1949,
was effective against typhoid fever. Anti- biotics were eventually found that
could act against every bacteria that causes diseases in humans. Some of those
bacteria are now developing resistance to anti-biotics and the development of
new anti-biotics is inhibited by the extreme cost, running into hundreds of
millions of dollars, of obtaining United States government approval for the
drugs. Nevertheless, anti-biotics have saved hundreds of millions of lives.
1.3.7 MEDICAL STATISTICS������������������������������������������������������������������������������������������
(back to content)
The use of statistics in medicine
to determine the cause of disease or the success of a treatment has a
relatively short history. In the past the causes of disease and the success of
treatments were usually decided by physician�s personal experience with
patients, which, assuming that physicians had similar experiences, led to
accepted beliefs as to the efficacy of treatments and the causes of disease.
The beliefs would be recorded in authoritative medical texts and would in many
cases become a sort of medical dogma. Disputing the dogma could involve
accusations of unorthodox opinions that could lead to bad practices that could
endanger patients� lives.
The idea of doing trials, to test
the effectiveness of medical treatments, was suggested by the scientist,
Johannes van Helmont and the philosopher George Berkeley. The first known trial
to assess the cause of a disease seems to have been done by James Lind in an
attempt to discover the cause of scurvy. Scurvy was killing large numbers of
sailors on long sea voyages. Lind took 12 scurvy sufferers and divided them
into 6 groups of 2 and each group was given a different dietary supplement. The
two sailors given oranges and lemons rapidly recovered and the others did
not.� Lind eventually published his
findings, and although there remained some confusion for some time, eventually
lemon juice became standard on long sea voyages.
One question, much debated in the
18th century, was whether smallpox inoculation was a good thing. In England
inoculation was generally favoured, in France it was opposed. Various calculations
were made as to the death rate from smallpox which was considered to be around
one in ten, excluding fatalities of those under 2 years old. Other calculations
were 1 in 12 and 1 in 7. This was compared to the death rate from inoculation
which James Jurin, secretary of the Royal Society, calculated at 1 in 91. The
Swiss mathematician, Daniel Bernoulli calculated that inoculation increased the
average life expectancy by two years. A further problem was that people
inoculated with smallpox could spread it to others and this was not taken into
account in calculating death rates from inoculation. If people who were
inoculated could be isolated for a period, then the figure might not be too
high, but then if people who got smallpox naturally were isolated that would
reduce the death rate from normal smallpox. An additional problem was that the
rate of smallpox infection varied considerably from large cities where nearly
everyone would, sooner or later get smallpox and the small towns and villages
where most people in the 18th century lived, and many people could live their
lives without getting smallpox. Modern estimates of the death rate from
inoculation are as high as 12%, not much better than the death rate from normal
smallpox infection.
The difficulty in calculating
accurate death rates for inoculation and normal smallpox infection, how to
introduce into the figures people who caught smallpox from those who were
inoculated and how to deal with the widely varying rates of smallpox infection
between urban and rural areas gives some idea of the difficulty in working out
whether inoculation was a good thing or a bad thing. The whole debate
eventually became irrelevant when vaccination with cowpox, a quite safe form of
immunization became available at the end of the 18th century. A further
illustration of the problem of accurate statistical analysis of medical
treatments is contained in the work of Pierre Louis in the first half of the
nineteenth century.� Louis conducted
several trials to test bloodletting as a treatment for various inflammatory
diseases. He concluded from his trials that bleeding resulted in patients
recovering earlier than if there was no bleeding and that if bleeding is done,
patients bleed earlier during the course of the disease recovered more quickly
than those bleed later. However, the way Louis conducted the trial was not
ideal. Those bleed earlier during the illness were on average 8 years and 5
months younger than those bleed later, which could explain the faster recovery.
A further criticism of Louis�s study was that the numbers involved in his trial
were insufficient so there was a wide margin of error in his results so they
were not reliable.
A more successful use of
statistics to discover the cause of disease occurred in the mid-19th century
when John Snow discovered the cause of cholera. Cholera was like many
infectious diseases, assumed to be caused by miasma or bad air caused by
putrefaction. Snow suspected that cholera could be transmitted by personal
contact and through polluted water supplies. He examined the sources of the
water supplies in London and compared it to mortality rates from cholera. Areas
with clean water supplies, due to water being taken from the Thames above
sewage outfalls, or with filtered water, or with water passed through
settlement ponds, showed much lower rates of cholera than areas using
unfiltered and unponded water taken from below sewage outlets. Areas with clean
water had a death rate of 10 per 10,000 from cholera, areas with polluted water
had a death rate of 110 per 10,000 from cholera.
Snow also investigated the
cholera levels for households in the same areas, where the water supplies came
from two separate companies, one of which supplied clean water to its customers
and the other which supplied polluted water. Those customers obtaining clean
water had 5 cholera deaths per 10,000, those obtaining polluted water had 71
cholera deaths per 10,000. The 5 cholera deaths per 10,000 could have been
caused by visiting houses, pubs and cafes with polluted water and people who
had fallen sick with cholera.
Snow�s final study concerned a
small area around Broad Street in London where 500 people died of cholera in
ten days. Snow suspected a water pump supplying drinking water in the centre of
the area could be responsible so he asked the local authority to remove the
handle from the pump. This was done and the cholera outbreak ended. More
particularly Snow showed certain groups within the Broad Street area, people in
a workhouse and those working in a brewery who did not use water from the pump
had an unusually low cholera death rate. He also showed that certain
individuals from outside the Broad street area who drank water from the pump
also died of cholera within the ten day period.
Snow�s three studies provided
powerful evidence that polluted water caused cholera but his findings were
initially rejected. Two inquiries considered cholera still came from bad air
and another study which concluded that the death rate from cholera rose as one
moved from highlands to sea level also suggested bad air was to blame.
Eventually, when miasmic theories of disease lost creditability with the rise
of the germ theory of disease, Snow�s explanation of cholera was accepted.
The first truly scientific
randomised control test was that conducted on the drugs streptomycin and PAS as
a treatment for tuberculosis. Tuberculosis was in the mid twentieth century,
the most common fatal infectious disease in the western world. Its cause, the
tubercle bacillus, had been identified by Robert Koch in 1885, but no effective
treatment had been found for it. Antibiotics like penicillin did not work
against it, as it had an impermeable waxy coat that protected it from
antibiotics.
A new drug called streptomycin
had been discovered in America in 1944 which seemed to work against
tuberculosis germs. It inhibited the growth of tuberculosis bacillus on ager
plates and was successful at curing tuberculosis in guinea pigs and when tried
on a human patient with five courses of treatment between November 1944 and
April 1945, cured the human patient. A second drug which showed promise as a
tuberculosis treatment was PAS. It had been noted that Aspirin resulted in the
tuberculosis bacilli absorbing increased amounts of oxygen and it was
considered that a similar drug to Aspirin might block the supply of oxygen to
the tubercle bacilli. PAS was tried and was shown to cause an improvement in
the condition of tuberculosis patients. Immediately after World War II Britain
was short of money and could afford only a very small amount of streptomycin.
The Tuberculosis Trial Committee, encouraged by one of its members Austin
Bradford Hill, recognised there was not enough streptomycin to provide to all
patients, decided to conduct a random control test with the streptomycin,
providing streptomycin to one set of patients and comparing the results with
another set of patients not receiving the drug. There was enough streptomycin
to provide to 55 patients and the results of the treatment were compared with
52 patients who received the usual treatment provided for tuberculosis
patients. Which patients received the streptomycin and which received the usual
tuberculosis treatment was decided completely at random to avoid any conscious
or unconscious bias in the allocation of patients to either group.
Six months after the trial had
begun it was found that only four patients had died from the group given
streptomycin while fourteen had died from the group receiving the conventional
treatment. Streptomycin seemed to be an effective treatment with significantly
fewer deaths in the group receiving the streptomycin. However, a follow up
investigation three years later revealed 32 of the group using the streptomycin
had died compared to 35 in the group not receiving the drug. After three years
the group using the streptomycin was only slightly better off than the group
not using it. What had happened was that over the period of treatment some of
the tubercle bacilli had become resistant to the streptomycin and when this
happened patients who initially seemed to be getting better, worsened and often
died. The test revealed that not only did streptomycin not work in the longer
term but that there was a problem of the bacilli becoming resistant to the
streptomycin which, if it could be overcome could mean that streptomycin could
still be an effective treatment for tuberculosis. If the drugs had simply be
provided to doctors for treating patients it would have taken much longer to
work out why it was not working.
A further trial was conducted
which combined streptomycin with PAS with the aim ofovercoming the problem of
resistance from the tubercle bacilli. In the second trial resistance to
streptomycin developed in only 5 patients compared to 33 in the first trial.
The combination of the two drugs proved to be an effective treatment for
tuberculosis and survival rates for tuberculosis patients went up to 80%.
Eventually other drugs such as isoniazid and rifampicin were introduced and it
was found that combining three drugs resulted in survival rates approaching
100%.
Random controlled trials were
also found to be effective in proving the causes of certain diseases. After
World War II the great majority of the adult population smoked and lung cancer
deaths were rapidly increasing. Bradford Hill, Edward Kennaway, Percy Stock and
Dr Richard Doll were asked to investigate whether smoking was a cause of the
increasing number of lung cancer deaths. Smoking was only one possible
explanation, others such as increased air pollution especially from motor
vehicles were considered to be as likely or more likely the cause of increased
lung cancer deaths, than smoking. The asphalting of roads was considered to be
another possible cause of the escalating lung cancer deaths. Given that most
adults smoked it was difficult to find a suitable control group of non-smokers.
The investigation was conducted by creating a detailed questionnaire which
patients suspected of having lung cancer completed. The questionnaire was also
completed by patients who had other cancers and also by patients in hospital
for reasons other than cancer to act as two control groups. It was found that
99.7% of the lung cancer patients smoked against 95.8% of the control group
patients. This was not a great difference but it was also found that 4.9% of
the lung cancer patients smoked 50 cigarettes a day as opposed to only 2% of
the control group patients.
The lung cancer rate amongst
those smoking 50 cigarettes a day was over double for lung cancer patients than
for the control group. The more people smoked the greater their chances of
getting lung cancer. The study conducted by Doll and Bradford Hill had looked
at lung cancer patients and looked back in time at their smoking habits. They
then decided to do a study of healthy people investigating their smoking habits
and then observing how their health developed in the future. Doll and Bradford
Hill decided to do the study on doctors, 40,000 of whom filled in and returned
their questionnaire. Two and a half years later enough doctors had died for
Doll and Bradford Hill to be able to show that the more the doctors smoked the
greater the likelihood they had died of lung cancer. It was eventually found
that doctors smoking 25 cigarettes per day were 25 times as likely to develop
lung cancer compared to non- smokers.
The success of the random control
tests on streptomycin and in showing that smoking caused lung cancer led to
random control tests becoming standard practice to test new drugs and to
identify the causes of disease. The testing has had its undesirable side with
the testing costs running to hundreds of millions of dollars and so
discouraging the production of new drugs and some studies of disease showing a
relationship between environmental factors and the disease without giving any
real indication of a cause and effect relationship.
(back to content)
1.3.8 DIAGNOSTIC TECHNOLOGY
The twentieth century has seen the development of a series of new
technologies that have enabled physicians to see inside the human body. The
technologies began with X-Rays, and then CT scanners, PET scanners and MRI
scanners were developed. These technologies all allowed physicians to see
inside the body from the outside while other technologies such as endoscopy
allowed physicians to invade the body with tiny cameras to observe the state of
the interior of patients bodies.
X-Rays were first discovered by Wilhelm Roentgen in 1895. Roentgen was
experimenting with a Crookes tube, a glass tube with the air removed to create
a vacuum and with electrodes to allow the production of an electric current
within the tube. The electric current, consisting of a stream of electrons
known as cathode rays, would cause phosphorescent material within the tube to glow.� When experimenting with a Crookes tube, the
German physicist, Phillip Leonard has noticed that cathode rays could travel
through an aluminium sheet he had placed over a window in the Crookes tube and
turn slips of paper covered with barium platinocyanide salts, fluorescent.
Lenard sent a Crookes tube to Roentgen for Roentgen to study the cathode rays.
Roentgen repeated Lenard�s experiments and found the cathode rays were escaping
from the Crookes tube just as Lenard had found. Roentgen thought that the
cathode rays might be passing through the walls of the Crookes tube as well as
through the aluminium covered window in the tube.
When conducting the experiment Roentgen noticed a screen coated with
barium platinocyanide, a yard away from the Crookes tube, turned fluorescent.
This could not be caused by cathode rays which only travel a few inches in the
air. Roentgen moved the screen further away from the Crookes tube and the
screen still turned fluorescent when he turned on the electric current in the
Crookes tube. Roentgen placed objects like a book and a deck of cards between
the Crookes tube and the screen and the screen still lit up when he turned on
the current in the Crookes tube. Further experiments revealed, that the ray
causing the screen to light up, could penetrate a wide range of materials such
as wood and flesh. Roentgen had no idea what the ray was so he called it an
X-ray. When a human hand was placed in front of a photographic plate and
exposed to X-rays, the plate showed the bones in the human hand. However, the
X-rays did not easily pass through metals and could not pass through lead at
all.
X-rays were found to have a
number of uses such as in crystallography, astronomy and in microscopic
analysis, but their most important use has been in medicine. X-rays can provide
a photograph of the inside of the human body. X-rays have a shorter wave length
than light so they can penetrate materials opaque to light. X-Rays can more
easily penetrate materials of low density such as skin and muscle, but cannot
penetrate materials of higher density, such as bone, bullets and kidney stones.
The use of x-rays in medicine was
greatly extended by the employment of contrasting media such as barium salts
and iodine solutions. Barium makes it possible to obtain x-rays of the large
and small intestine and the stomach and the oesophagus. Iodine allows an x-ray
picture of the kidneys and bladder and also the carrying out of angiographs.
Angiography provides a view of the blood within the arteries and veins which
will disclose blockages and other problems within the arteries and veins. The
use of catheters allows contrast materials to be injected into the heart
allowing x-rays of the internal structures of the heart. X-rays can be used to
detect tumours, cancers and cysts.
A further enhancement of x-ray
technology came with the development of CT or CAT scanners. The CT scanner uses
x-rays, photon detectors and computers to create cross section images or
tomograms of the human body. In 1963 Allan Cormack invented an improved x-ray
machine using computers, an algorithm and tomograms. In 1972 Godfrey Hounsfield
invented the CT or computerized tomography scanner. It allowed many x-rays to
be taken, from multiple angles of thin slices of the human body and detectors
opposite the x-ray tubes would collect the data, which was converted into
digital data, which was then converted by an algorithm, a set of mathematical
instructions, by a computer into x-ray pictures. The CT scanner could give
three dimensional views of the body and provides much better resolution than ordinary
x-ray images. It can show soft tissues and liquid parts of the brain and can
show tumours as small as one or two millimetres in size. CT scanners have gone
through a series of improvements involving various different generations of
scanners. In the earlier scanners the x-ray beam lacked the width and the
number of detectors to cover the complete area of interest requiring multiple
sweeps to produce a suitable image. In subsequent scanners a wider x-ray beam
and more detectors were used to shorten scanning times.
Endoscopy, also known as
laparoscopy, involves inserting an instrument into the body either through the
body�s natural entrances or through a small hole surgically cut in the body.
The instrument is used to observe the internal structures of the body and can
also be used for surgery with tiny instruments at the end of the endoscope
being manipulated by the surgeon through the endoscope.
Endoscopy goes back to the late
nineteenth century but was not widely used as the views it provided of the interior
of the body were too poor for practical use. Harold Hopkins, a physicist, heard
about the problems with endoscopes and remembered that although light normally
travelled in a straight line it could in certain circumstances be made to
travel around corners by the use of curved glass. Hopkins considered that tens
of thousands of flexible glass fibres operating together may be able to cause
light to go around corners. He made an experimental endoscope and published his
results in 1954. Basil Hirschowitz, a South African, working in the United
States, read about Hopkins ideas and created his own endoscope. Several hundred
thousand fibres were wound together and to stop light jumping from one fibre to
another which could cause the loss of the image a technique of coating each
fibre with a glass coating was developed. The endoscope allowed investigation
of much of the interior of the body and some surgery on the interior of the
body without having to make substantial incisions into the body.
Photography through an endoscope
was not very satisfactory due to inadequate illumination and because the
optical system was not good enough. Hopkins investigated the problem and found
that an endoscope consisting of a glass tube containing thin lenses of air gave
improved light transmission around eighty times stronger than conventional
endoscopes made of an air tube containing thin lenses of glass. This allowed
the taking of photographs through the endoscope and allowed greatly expanded
surgical possibilities through the endoscope. Endoscopy can be used for surgery
by instruments such as lasers or wire loop cautery devices attached to the head
of the endoscope and controlled by the surgeon through the endoscope.
1.3.9
MODERN SURGERY��������������������������������������������������������������������������������������������
(back to content)
Surgery, before the introduction
of anaesthetics and anti-septic and aseptic practises, was limited to a narrow
range of operations, of which limb amputation was by far the most common. The
quickest operations only were possible without anaesthetics and the mortality
rates from infection were enormous before anti-septic practices were
introduced. The introduction of gowns, masks, rubber gloves and the
sterilization of instruments dramatically cut the death rate in surgery.
Abdominal surgery only became
possible with anaesthetics and anti-septics. Christian Billroth (1829-94)
pioneered operations in this area. Operations to remove the appendix and to
close a perforated gastric ulcer began to be performed in the late 19th
century. Brain surgery began with Sir William Macewan (1848-1924) in Glasgow
and Macewan also developed operations to deal with bone diseases such as
rickets.
Plastic surgery was to make great
progress in the 20th century, two New Zealanders Harold Gilles and Archibald
McIndoe leading the way. Plastic surgery dates back to ancient times and was
practiced in pre-British India and Renaissance Europe when it was used to deal
with the terrible damage caused by syphilis. During World War I Harold Gilles
carried out plastic surgery on the badly disfigured faces of soldiers and
sailors. He developed an operation whereby a skin flap was sliced from the
upper arm, one end of the flap remaining attached to the arm and the other end
was moulded over the nose and then sewn down. After several weeks the skin sewn
to the face would take and the skin attached to the arm could be cut and sewn
into place on to the face. When the injured had no facial skin at all Gilles
took the flap of skin from the abdomen rolling it over the chest and sewing one
end to the face. Holes would be cut in the skin for the nose, eyes and mouth.
When that end had taken Gilles cut the end still attached to the abdomen and
then sewed that into place on the face. This system involved two operations as
if the skin was completely removed from the donor area before it had taken on
the face it would die due to lack of blood supply. These techniques were
further developed by Archibald McIndoe while operating on air force pilots
injured in World War II.
The first experiments with organ
transplants had been made by Alexis Carrel early in the 20th century. He
carried out various transplant operations on animals discovering the problem of
rejection where the transplanted organ was rejected by the receiving animal�s
body. The problem of rejection was investigated by Peter Medawar when he
observed skin drafts taken from a donor would last for ten days before
rejection, while a subsequent skin draft from the same donor was instantly
rejected. When the body suffers an infection from bacteria or viruses initially
it takes time to identify the invading organism before the immune system
attacks the invading organism. In the event of a subsequent attack by the same
organism the organism is immediately attacked because the immune system recognizes
it as foreign material due to its previous contact with the virus or bacteria.
The way in which the first rejection takes some time but a second rejection of
the same material occurs immediately led Medawar to realize that it was the
immune system rejecting the transplant in the same way as it attacked invading
bacteria and viruses.
Organ transplant required a
practical surgical technique which was developed by Joseph Murray who improved
on techniques experimented with by Alexis Carrel on animals. The technique
involved the sewing together of small blood vessels which allowed the attaching
of the transplanted organs blood supply to those of the recipient so that it
could receive the receipts blood. The first attempts at organ transplant were
kidney transplants. This was because humans had two kidneys, but only need one
so living donors were readily available. Kidney transplants were also
relatively straight forward operations the main job being to connect the
transplanted organs blood supply to the recipient�s blood supply.
Kidney transplants did however
require the prior invention of the kidney dialysis machine. The dialysis
machine was invented by Wilhelm Kolff, a Dutch physician in 1941. The dialysis
machine performs the work of the kidneys when the kidneys fail. This mainly
involves removing waste material from the blood. The dialysis machine is needed
during transplants to keep people alive before the operation and for a period
of time after the operation, often ten days or so, until the donated kidney
begins to work.
A workable surgical technique and
the dialysis machine allowed kidney transplants to be performed and the first
operation was performed in 1954 by Joseph Murray on a patient whose identical
twin supplied the donated kidney. The operation was a success with no rejection
problems as the donated kidney came from an identical twin so that the
recipient�s immune system did not treat the donated kidney as foreign material.
When however, kidney transplants were attempted using close relatives as
donors, the donated organs were rejected by the recipient�s immune system
resulting in the death of the recipient.
A drug, known as 6-mp, had been
developed by George Hitchings and Gertrude Elion as a treatment for leukaemia.
6-mp worked by stopping the cancer cell from dividing by appearing to be a
chemical necessary for the cancer cells division, but which was slightly
different so that it stopped the cancer cell from dividing and so killed the
cancer cell. 6-mp was tried to stop the immune system rejecting transplanted
organs by stopping the division of cells in the immune system. 6-mp was tried
on rabbits and found to stop the rabbit�s immune system attacking foreign
material, but leaving the rabbits immune system otherwise working. Hitchings
and Elion also developed a new drug azathioprine that was an improved version
of 6-mp. Azathioprine was tried on people but with poor results until high
doses of steroids in short bursts were given to patients with the azathioprine.
This had the desired effect of preventing the immune system attacking the
transplanted organ while still leaving the immune system able to work against
ordinary infections. Eventually another drug cyclosporine was developed which
had the same effect and transplant operations for other organs such as the
lungs, liver, bone marrow and hearts were developed.
Improvements in medicine and
sanitation led to people living longer and an increasing exposure to the
diseases of old age. Arthritis became much more common in the twentieth century
than previously. Arthritis of the hip was particularly a problem causing
constant and serious pain to patients and greatly reducing mobility. The pain
was caused by the rubbing of bone against bone in the hip due to the erosion of
cartilage between the bones.
Some attempts had been made to
provide artificial hips in the 1930�s and 1940�s but none had been particularly
successful. A major difficulty was that the hip has to maintain the weight of
the body as well as being completely mobile.�
John Charnley looked at problem and came up with three innovations that
were to lead to a practical artificial hip. He redesigned the socket, he
cemented the artificial hip to the bones with acrylic cement and he lubricated
the joint first with Teflon and then when that failed with polyethylene.
Charnley�s new artificial hip was an outstanding success and the hip
replacement operation was to become a common operation in the late 20th
century.
The heart is the most complex
organ in the body and for the first half of the twentieth century surgeons did
not touch it believing that to do so would kill their patient. In the 1930�s
and 1940�s operations were carried out on the aorta and the pulmonary artery to
ease symptoms caused by heart problems, but the heart itself was not touched.
In the late 1940�s surgeons began to widen heart valves through a hole cut in
the wall of the heart while the heart was still working. However, much heart
surgery, known as open-heart surgery, was only possible with the heart being
stopped. If the heart was stopped some means of maintaining the blood supply to
the body was necessary or the patient would die. John Gibbon and his wife Mary
Hopkins began work on a machine that could perform the work of the heart and
lungs in the 1930�s. The machine needed to be able to add oxygen and remove
carbon dioxide from the blood and to pump the blood through the body. The
machine needed valves to ensure the blood all flowed in one direction and had
to use glass tubes as plastic had yet to be invented. The Second World War
delayed progress, but a heart-lung machine was created in the early 1950�s.
Early results were not promising but the machine was taken over and improved by
the Mayo Clinic. Donald Melrose, in England, and Viking Bjork, in Sweden, also
built similar machines to allow open heart surgery. The result was to be an
effective heart-lung machine that could take over the functions of the heart
and lungs during operations so as to allow surgery on the human heart.
(back
to content)
2.0 Analysis of the order of discovery in the history of medicine
The question of the origin of
infectious disease was in dispute for thousands of years, the matter not being
settled until the late 19th century. The earliest cultures and civilizations
considered the cause of diseases to be supernatural and the appropriate
remedies to be appeals to the Gods and magical incantations. Such beliefs were
perfectly reasonable based upon the knowledge available to our pre- historic
ancestors and to early civilizations. They had no awareness of bacteria,
viruses or other microscopic organisms. Given that beliefs in Gods were used to
explain other mysterious events, such as earthquakes, storms and volcanic
eruptions, the Gods were an obvious explanation of disease. Given also that
diseases can kill human beings, it would be reasonable to assume they are
caused by powerful beings, like Gods or powerful demons and evil spirits. As
the body automatically tends to repair itself, due to the immune system, it
must have appeared to our pre-historic ancestors that on occasions the magical
incantations and appeals to the Gods had worked. When the patient died the
death could be put down to the capriciousness of the Gods or the great power of
the evil spirit, rather than there being anything wrong with the treatment
used.
In the west, from the time of
Hippocrates, natural causes of diseases, such as the four humors theory, were
the favoured explanation, although supernatural explanations continued to find
acceptance. The same situation existed in China with natural causes of disease
such as inadequate or imbalanced Qi and Yin and Yang being considered to be the
causes of disease. A similar situation existed in India where a balance of the
three elements, air, bile and phlegm was required for good health. The Greek,
Chinese and Indian explanations of disease are quite similar all involving
imbalances in bodily substances and all acquired a status that made them
impervious to criticism and a block on innovation.
The presence of blood, urine,
vomit and diarrhoea clearly shows the body has many internal fluids. Vomit and
diarrhoea particularly seem to be present at times of sickness and recovery
often occurs after vomiting and diarrhoea so that it would appear that getting
rid of fluids from the body could cure sickness. Even bleeding was often
followed by recovery from injury so that a limited loss of blood could be seen
as promoting recovery. It is because the human body has these fluids and
because getting rid of the fluids with vomiting, diarrhoea and bleeding seemed
to cure sickness and injury, ideas such as an imbalance of fluids caused ill
health arose in Western, Chinese and Indian cultures. This gave rise to
theories such as Hippocrates and Galen�s four humors theory and to remedies
such as bleeding and purging. The Chinese theory of an imbalance between Yin
and Yang causing disease appears to be a more abstract version of the same
idea. Given the knowledge of non-scientific societies these theories make good
sense. A theory that micro-organisms, invisible to the naked eye, cause disease
is hardly credible for societies that have no evidence of the existence of the
micro-organisms. On the other hand, bodily fluids plainly do exist and their
removal from the human body seems to be associated with recovery from disease
and injury.
The medicine of Hippocrates and
Galen did not just relate to the four humors. It also dealt with qualities such
as hot, cold, dry and wet. This is because many of the symptoms of disease
relate to these qualities for example if a person has a temperature or fever,
they are hot, if they are perspiring, they are wet. If they do not have a
temperature, they are cold, if they are not perspiring, they are dry. Galen�s
theory was built up from the way the human body acts, both when it is sick and
when it is healthy. If the human body functioned in a different way, it would
have led to a different type of medical theory. If for example the human body
changed color when it was sick, rather than changing temperature, medical
theory would likely involve explanations and treatments that involve colors
with the aim of restoring the patient to his or her normal healthy color.
The traditional Chinese theory of
medicine has considerable similarities to the classical theories of Galen. The
western idea of pneuma, a vital spirit taken into the body by breathing, is
similar to the Chinese concept of Qi. Galen�s theory of the four humors
considers much sickness is caused by an imbalance in the body fluids. The
Chinese theory also deals with body fluids, known as JinYe. A healthy person
will have the body fluids in balance, but if the body fluids are deficient, or
if there is an accumulation of fluids, sickness can result. A further
similarity between Galen�s humoral theory and the Chinese theory is that the
Chinese theory of Yin and Yang, like the humoral theory considers sickness is
caused by imbalances within the body. The Chinese theory of blood also
emphasizes that imbalances can cause sickness. Given that Yin and Yang, body fluids
and blood should all be in balance to avoid sickness in Chinese medical theory,
it has considerable similarities with Galen�s humoral theory which considers
sickness is caused by imbalances in the four humors. In both the humoral theory
and traditional Chinese medicine the weather could cause imbalances in body
fluids.
A further similarity between
Galen�s theory and traditional Chinese medicine concerns the elements. Galen�s
theory uses the idea of the four Greek elements, air, fire, earth and water. Each
element is associated with a particular organ, a particular humor and with the
qualities of hot, cold, dry and wet. Water for example is associated with the
organ, the brain, the humor phlegm and the qualities of cold and wet.
Traditional Chinese medicine uses the Chinese elements of fire, earth, water,
wood and metal. The elements are each associated with organs, one of which is a
Yin organ and the other a Yang organ. Water for example is associated with the
bladder and the kidney, while earth is associated with the stomach and the
spleen. The elements are all interconnected so that if one of the organs and
its element is in a state of imbalance, it will affect the other elements and
their organs. This could affect the individual�s facial color and emotional
state as well as the functioning of the relevant organs. The Western and
Chinese theories of medicine were so similar, because each was derived from the
same source. The source was the human body and the environment that could
affect the human body. If the human body and the environment were different the
theories would be different.
The naturalistic and supernatural
explanations of disease co-existed for thousands of years, sometimes with one
dominant, and at other times, the other being the more powerful. Neither was
more convincing than the other, in that both sometimes appeared to work and
that both sometimes failed to work. When they failed to work, both the
supernatural and naturalistic theories provided explanations for the failure.
If the human body did not have an immune system, so that if a person got sick
they inevitably died and the incantations to the Gods and the treatment
provided by doctors never worked, then the supernatural and naturalistic
explanations of disease and the treatments they gave rise to would never have
existed. It is only because the human body fights against disease, often
successfully, that the incantations to the Gods and doctor�s treatments often
appeared to be successful which suggested that the explanations of disease were
true and the treatments provided were sometimes working. Both the supernatural
and naturalistic explanations of disease could have been proved wrong with
modern double blind testing, but such testing was not done in the past because
it required knowledge of sophisticated statistical techniques that only became
available in the last 400 years. Even in the 18th century the English and
French were unable to agree as to whether smallpox inoculation was desirable,
while in the first half of the 19th century Pierre Louis conducted trials which
showed bleeding was a useful treatment. Even today, drug trials sometimes
produce contradictory results. Even if testing had been done the theories would
probably have survived due to the lack of serious alternatives.
It was not until the late 19th
century with the development of the germ theory of disease that the question of
the origin of infectious disease was settled in favour of a naturalistic
theory, but a theory completely different from any of the naturalistic theories
previously accepted. When Fracastorius in the 16th century suggested contagious
disease was caused by tiny seeds invading the human body, the theory was quite
reasonably not accepted, as there was no evidence of the existence of the tiny
seeds, or that they caused disease. Fracastorius theory was almost identical to
the germ theory of disease and the germ theory was only accepted in the late
19th century with the work of Pasteur and Koch. Leeuwenhoek had discovered
micro-organisms in the late 17th century but that did not mean that they caused
disease. In fact, the vast majority of micro-organisms do not cause disease in
humans. It was only with the more powerful 19th century microscopes that
Pasteur and Koch were able to discover particular organisms which caused
particular diseases in humans. They were able to show the organisms were the
causes of the disease by isolating the organisms and by preparing a pure
culture of the organism, which in the case of animals would then be injected
into an animal causing the disease in the animal. This procedure known as
Koch�s postulate established the germ theory of disease and was able to show
which particular germs caused which disease.
The explanations of infectious
disease were based upon the knowledge available to a society at a particular
time. When that knowledge changed (the discovery of micro-organisms and the
discovery that some of them cause disease) the explanations of disease changed.
Societies that considered the activities of supernatural beings as explaining
otherwise inexplicable phenomena used supernatural explanations for the cause
of infectious diseases. Supernatural explanations and naturalistic explanations
of disease co-existed for thousands of years. Each was as convincing as the
other until the germ theory of disease arose in the late 19th century.
Naturalistic explanations of disease were based upon the natural world, and in
particular, on the human body itself. Body fluids, organs and the elements of
the natural world all had a prominent role in both Western and Chinese
naturalistic explanations of disease.�
The Chinese and Western
explanations of disease were similar because they had similar knowledge of the
natural world and of the human body, so they developed similar theories to explain
the origin of disease. If the natural world and the human body were different,
then the theories explaining disease would have been different. When human
knowledge of the natural world increased, with the discovery of micro-organisms
in the 17th century and the discovery in the late 19th century that some of
those micro-organisms caused disease in humans, the theories explaining the
causes of disease changed. The germ theory of disease became the accepted
explanation of infectious disease throughout the western world. The practice of
immunization (the modern name for vaccination, also known as inoculation) has
been one of the most successful medical practices in history. It has been
responsible for an enormous reduction in human suffering and has saved an
enormous number of human lives. The injection of dead bacteria or their toxins,
or dead or weakened viruses into the human body to create immunity against
disease, has eliminated or controlled a considerable range of diseases.
Immunization has been used successfully against anthrax, bubonic plague,
chicken pox, cholera, diphtheria, Haemophilus influenza type B, mumps,
paratyphoid fever, pneumococcal pneumonia, poliomyelitis, rabies, rubella
(German measles), Rocky Mountain spotted fever, smallpox, tetanus, typhoid,
typhus, whooping cough and yellow fever.
Immunization works because the
body�s natural defenses against infection are able to remember dangerous
bacteria and viruses they have already had contact with and are able to react
more quickly and more strongly to later infections from the same organism. When
an infection occurs certain cells in the body respond by moving to destroy the
invading bacteria or viruses. In order to destroy the invading bacteria or
viruses the body�s immune system, a collection of free moving cells, has to
recognize which materials in the body are foreign invaders and what is part of
the body. It does this by matching the shape of receptors on the surface of
defending cells to the shape of the surface of the invading organism and if
they fit together the defending cells recognizes an invading organism. Once
recognition of an invader has taken place other defending cells will attack and
destroy the invading organisms. The defending cells can also produce memory
cells which, in the event of a future invasion by the same organisms, are able
to immediately clone large numbers of the appropriate defending cells to attack
the invading organism, without having to go through the process of recognizing
the invading organism.
This makes the immune systems
response to invading organisms, which it has recognized before, much stronger,
faster and more effective. This process known as the amplification of the
response is the basis for immunization. A dead or greatly weakened infectious
organism is injected into the human body so that the defending cells will
remember the organism, so that in a future attack the immune system does not
have to go through the recognition process and can immediately attack the
invading organisms with large numbers of cloned defending cells. If the body
did not work in this manner, for example if it did not produce memory cells
which instantly recognize invading organisms, the process of immunization would
not work. This would mean that the wide range of diseases immunization is
effective against would still be killing vast numbers of people.
Smallpox was the first infectious
disease to be treated with immunization, partly because it was one of the worst
and most persistent diseases in history and partly because nature provided a
ready-made immunizing material, in the form of cowpox, which saved people from
having to identify, isolate and produce a safe vaccine. The high mortality rate
from smallpox and the observation that survivors were protected from future
attacks, which could only be observed with a disease which was continually or
often present made smallpox the obvious disease to immunize against. A disease
which came and then disappeared often for centuries is a less urgent case to
immunize against as it may well not come back for centuries making immunization
unnecessary. Given that smallpox was often or continually around it made sense
to immunize against it. It also made it more easily observable that survivors
were protected against future attacks. This was not so easily observable with
diseases which involved major epidemics and then disappeared for long periods
of time, so there were no future attacks from which the victims of earlier
attacks could be shown to be immune. However early attempts at variolation were
so dangerous, that it is not surprising that it never really caught on.
The reason why smallpox was the
first disease effectively treated with immunization was because nature
provided, in cowpox, a ready-made vaccination material which was not dangerous
to human beings. To produce effective vaccines for other diseases it was
necessary to discover the bacteria or virus involved, to isolate it and to
reproduce it. This process enunciated in Koch�s postulates could only be done
with better microscopes than was available in the 18th century. It also needed
the understanding that germs cause infectious disease which was not established
until late in the 19th century by Pasteur and Koch. This understanding was not
needed for smallpox, where it could be empirically observed, even by milkmaids,
that the natural vaccine, cowpox, prevented smallpox.� With the other diseases it was necessary to
understand the germ theory of disease and then to artificially produce a vaccine
before it was possible to immunize against those diseases. The process of
immunizing against smallpox was a lot simpler than the process of immunizing
against other diseases, so immunization against smallpox occurred before
immunization against the other diseases.
The taboo on human dissection
applied in most human societies, except India, Ancient Egypt and Europe since
the Renaissance. The result was substantially erroneous beliefs concerning
human anatomy and physiology. Beliefs that the heart was the centre of thought,
sense perception and controlled bodily movements, while the brain cooled the
heart and blood held by Aristotle resulted from the taboo on human dissection.
When the taboo was not present, such as in Alexandria during the Ptolemaic era,
it was discovered, that the brain dealt with sense perception and bodily
movements. Further progress in anatomy and physiology was delayed until the
Renaissance when some dissections of the corpses of executed criminals was
allowed. This eventually resulted in the anatomical discoveries of Versalius
and the circulation of the blood by Harvey. Many future developments in
medicine, especially in surgery, were dependent upon the new knowledge of
anatomy and physiology obtained from the lifting of the taboo on human dissection.
Progress in surgery was also
dependent on the discovery of anaesthesia and anti-septic and a- septic
practices. There were two main consequences from the discovery of anaesthesia.
The first was that surgery became far more common as patients no longer tried
to avoid it. The second was that surgical operations became a lot longer with
emphasis being on precision and accuracy rather than on speed. With increasing
time being spent on operations more intricate and complex operations could be
performed which greatly widened the range of operations available. With much
longer operations and the need for anaesthetics and anaesthetists the cost of
operations went up as did the status of surgeons who were now able to do so
much more for their patients. Surgery became a practical solution to many medical
problems.
The idea that cleanliness was
important to stop infections in surgery and obstetrics was only accepted after
Pasteur had established the germ theory of disease which showed that bacteria
in the air caused infections. Prior to the germ theory of disease being
accepted suggestions that cleanliness was important, were ignored as there
seemed to be no reason why cleanliness could stop infection or lack of
cleanliness could cause infection. The discovery that infection was caused by
bacteria in the air, led to the anti-septic idea of killing the bacteria to
stop infection and then to the a-septic idea of sterilising everything that
came in contact with the patient.
The ending of the taboo on human
dissection resulted in vastly improved knowledge of anatomy and physiology,
this, and the discovery of anaesthesia and the realisation of the importance of
a-septics, formed the basis of modern surgery. Only when these developments
came together, was it possible for modern surgery, with its sophisticated and
intricate operations, to become a reality. This led to new types of surgery
which had never before been developed such as abdominal and brain surgery.
Plastic surgery, which had been practiced crudely in the past, improved
enormously and later led to cosmetic surgery. Hip replacement operations were
developed after the invention of a practical artificial hip. Organ transplants
began when surgical techniques were developed for joining small blood vessels
and when the problem of rejection of donated organs was solved by the
development of appropriate drugs. Kidney transplants developed rapidly after
the invention of the kidney dialysis machine as it is a relatively simple
operation and because there is a better supply of donated kidneys as human
beings have two kidneys and only need one so as to allow transplants from
living donors. Open heart surgery and heart transplants were developed after
the invention of the heart-lung machine to keep the patient alive during surgery.
The use of anti-biotics in
medicine is only possible because nature provides such organisms that inhibit
the growth of bacteria and allows the production of synthetic compounds that
achieve the same result. If nature did not provide these organisms, or allow
such compounds, there would have been no anti-biotics used in medicine. Without
anti-biotics, medicine since the 1940�s would have been much less effective and
hundreds of millions, who were cured of infections, would have died. The
discovery and use of anti-biotics was impossible before the development of
microscopes capable of observing bacteria. Only when such microscopes existed
was it possible to observe that certain organisms were capable of killing or
inhibiting bacteria. A number of such observations were made in the late 19th
and early 20th century and eventually it was realised that penicillin, a
substance taken from one of those bacteria killing organisms, could be used
against infectious disease. When penicillin was proved to be effective, a
systematic search was made for other anti-biotics which resulted in the
discovery of a number of other anti-biotics. However, it was only because
nature has provided the anti-biotics that we have them, and we have only had
them, since we acquired the knowledge of their existence and of how to use
them.
The use of statistics in medicine
has been of enormous use in showing the causes of disease and in assessing the
effectiveness of treatments. Yet statistics are never able to provide a perfect
answer to questions of drug effectiveness and the causation of disease. They
may show a co-relation between two variables, for example people living close
to the sea have higher rates of cholera, than people further from the sea. This
does not however mean that proximity to the sea causes cholera. Co-relation
does not prove causation as the correlated variable may be caused by a third
factor, such as polluted river water which is more common closer to the sea.
The third factor, often called a lurking variable, may well not be considered
in the data so no effort is made to compare cholera rates among people drinking
polluted water close to the sea with those drinking clean water close to the
sea. If the comparison was made it would show that it was the quality of drinking
water rather than proximity to the sea that was the important variable
concerning cholera rates. When trying to discover the cause of increasing lung
cancer after World War II, air pollution and asphalting of roads were
considered likely causes as both were increasing at the time lung cancer rates
were increasing. Working out, which variable to study, when trying to discover
the causes of disease, can be very difficult.
A further problem concerns trying
to ensure the chosen sample is representative of the population which is being
studied. Pierre Louis concluded bleeding was a useful treatment, but one of the
groups he studied was substantially younger than another group. The sample must
also be of sufficient size or simple co-incidence and high margins of error may
provide misleading results. Pierre Louis� study of bleeding was criticized for
having insufficient numbers in his sample.
Given the difficulties of doing
good statistical studies it is not surprising that the causes of diseases and
the effectiveness of treatments were never accurately assessed until recently. Modern
statistical methods were only developed in the 17th, 18th and 19th centuries
and arose from probability theory. It was only with the development of modern
statistical methods that it has been possible to identify the causes of many
diseases and to evaluate the effectiveness of treatments. Even with modern
statistical methods the causes of some diseases, for example some cancers, are
still difficult to pinpoint. Often different studies of the same phenomena will
produce different results. In these circumstances it was impossible for people
in the past to discover the effectiveness of treatments and the real causes of
disease until the discovery of modern statistical analysis.
Modern diagnostic technology
began with the discovery of X-rays. X-rays however could not be discovered
until certain earlier discoveries had been made. X-rays were discovered through
the use of a Crookes tube which required prior discoveries of an efficient air
pump to create a near vacuum in the tube and the ability to send an electric
current through the tube. Only when these discoveries had been made was it
possible to discover X-rays. The use of X-rays was eventually improved and
extended by the use of contrasting media and eventually by CT scanners after
the invention of computers.
X-rays are a form of
electro-magnetic energy and are useful due to their property of being able to
pass through matter of low density but not matter of high density. This allows
X-rays to be used to produce photographs of the interior of the human body,
which is why X-rays are so useful in medicine. It is only because nature has
provided such a form of electro-magnetic energy that we have X-rays available
to be used for medical diagnosis. If nature had not provided electro-magnetic
radiation with that property, we could not have the ability to see inside the
human body for medical purposes by means of X-rays.
Endoscopy only became practical
when Hopkins and Hirschowitz discovered a practical method to make light travel
around corners. It was only because such a method exists that we are able to
have modern endoscopy, and modern endoscopy could not exist until the discovery
of how to make light travel around corners. Endoscopy was further enhanced when
Hopkins discovered that thin lenses of air gave much greater light transmission
than thin lenses of glass, so as to allow much better endoscope photography. If
such lenses did not provide improved light transmission, then endoscope
photography might still not be practical.
Our brief examination of the
history of medicine has shown how the environment relevant to medicine has
affected the history of medicine. The relevant environment includes the human
body, how the human body works, the diseases that attack the human body, how
the materials in the environment affect the human body and how the body reacts
to disease and injury. If the human body was different then the history of
medicine would have been different. If, for example, there was no immune
system, then a lot of the confusion concerning the effectiveness of treatments
used in the past would not have existed. When patients treated with prayers,
incantations, herbs, medicines, moxabustion and bleeding recovered, it looked
as though the treatment had worked. If patients died all the time, as they
would have if there was no immune system, it would have been clear all these
treatments were failing and they would have been abandoned. If there was no
immune system then modern treatments such as immunization would not work and
would not be available. If the human body was different, the theories as to
what went wrong with it when people got sick would have been different. Galen�s
humoral theory and traditional Chinese theories were based on the human body
and how it behaved in sickness and in health. If the body was different then
those theories would have been different.
Anaesthesia was only possible as
materials in the human environment had the property of making people so
unconscious that they could not feel pain. X-rays were only possible as
electro-magnetic energy of a certain wave length will pass through matter of
low density but not matter of high density. Modern endoscopy is only possible
because light can be made to travel around corners and thin lenses of air
provide excellent light transmission. The use of anti-biotics is only possible
due to bacteria killing organisms existing in the human environment and the
ability to create compounds that will kill bacteria. The properties of materials
and matter and forms of energy in the environment determine what is possible in
medicine.
When knowledge of the environment
relevant to medicine changed, this resulted in new theories, such as the brain
being the centre of thought and emotions rather than the heart, the circulation
of the blood and the germ theory of disease. These ideas were the logical
explanations of the new knowledge that human beings had acquired, just as the
previous theories were the logical explanations of the knowledge humans possessed
at those times.� Increasing knowledge of
the environment, relevant to medicine, also led to the development of new
treatments such as anaesthetics and new drugs. The new theories and treatments
inevitably had significant social and cultural consequences, such as greater
life expectancy, reduced suffering and different attitudes concerning religious
beliefs, all of which would themselves result in further social and cultural
consequences.
Where taboos existed against the
acquisition of new knowledge, such as the taboo on human dissection, then the
acquisition of new knowledge will be delayed until the taboo is removed. This,
in the case of medicine, meant erroneous ideas of human anatomy and physiology
continued for as long as the taboo remained in place.� Only after the taboo was lifted was it
possible to make the anatomical discoveries of Versalius and for Harvey to
discover the circulation of the blood.
(back
to content)
2.1
The Origins and History of Medical Practice with Fundamentals of Medical
Practice Management g
LIFELONG LEARNING
Practice management is changing
rapidly in response to the ever-changing landscape of healthcare and the
medical practice. Practice managers need to be committed to lifelong learning
and be active in our professional organizations to ensure they are up-to-date
on current knowledge.
The Medical Group Management
Association (MGMA), with its academic arm, the American College of Medical
Practice Executives (ACMPE), is the premier practice management education and
networking group for practice managers. The organization dates back to 1926 and
represents more than 33,000 administrators and executives in 18,000 healthcare
organizations in which 385,000 physicians practice. MGMA (2016a) has been instrumental
in advancing the knowledge of practice management, and ACMPE offers a rigorous
certification program in practice management that is widely recognized in the
industry.
ACMPE has identified eight areas
that are essential for the practice manager to understand (exhibit 1.1).
This text examines each of these
domains of the practice management body of knowledge to provide a sound,
fundamental base for practice managers and practice leaders. It includes a
comprehensive overview that does not assume a great deal of prior education in
the field of practice management. Furthermore, it seeks to provide not only
specific information about the management of the medical practice but also
context in the larger US healthcare system. Too often, different segments of
the healthcare system see themselves as operating in isolation. This point of
view must change if medical practices are to transform and if managers are to
lead successful practices in the future, whether a small, free-standing
practice or a large practice integrated with a major healthcare system.
Another prominent organization
for the education and advancement of practice management is the American
College of Healthcare Executives (ACHE). ACHE is a professional organization of
more than 40,000 US and international healthcare executives who Certification
A voluntary system of standards
that practitioners meet to demonstrate accomplishment or ability in their
profession. Certification standards are generally set by nongovernmental
agencies or associations.
|
Business operations
|
Financial management
|
|
Human resource management
|
Information management
|
|
Organizational governance
|
Patient care systems
|
|
Quality management
|
Risk management
|
Source: MGMA (2016b).
Exhibit 1.1
THE EIGHT DOMAINS OF THE BODY OF KNOWLEDGE FOR PRACTICE
MANAGERS
Natural healthcare systems,
hospitals, and other healthcare organizations. Currently with 78 chapters, ACHE
offers board certification in healthcare management as a Fellow of ACHE, a
highly regarded designation for healthcare management professionals (ACHE
2016).
THE AMERICAN HEALTHCARE SYSTEM
The practice of medicine drives
the US healthcare system and its components, and medicine is heavily influenced
by the system as well. Medical practice and the healthcare system both are
built on the foundation of the physician�patient relationship. Although the
percentage of total healthcare costs attributed to physicians and other
clinical practitioners was 20 percent in 2015, the so-called clinician�s pen,
representing the prescribing and referral power of medical practice clinicians,
indirectly accounts for most healthcare system costs.
Administrators do not prescribe
medication; admit patients, or order tests and services. This fact is just one
illustration of a fragmented system whose segments can act independently.
This fragmentation must be
addressed if medical practices are to provide high-quality healthcare to
patients at the lowest cost possible.
To begin our study of practice
management, the book first offers some perspective of medical practices in
terms of the overall US healthcare system. A complete history of the practice
of medicine is beyond the scope of this text, but the lengthy and enduring
nature of medical practice is important to recognize. The first known mention
of the practice of medicine is from the Old Kingdom of Ancient Egypt, dating
back to about 2600 BC.
BEHAVIOR
How an individual acts,
especially toward others.
Later, the first known code of
conduct, the Code of Hammurabi, dealt with many aspects of human behavior and,
most importantly for our study, established laws governing the practice of
medicine. The first medical text was written about 250 years later (Nunn 2002).
Exhibit 1.2 provides a sample of
some significant points in the development of the physician medical practice
from ancient times to the present. The reader may wonder why such a diverse
series of events is listed, ranging from the recognition of the first physician
to the occurrence of natural disasters and terrorist acts. Medicine, whether
directly or indirectly, influences virtually every aspect of human life. Events
such as Hurricane Katrina, the 9/11 terrorist attacks, the emergence of the
human immunodeficiency virus (HIV), and the Ebola virus outbreak have had major
impacts on the healthcare system and physician practice. Before 9/11, medical
practices thought little about emergency preparedness and management; such
activities were seen as under the purview of government agencies. Until HIV was
identified in 1983 as the cause of acquired immunodeficiency syndrome (AIDS),
and reinforced by the Ebola crisis of 2014, medical practices spent few
resources and little time thinking about deadly infectious disease and the
potential for it to arrive from distant locales. A traveler can reach virtually
any destination in the world within a 24-hour period, which is well within the
incubation period of most infectious agents. Modern air travel has made the
world of disease a single place, so practices must be mindful of patients�
origins and travels.
Exhibit 1.2
SELECTED MAJOR EVENTS IN THE HISTORY OF MEDICINE AND MEDICAL
PRACTICE
2600 BC: Imhotep is a famous doctor and the first physician
mentioned in recorded history. After his death he is worshiped as a god. (Hurry
1978)
1792�1750 BC: The Code of Hammurabi is written, establishing
laws governing the practice of medicine. (Johns 2000)
1500 BC: The Ebers Papyrus is the first known medical book.
(Hinrichs�sche, Wreszinski, and Umschrift 1913)
500 BC: Alcamaeon of Croton in Italy says that a body is
healthy as long as it has the right balance of hot and cold, wet and dry. If
the balance is upset, the body falls ill. (Jones 1979)
460�370 BC: Hippocrates lives. He stresses careful
observation and the importance of nutrition. (Jones 1868)
384�322 BC: Aristotle lives. He says the body is made up of
4 humors or liquids: phlegm, blood, yellow bile, and black bile. (Greek
Medicine.net 2016)
130�200 AD: Roman doctor Galen lives. Over following
centuries, his writings become very influential. (Sarton 1951)
12th and 13th centuries: Schools of medicine are founded in
Europe. In the 13th century, barber-surgeons begin to work in towns. The church
runs the only hospitals. (Cobban 1999; Rashdall 1895)
1543: Andreas Vesalius publishes The Fabric of the Human
Body. (Garrison and Hast 2014)
1628: William Harvey publishes his discovery of how the
blood circulates in the body. (Harvey 1993)
1796: Edward Jenner invents vaccination against smallpox.
(Winkelstein 1992)
1816: Rene Laennec invents the stethoscope. (Roguin 2006)
1847: Chloroform is used as an anesthetic by James Simpson.
(Ball 1996)
1865: Joseph Lister develops antiseptic surgery. (Bankston
2004)
1870: The Medical Practice Act is passed. Licensure of
physicians becomes a state function. (Stevens 1971)
1876: The American Association of Medical Colleges is
founded. (Coggeshall 1965)
1880: Louis Pasteur invents a cure for chicken cholera, the
first vaccine. (Debr� 2000)
Exhibit 1.2
SELECTED MAJOR EVENTS IN THE HISTORY OF MEDICINE AND MEDICAL
PRACTICE
1895: Wilhelm Conrad R�ntgen X-rays are discovered. (Glasser
1933)
1910: The Abraham Flexner report on medical education is
published. (Flexner 1910)
1928: Penicillin is discovered by Scottish scientist
Alexander Fleming, and it is established that the drug can be used in medicine.
(Ligon 2004)
1929: The first employer-sponsored health insurance is
created at Baylor Teachers College as Blue Cross. (Buchmueller and Monheit
2009)
1931: The electron microscope is invented. (Palucka 2002)
1943: Willem Johan Kolff invents the first artificial kidney
(dialysis) machine. (Heiney 2003)
1951: Epidemiology studies identify cigarette smoking as a
cause of lung cancer. Sir Richard Doll is the first to make this link. (Keating
2009)
1953: Jonas Salk announces he has developed a vaccine for
polio. (Koprowski 1960)
1953: The structure of DNA is determined. (Dahm 2008)
1965: Medicare and Medicaid are passed into Law. (Social
Security Administration 2016)
1967: The first heart transplant is performed by Christiaan
Barnard. (Barnard 2011)
1971: MRI scanning is invented. (Lauterbur 1973)
1973: The HMO Act is passed. (Dorsey 1975)
1989: President George W. Bush signs the Omnibus Budget
Reconciliation Act of 1989, enacting a physician payment schedule based on a
resource-based relative value scale. (AMA 2017)
1996: The Health Insurance Portability and Accountability
Act is passed as an amendment to the HMO Act. (Atchinson and Fox 1997)
2001: The 9/11 terrorist attacks occur. (Bernstein 2003)
2003: The human genome is sequenced. (National Human Genome
Research Institute 2010)
2005: Hurricane Katrina devastates the Gulf Coast, including
New Orleans. (Knabb, Rhome, and Brown 2005)
2008: The Triple Aim for healthcare delivery is proposed by
the Institute for Healthcare Improvement. (Berwick, Nolan, and Whittington
2008)
Exhibit 1.2
SELECTED MAJOR
EVENTS IN THE HISTORY OF MEDICINE AND MEDICAL PRACTICE
2008: Medicare Part D is enacted. (Hargrave et al. 2007)
2010: The Affordable Care Act is passed. (HHS 2010)
2012: High-deductible health plans become more common. (Bundorf
2012)
2014: The Ebola crisis emerges in West Africa. (CDC 2014)
2016: Zika virus becomes a serious health threat. (CDC
2016b; Wang and Barry 2016)
The evolution of medical
practices has coincided with and been driven in part by the development of medical
technology and the scientific revolution. Medicine was limited in scope and
primitive until the middle of the nineteenth century. Theories of disease were
arcane, and diagnostic tools were largely absent (Rosenberg and Vogel 1979).
Prior to 1850, medical education
constituted an apprenticeship that was inconsistent and poorly preceptored,
with no standard curriculum (Rothstein 1972). Procedures focused on expelling
the disease with bleedings and emetics. Surgery was limited because of the lack
of anesthesia, and as a result, being fast was better than being good. Patients
often directed the physician as to the care they should receive. One might say
early medical practice was the first iteration of patient-centered care (Burke
1985).
PRACTICE MANAGEMENT RESOURCES
Accounting
A system for keeping score in business, using dollars.
Now, however, the amount of
information available about medicine and medical practice management is
virtually endless, representing many points of view; ideas; political world
views; notions about funding and access; and the numerous disciplines in the
broader management field, such as accounting, finance, human resources
management, organization development, and logistics. With the vast expanse of
knowledge available, students of healthcare and practice management are
encouraged to develop lifelong learning skills.
The field is changing so rapidly
that the need for continuous updating of knowledge and skills is essential.
For example, practice managers
need to build a virtual library of accurate and reliable sources. The list that
follows comprises the foundation of that library, which should be referred to
frequently (see the appendix to this text for each resource�s website):
◆ Centers for Medicare &
Medicaid Services (CMS)
◆ Advisory Board
◆ Dartmouth Atlas
◆ National Committee for
Quality Assurance
◆ Institute for Healthcare
Improvement
◆ Institute of Medicine
◆ Institute for Health
Policy and Innovation
◆ Kaiser Family Foundation
◆ Robert Wood Johnson Foundation
◆ Annenberg Foundation
◆ Commonwealth Fund
◆ Centers for Disease
Control and Prevention
◆ Agency for Healthcare
Research and Quality
THE DIMENSIONS OF MEDICAL PRACTICE
Governance
A system of policies and procedures designed to facilitate
oversight of the management of the enterprise.
Serves as the foundation of how the practice will behave,
compete, and document its actions.
Medical practices can take many
forms, ranging from small sole proprietorships to large multispecialty medical
practices. Recent years have seen more medical practices embedded in large
healthcare organizations, which also may be solo practices or large
multispecialty entities (see exhibit 1.3).
A group practice is defined as a
medical practice consisting of two or more practitioners working in a common
management and administrative structure. Single-specialty groups are those that
focus on one aspect of medicine, such as general surgery, family practice,
orthopedics, cardiology, or internal medicine. Multispecialty medical groups
contain more than one medical specialty in the organization. Multispecialty
practices are highly integrated, with a common governance leadership and common
management structure, and they have a highly developed corporate system for
managing finances and dealing with regulatory agencies. Their operation and
function are much more complex than solo or small practices.
GOAL
A specific target that an individual or a company tries to
achieve.
Integrated delivery systems
(IDSs) are networks of healthcare organizations under a single holding company
or parent organization that contain multiple components of healthcare delivery.
An IDS often includes hospitals, physicians and other clinicians, and payment
organizations, often referred to as third-party payer organizations. The goal
is to provide as complete a continuum of care as possible.
Exhibit 1.3
PRACTICE
STRUCTURES�SIMPLE TO COMPLEX
Solo Practice � Group Practice � Integrated System��
TYPES OF PRACTITIONERS
Physicians have, of course,
played a pivotal role in the US healthcare system since its inception.
Physicians�and now, other non-physician providers such as nurse practitioners
(discussed later)�care for patients by
◆ assessing the patient�s health status,
◆ diagnosing the patient�s condition, and
◆ prescribing and performing
treatment.
It has been said that the most
expensive instrument in the healthcare industry is the provider�s pen. An
amusing statement, it also carries a lot of truth because all diagnostic and
surgical procedures as well as office-based and hospital-based assessments�in
fact, all care in general�is either performed or ordered by a provider.
Furthermore, the medical practice
is unlike any other organization in the medical field because the nature and
identity of the practice is closely linked to the individual providers in the
practice. The providers are the primary producers and the primary governance
body, and they are held accountable for the performance of the practice in a
personal way. Their income is directly tied to the practice�s performance, more
closely than for other medical field workers. Exhibit 1.4 shows the fundamental
components of a medical practice.
Often, the challenge in practice
management is to serve the interests of the providers while maintaining a focus
on the patient, with patient focus being the True North of the practice.
Exhibit 1.4
THE PRACTICE MANAGEMENT MODEL
|
Continue to measure each step
|
Mission, Vision, and Values
��������������������� |
Strategic Planning and Decision Making
���������������� �����|
�����������
Operations
���������������������� |
�����������
Assessment
���������������������� |
���� Process
Improvement
|
True North
|
��True North� is a concept taken from Lean
management that embodies the ideal state of a practice, its providers� vision
of perfection, and the type and quality of practice it should strive to achieve
every day. True North should transcend the individual and his or her personal
goals or actions. Achieving personal objectives is not mutually exclusive but coincidental
with True North.
Exhibit 1.5 shows the number of
physicians practicing in the United States. This number can be further broken
down into the number of practices by size and multispecialty versus single
specialty, as shown in exhibit 1.6. Note the increasing size of practices over
time, a trend that is expected to continue.
Exhibit 1.5
TOTAL ACTIVE PHYSICIANS IN THE UNITED STATES, APRIL 2017
|
Primary Care Physicians
|
Specialist Physicians
|
Total
|
|
443,962
|
479,346
|
923,308
|
Source: Kaiser Family Foundation (2017).
A primary care physician (PCP) is
often the first contact for a patient with an undiagnosed health concern. In
addition, PCPs frequently provide continuing care for many medical conditions
that are not limited by cause, organ system, or diagnosis. This purview of
practice differs from a medical specialist, who has completed advanced
education and clinical training in a specific area of medicine and typically
focuses on the diagnosis and treatment of one organ system of the body and its diseases.
Nurse practitioners and physician
assistants are a growing segment of medical service provider, as seen in
exhibit 1.7. A physician assistant (PA) is a nationally certified and
state-licensed medical professional. PAs practice medicine with physicians and
other providers and are allowed to prescribe medication in all 50 states, the
District of Columbia, the majority of US territories, and the uniformed
services. A nurse practitioner (NP) is a registered nurse qualified, through
advanced training, to assume some of the duties and responsibilities of a
physician.
PAs and NPs are sometimes
referred to as advanced practice professionals or midlevel providers; however,
the term mid-level provider is considered obsolete.
State laws vary as to the
specific duties PAs and NPs are allowed to perform, so the practice manager
must be fully informed on these regulations.
Advanced practice professionals
are becoming increasingly important to medical practices because they can
replace physicians in care delivery for many services, reserving the physician
for more complex care requiring their expertise. For example, PAs and NPs often
work as part of a care team with physicians. They may examine the patient
first; collect facts and findings; and then, in collaboration with the
physician, make a diagnosis
Exhibit 1.6
DISTRIBUTION OF SINGLE- AND MULTISPECIALTY PHYSICIANS BY
PRACTICE SIZE, 2014
|
Number of Physicians in Practice
|
Single-Specialty Practice
|
Multispecialty Practice
|
|
1
|
1.5%
|
0.3%
|
|
2 to 4
|
42.0%
|
13.8%
|
|
5 to 10
|
31.7%
|
20.8%
|
|
11 to 24
|
13.7%
|
17.2%
|
|
25 to 49
|
6.7%
|
11.1%
|
|
50+
|
4.5%
|
36.9%
|
|
Total
|
100%
|
100%
|
|
N
|
1,452
|
836
|
Source: Kane (2014).
and develop a treatment plan. The
physician supervises the process and conducts his or her own examination of the
patients to ensure that the proper care is delivered. The physician often
checks critical elements of the exam and establishes a relationship with the
patient.
The PA or NP typically follows up
with the patient once the treatment plan is established.
PRACTICE OWNERSHIP
In addition to the area of medicine practiced, physician
practices can be classified by type of ownership. Exhibit 1.8 shows the
distribution of medical practices by ownership.
Note the trend�also expected to continue�toward practice
ownership by hospitals and healthcare systems.
LICENSING PHYSICIANS
All 50 states require physicians
and medical providers to hold a license. The licensing of medical providers is
performed under the auspices of a medical examining board. These boards have
the right to grant a license to practice medicine and the responsibility to
investigate and discipline providers in cases of inappropriate conduct.
LICENSURE
A mandatory system of
state-imposed standards that practitioners must meet to practice a given
profession.
These licenses provide the
practitioner a general right and privilege to practice medicine, but they
usually do not grant specific privileges to practice a particular medical
specialty. This activity is beyond the scope of licensure and typically is conducted
by the hospital or hospitals at which the physician or advanced practice
provider delivers care.
The licensing process includes a
thorough, painstaking review and verification of the training and experience
the physician or provider has received. Criminal background checks and reviews
of the National Practitioner Data Bank (NPDB) are conducted in this process.
The NPDB contains documentation
of any disciplinary acts leveled against the physician, malpractice
settlements, and other practice restrictions the physician may have received.
Reciprocity, or the reciprocal
granting of a medical license by states based on licensing of the provider in
another state, has become a thing of the past because of concerns
Exhibit 1.7
NURSE PRACTITIONERS AND PHYSICIAN ASSISTANTS
|
Provider Type
|
Total
|
Percent
Primary Care
|
Practicing
Primary Care
|
|
Nurse practitioners
|
106,073
|
52.0%
|
55,625
|
|
Physician assistants
|
70,383
|
43.4%
|
30,402
|
Source: AHRQ (2011).
Exhibit 1.8
DISTRIBUTION OF PHYSICIANS BY PRACTICE OWNERSHIP
|
|
2012
|
2014
|
|
At least some hospital ownership
|
23.4%
|
25.6%
|
|
Wholly owned by hospital
|
14.7%
|
15.6%
|
|
Jointly owned, physicians and hospital
|
6.0%
|
7.3%
|
|
Unknown whether wholly or jointly owned
|
2.6%
|
2.7%
|
|
Direct hospital employee
|
5.6%
|
7.2%
|
|
Not-for-profit
|
6.5%
|
6.4%
|
|
Other
|
4.4%
|
4.0%
|
|
Total
|
100%
|
100%
|
|
N
|
3,466
|
3,500
|
Source: Kane (2014).
The origin and history of medical
practice that practitioners with a poor record or history of committing fraud
can simply cross state lines and begin anew.
Licensure should not be confused
with certification. Many medical specialties offer special recognition through
board certification, which indicates the practitioner has acquired additional,
specific training and testing in an area of medicine (see exhibit 1.9). Contrary
to licensure, the absence of board certification by itself does not prohibit a
physician from practicing in a medical specialty in most states.
MEDICAL TRAINING
According to the American
Association of Medical Colleges (AAMC 2016), 145 accredited US and 17
accredited Canadian medical schools; nearly 400 major teaching hospitals and
health systems, including 51 US Department of Veterans Affairs medical centers;
and more than 80 academic societies offer medical education. In addition, the
American Association of Colleges of Osteopathic Medicine (AACOM 2016) reports
that 31 colleges of osteopathic medicine are in operation. Although both are
fully licensed physicians in the United States and very similar in many
respects, doctors of osteopathy (DOs), or osteopaths, differ from medical
doctors (MDs) in the educational path they take for their medical education.
DOs attend osteopathic medical schools, and MDs attend allopathic medical
schools. Each type of school teaches the diagnosis and treatment of disease,
but the disciplines vary somewhat in philosophy, with the osteopathic approach
focusing more on a holistic view of human disease and treatment. Also worth
noting is that DOs often complete their postgraduate training in allopathic
residencies and fellowships, which further reduces the distinction between the
two types of physician.
Among them, these organizations
employ more than 128,000 faculty members, educate 83,000 medical students, and
host 110,000 resident physicians (AAMC 2016).
What Is Changing?
The Conundrum
Three fundamental aspects of
practice management and care delivery are important to focus on in any
discussion of medical practice: high quality, high access, and low cost.
Economists may argue that a
practice can succeed as a business with any two of those three components, for
instance, high quality and a high level of access, where cost is not low.
Indeed, economic theory holds that a business cannot achieve all three
simultaneously. However, medical practices must achieve each to be an effective
and high-quality practice.
Consider that in some countries,
to limit healthcare costs, a concern around the world, their healthcare systems
limit access. For example, delays are seen with hip replacements, knee
replacements, and even some essential surgeries. In the United States, these
procedures can be undertaken almost immediately. But healthcare costs for care
and treatment
Exhibit 1.9
PARTIAL LIST OF MEDICAL SPECIALTIES
|
Allergies and immunology
|
Anesthesiology
|
Cardiology
|
|
Dermatology
|
Emergency medicine
|
Genetics
|
|
Gerontology
|
Gynecology
|
Hematology
|
|
Internal medicine
|
Neurology
|
Obstetrics
|
|
Oncology
|
Otolaryngology
|
Palliative care and hospice
|
|
Pathology
|
Pediatrics and related subspecialties
|
Preventive medicine
|
|
Primary care practice
|
Psychiatrist
|
Radiation oncology
|
|
Radiology
|
Surgery and related subspecialties
|
Urology
|
are much higher than in other
countries. Thus, one job of the practice manager and leader is to maximize or
optimize the relationship between cost, access, and quality (see exhibit 1.10).
SOCIAL CHANGE
As US society has changed, so has
the practice of medicine. In social terms, the country has moved from a time
when information about health and our healthcare was the sole purview of the
medical professional to a time when individuals have access to an enormous
amount of information. The Internet has had a profound impact on healthcare.
Patients are now able to read about virtually any condition, diagnosis, or
treatment, and in many cases, they make judgments about what option is in their
best interest.
Patients also have demonstrated
new, or renewed, interest in alternative forms of healthcare. A variety of
terms are associated with alternative medicine, including complementary
medicine and integrative medicine. Complementary and alternative medicine (CAM)
modalities include acupuncture, energy therapies, magnetic field therapies,
therapeutic touch, Reiki, Ayurvedic medicine, herbal medicine, and Chinese
medicine, to name a few.
The effectiveness of these
therapies has been demonstrated to varying degrees, but Americans spent more
than $33.9 billion in 2007 on CAM products and services, according to a
National Institutes of Health survey conducted by the National Center for
Exhibit 1.10
THE PRACTICE CONUNDRUM
COST � QUALITY � ACCESS
Complementary and Integrative
Health (2009). These findings indicate that patients are seeking solutions that
suit their healthcare needs better than traditional medicine does.
What Are Some of Today�s
Challenges?
To develop an appreciation for
some of the important changes and challenges facing medical practice, this
section touches on a few important issues, including the following:
◆ The cost of care
◆ The Patient Protection and
Affordable Care Act of 2010 (ACA)
◆ Health policy issues, such
as changes to Medicare and Medicaid
◆ Changing disease burden
and rise of chronic disease
◆ Lack of a coordinated
system of care
◆ Rising consumerism and
patient-centered care
◆ Patient safety and quality
concerns
◆ Demographic changes in the
population
◆ Rapidly changing
technologies and treatments
◆ Digital transformation
◆ Nontraditional providers
◆ Workforce issues
◆ Uninsured and underinsured
populations
◆ Financial constraints of
practices
◆ Changing forms of payment
and reimbursement, driven in part by the
Medicare Access and CHIP Reauthorization Act of 2015
(MACRA), which replaced the sustainable growth rate formula for physician
reimbursement for services and includes
�� the Merit-Based Incentive Payment System and
�� advanced alternative payment models
◆ The political landscape,
including the possible replacement or repeal of the ACA
THE PERFECT STORM
The �perfect storm� metaphor
describes the coalescing of multiple events to create dramatic and unique
consequences. Similar to the scenario depicted in a novel with this title by
Sebastian Junger (2009), in which he describes a catastrophic storm off the
coast of New Bedford, Massachusetts, some US healthcare observers would
describe what is happening today in healthcare as a perfect storm.
No factor has affected the sense
of urgency to reform the US system of healthcare more than the cost. According
to CMS (2015), US healthcare spending increased 5.3 percent to $3.0 trillion in
2014, or $9,523 per person. This growth was primarily the result of the
coverage expansions under the ACA, particularly for Medicaid and private health
insurance.
Of course, the trend of rapidly
increasing healthcare costs was seen long before the passage and enactment of
the ACA: The share of the US economy devoted to healthcare spending was 17.5
percent, up from 17.3 percent in 2013 and almost 2.5 times that of other
Western countries.
Exhibit 1.11
THE FORCES OF CHANGE ACTING ON MEDICAL PRACTICES: �THE
PERFECT STORM�
|
The Practice and the Practice Manager
|
Patient
Safety
Quality
Population
Technology
Digital
Care
Issues
Workforce
Financials
Consumers
Policy
Issues
ACA
The Cost of Care
|
The Institute of Medicine, a
prestigious federal research and policy organization established in 1970 as
part of the National Academy of Sciences, estimates that roughly a third of US
healthcare dollars is wasted, amounting to between $700 and $800 billion. This
enormous amount of waste is a result of unnecessary services, insufficient care
that leads to readmissions and other repeat care, excess administrative costs,
and increasing prices (IOM 2001). As one might expect, waste and the resulting
excess expenditure in the US healthcare system is one area of tremendous
criticism from many observers.
According to the Organisation for
Economic Co-operation and Development (OECD 2015), an international economic
group composed of 34 member nations based in Paris, the important factors that
differentiate the US healthcare system from that of other countries are as
follows:
◆ The United States has
fewer physicians per capita than many other OECD countries have, at 2.4
practicing physicians per 1,000 people in 2010, below the OECD average of 3.1
practicing physicians per 1,000 people.
◆ The number of hospital beds
in the United States was 2.6 per 1,000 people in 2009, whereas the OECD average
was 3.4 beds.
◆ In the United States, life
expectancy at birth increased by nearly nine years between 1960 and 2010, while
it rose by more than 11 years on average in other OECD countries and by more
than 15 years in Japan. In 2010, the average American lived to be 78.7 years�more
than a full year below the average for other OECD countries. Cultural factors,
lifestyle issues, and health habits play a role in this difference.
THE AFFORDABLE CARE ACT AND OTHER
LEGISLATION
Since the passage of Medicare and
Medicaid legislation in 1965, no other law has had a greater impact on the
healthcare delivery system than the ACA. We discuss the ACA in detail in later
chapters; here, we consider its impact on the healthcare system as well as the
challenges and opportunities it brings.
The timeline shown in exhibit 1.2
includes a number of significant changes to healthcare regulations. As
healthcare moved from a trade to a profession, its regulation increased. Every
state now licenses the practice of medicine and enforces educational and training
standards toward that end. Medical practices must comply with all regulations
related to corporations and businesses in the state in which they operate and
are subject to employment regulations by state and federal government.
Major pieces of legislation have
been instrumental in shaping the direction of the practice of medicine in some
important ways; they include the following:
◆ Corporate Practices Act
◆ Medicare and Medicaid
legislation
◆ Balanced Budget Act of
1997, which created the resource-based relative valuescale
◆ ACA
◆ MACRA
THE CHANGING DISEASE BURDEN AND THE RISE OF CHRONIC DISEASE
DISEASE BURDEN
Another significant issue facing
the modern healthcare practice is how the burden of disease, or the impact of a
health problem as measured by financial cost, mortality, morbidity, or other
indicators, has changed and whether providers can keep up with these changes.
In 1900, gastrointestinal infections, tuberculosis, pneumonia, and influenza
were significant potential detriments to Americans� health and longevity. By
2010, however, cancer and heart disease became the major causes of mortality in
the United States (Jones, Podolsky, and Greene 2012). Add to these conditions
emerging diseases such as fibromyalgia and infections from the Zika virus�some
of which may not have become known until recently�and the enormity of disease
states medical practices must be equipped to treat is daunting.
The number of services provided
in practice offices is substantial. Most individuals receive most of their care
in a medical practice; the following statistics are just a sampling of the
scale (NCHS 2015a):
◆ Number of drugs ordered or
provided�2.6 billion
◆ Percentage of visits
involving drug therapy�75.1 percent
◆ Most frequently prescribed
therapeutic classes
�� Analgesics
�� Antihyperlipidemic agents
�� Antidepressants
◆ Percentage of persons
using at least one prescription drug in the past 30 days�48.7
percent (2009�2012)
◆ Percentage of persons
using three or more prescription drugs in the past 30 days�21.8 percent
(2009�2012)
◆ Percentage of persons
using five or more prescription drugs in the past 30 days�10.7 percent (2009�2012)
CHRONIC DISEASE
Almost half of US residents have
at least one chronic condition, and more than 85 percent of those older than 65
have a chronic disease. As defined by the Centers for Disease Control and
Prevention (CDC 2016a), chronic diseases are those that persist for three
months or more. They generally cannot be prevented by vaccines or cured by
medication, and they do not disappear spontaneously. Chronic disease is a major
driver of cost because approximately 80 percent of healthcare resources
expended are used by people with chronic conditions.
Importantly, most of the
treatment of these diseases occurs in the medical office setting.
According to the CDC (2016a),
chronic diseases are responsible for seven out of ten deaths in the United
States. Common chronic diseases include the following:
◆ Diabetes
◆ Heart disease
◆ Arthritis
◆ Kidney disease
◆ HIV/AIDS
◆ Lupus
◆ Multiple sclerosis
Because chronic disease cannot be
cured, prevention is the key to reversing the cost, morbidity, and mortality
trends currently seen in the healthcare system. Prevention is viewed as taking
place in one of three levels:
1. Primary prevention seeks to
avoid the onset of a disease using risk-reduction strategies such as altering
behaviors or eliminating exposures that can lead to disease, or by enhancing
resistance to the effects of exposure to a disease agent.
An example of primary prevention
is vaccination against flu.
2. Secondary prevention includes
procedures that detect and treat so-called preclinical health status changes
and controlling disease progression. An example of secondary prevention is mammography
to detect early breast cancer.
3. Tertiary prevention reduces
the impact of disease on the patient�s functioning, longevity, and quality of
life. An example of tertiary prevention is cardiac rehabilitation following a
heart attack.
A Large and Growing Problem: The
Number of People with Chronic
CONDITIONS
Boyle and colleagues (2001)
projected a 165 percent increase in diabetes by 2050 to a prevalence of 7.2
percent of the population, affecting 29 million US residents. More recent
evidence suggests those figures might be underestimations (CDC 2012). Unless
that incidence curve is changed, US society will continue to see the
devastating complications of this disease, including neuropathy (nerve damage),
blindness, kidney failure, and heart disease.
Type 2 diabetes and many other
chronic diseases are classified as �lifestyle diseases� because they are
preventable and closely related to diet, exercise, and other lifestyle
behaviors (Al-Maskari 2010).
In addition to causes such as
obesity, observers expect to see a steady increase in the number of people with
chronic conditions, in part because the US population is aging, and older
people tend to have more chronic disease than younger people have.
Health-conscious behavior,
including a focus on eating natural and chemical-free foods, has become a more
popular way to combat chronic disease. Medicine has come a long way from the
time of Hippocrates, but we are wise to remember what he said: �Let medicine be
thy food and let food be thy medicine� (Lloyd 1950). That old wisdom must be
reinserted into medical practice, at least to some degree.
LACK OF A COORDINATED SYSTEM OF
CARE
The US healthcare system
currently does not pay adequate attention to the continuum of health services
and the continuum of care. As human beings, we have healthcare concerns
starting before we are born and present or emerging all the way until the end
of our lives.
An effective system of care needs
to reflect all the stages of one�s life.
In particular, end-of-life care
is an issue that lacks a coordinated model in the United States. Many observers
consider that the US healthcare delivery system does not deal with end-of-life
care well. For example, a significant amount of money is spent at the end of
life for care that, in many cases, is at best futile and at worst harmful to
the patient and his or her family.
A coordinated system of care also
should be concerned with the determinants of health. Exhibit 1.12 shows some
major factors that determine health status. Healthcare is a component, but many
others are present. The increased focus on the determinants of health points to
the need for medical practices to be aware of and attend to the other
Practices can do more in this
area than they are currently; we discuss those ideas in later chapters.
RISING CONSUMERISM
An area of medical practice and
healthcare in general that also has received regular attention recently is the
experience of the patient and his or her family. In considering this issue, one
must first distinguish between two primary modes of practice as they relate to
patient care.
PROVIDER-DIRECTED
CARE
The first is provider-directed
patient care. In this model, which has been practiced for decades in the United
States, the provider makes the vast majority of decisions and determines the
type and extent of care the patient receives.
One concern related to
provider-directed care is that the patient may have little understanding about
the treatment being received and, therefore, be less committed to complying
with instructions. For provider-directed healthcare to result in satisfactory
outcomes, a patient must have both the desire and the ability to comply with
treatment recommendations; thus, his or her individual circumstances are very
much a part of the treatment equation.
Exhibit 1.12
DETERMINANTS OF HEALTH
|
Societal Issues
|
� Crime
� Housing
� Family relationships
� Culture
� Behavior
|
|
Health Policy
|
� Access to healthcare
� Affordable Care Act
� Environmental protection
� Funding for services
� Funding for research
|
|
Biological Factors
|
� Genetics
� Biology of disease
� Sex
� Age
|
PATIENT-CENTERED
CARE
The second model is
patient-centric healthcare. In this model, the patient and his or her family
play a central role in conjunction with the provider (Jones 2014). The provider
offers multiple options to the patient, all of which are medically acceptable,
and the patient assumes greater decision-making responsibility regarding the
approach to treatment.
Patient-centered care can be seen
in decisions related to treating prostate cancer.
Prostate cancer is often a
slow-growing tumor. In fact, more than 80 percent of men older than age 80 have
prostate cancer, but the disease has limited medical consequences in many of
these cases. Due to the slow-advancing nature of prostate cancer, two viable
approaches are considered for its treatment. One approach, known as watchful
waiting, involves careful monitoring of the patient�s condition whereby
aggressive intervention is not undertaken until definitive signs indicate the
cancer is growing. The second option is aggressive therapy.
This approach may involve
surgery, chemotherapy, or other forms of treatment.
The question is, which to choose?
According to a study published in the New England
Journal of Medicine (Bill-Axelson
et al. 2014), the benefits of aggressive therapy were found to be highly
dependent on the age of the patient and the type of prostate cancer.
This finding gives enhanced
credence to the notion of watchful waiting, which may also reduce unnecessary
surgery, side effects, and cost.
One major initiative in
population health management related to patient-centric care that involves the
medical practice is the patient-centered medical home (PCMH).
The PCMH provides a starting
place for the patient to receive all his or her nonemergency medical care. The
model is characterized by 24/7 access to tightly coordinated care by a team of
providers. Primary care is offered at the PCMH location, and other medical
services are referred to specialists as appropriate (NCQA 2014).
Today, physicians are becoming
increasingly patient centered. In addition to bringing the patient to the
decision-making table, they are accommodating him or her in other ways, such as
adopting alternate forms of communication, such as e-mail (Dalal et al. 2016).
PATIENT SAFETY AND QUALITY
CONCERNS
In terms of patient safety and
quality, the medical practice must ensure that it provides healthcare that
meets the following standards (IOM 2001; AHRQ 2016):
VALUES
The beliefs and guidelines an
individual uses to make choices when confronted with a situation.
◆ Safe�Protecting patients from being harmed by the care that is
intended to help them. This goal includes the prevention of nosocomial
infections, which are infections acquired in the hospital or healthcare
setting; wrong-site surgery; medication errors; falls; and other harmful
events.
◆ Effective�Providing services on the basis of scientific knowledge to all
who can benefit and refraining from providing services to those not likely to
benefit (i.e., avoiding underuse and misuse, respectively).
◆ Patient centered�Providing
care that is respectful of and responsive to individual patient preferences,
needs, and values and ensuring that patient values guide all clinical
decisions.
◆ Timely�Reducing wait times for and eliminating harmful delays in
care.
◆ Efficient�Avoiding waste,
including waste of equipment, supplies, ideas, and energy.
◆ Equitable�Providing care that does not vary in quality because of
personal patient characteristics such as race, gender, ethnicity, geographic
location, and socioeconomic status.
DEMOGRAPHIC CHANGES
THE GRAYING OF AMERICA
The baby boom generation is
retiring at the rate of about 10,000 people per day. In fact, the most rapidly
growing segment of the US population is people older than age 85. US residents
are living much longer than in the past, and as people age, they tend to need
more healthcare. Although healthcare is a major contributor to longevity, it is
not the only important contributor; other factors may have an even more
significant impact on length of life (Nelson 2016). Only in the past 100 years
has longevity been linked to healthcare.
Before that time, life expectancy
was largely determined by uncontrollable risk, such as infections, accidents,
childbirth, starvation, and other similar events. For example, George
Washington died from acute laryngitis, a condition that is easily treated today
with an antibiotic (Knox 1933).
The graying of America will
continue to be a significant issue for medical practices, as from age 65, on
average, men and women will live almost 20 additional years (NCHS 2015b):
◆ Both sexes at 65 years�19.3 years of average additional life expectancy
◆ Men at 65 years�17.9 years of average additional life expectancy
◆ Women at 65 years�20.5 years of average additional life expectancy
CHANGES IN THE US POPULATION
The increase in immigration to
the United States and the diversity of the population are major new
considerations for medical practices. US providers encounter more languages,
customs, and beliefs than in the past, making service to patients an increasing
challenge.
Mastering the nuances of
diversity is essential for a modern practice to be successful.
RAPIDLY CHANGING TECHNOLOGIES AND
RELATED TREATMENTS
The healthcare industry has seen
a dramatic shift in the types and complexity of medical technology and the
available treatments for patients. This unrelenting trend has led to
commensurate complexity and increased cost, as well as the need for greater
specialization in the delivery of services.
DIGITAL TRANSFORMATION AND
NONTRADITIONAL PROVIDERS
AMBULATORY CARE
Healthcare services provided to
patients on an outpatient basis, rather than by admission to a hospital or
another healthcare facility.
Not only has the science and
technology of treatment changed, but the way healthcare is delivered is rapidly
changing as well. A major transformational force in the medical practice has
been the rise of digital media tools and the nontraditional provider who has
been enabled by digital innovations.
Transformation often does not
occur from within the industry being transformed, and healthcare is no
exception. In 2015, more than 165,000 healthcare apps were available for
smartphones and tablet computers, many of them targeted to the ambulatory care
environment and most developed outside the healthcare industry (Terry 2015).
The medical practice must compete
with entrants from the information technology industry, the retail
pharmaceutical industry, the insurance industry, medical device companies, and Internet-based
providers from around the world. The emergence of web-based providers has
created a whole new mobile health industry known as mHealth.
The digital transformation of
healthcare is not limited to the alternative delivery modes; it also has revolutionized
the availability of information. One may consider this development to have a
democratizing effect on healthcare, as information about virtually any
condition, treatment, or procedure is available on the Internet. Like most
innovations, it can carry both positive and negative consequences. Although a
tremendous amount of information is available, this information is often of
limited value unless it can be properly interpreted by a professional. A
patient may be aware of information, but he or she may not understand it and
certainly will not be able to apply it to the situation at hand.
Another major issue regarding
Internet-based information is its accuracy. Physicians are often concerned that
patients access information that is either misunderstood or, in some cases,
blatantly inaccurate, which can cause difficulties in the physician�patient
The patient may be skeptical of
information provided by the physician because it conflicts with inaccurate
information the patient obtained from another source and believes to be true.
One solution to this problem is to provide patients with high-quality sources
for Internet-based information about their condition and encourage them to
obtain more detailed information. Therefore, the Internet can be an educational
resource for the physician practice when proactively embraced and used
properly.
WORKFORCE ISSUES
For the first time in US history,
four generations of employees are in the workforce, and that workforce is
becoming increasingly diverse in many other areas as well. These factors
present unprecedented challenges, as each generation and ethnic group brings
its own temperament; belief system; and preferences for structure, authority,
and workplace interaction (Knight 2014).
One issue that arises from intergenerational
and ethnic diversity is that people tend to focus on differences instead of
looking for similarities to forge collaborations and embrace new ideas. This is
a key consideration, as the process of collaboration allows people to produce
the best outcome possible.
How do we get multiple
generations to work effectively in a collaborative fashion?
Everyone has much to contribute
and share, and practice managers must devise ways for the organizations to tap
the power of diversity. One means to do so is to focus on the shared objective
in light of the value each generation and group brings to the work environment.
By making the most of our diverse
workforce, practice managers and leaders can combine new concepts and
innovations to solve problems together.
FINANCIAL CONSTRAINTS
By definition, constraints limit
the scope, the time, or the quality of the product or service being provided.
As resources are limited, decisions must be made in an effort to optimize the
constraint relationship and thereby deliver optimum outcomes. Of course,
financial resources are no different. Financial constraints limit the freedom
to act and provide support for people and projects in the organization (Travis
et al. 2004).
STAKEHOLDER
Individual or group that has a
vested interest in the practice.
In a later chapter, we delve into
the issues related to fighting financial constraints in more detail. Here, we
consider the unique nature of healthcare financing as a source of concern for
the practice manager. Although practices set their own fees, in most cases
healthcare is paid for by so-called third-party payers, such as Medicare.
Medicare establishes reimbursement limits for services, effectively setting the
fees for the practice. Similarly, in the case of nongovernmental payers, such
as insurance companies, fees may be negotiated, but negotiation is often
limited by the size and market power of the practice. Small practices may be
dealt with on a take-it-or-leave-it basis. Most enterprises have their actual
payment rate or price established by external stakeholders; these represent a
unique and challenging aspect of medical practice management.
As in a society, practice
managers and leaders must balance the ideal outcome with what is possible given
that all resources are limited to some extent. Doing so requires a combination
of personal responsibility and practice accountability.
LEADERSHIP CHALLENGES
The list of challenges discussed
to this point is significant. To address them, medical practice leaders and
managers must be adept at guiding change in their practice.
THE REIMBURSEMENT PARADIGM SHIFT
PARADIGM SHIFT
A change in the way a practice
views its business.
The paradigm of medical practice
is currently experiencing a seismic shift. Most businesses and industries
undergo transitions of their business and operational models over time as the
environment of the industry changes. However, the current paradigm shift means
medical practices will be paid differently than in the past, placing a lot of
pressure on how practices adapt to other changes occurring in the healthcare
system, such as the way medical care is delivered.
What Happens to Organizations
When a Paradigm Shift Occurs in an Industry?
A paradigm is the way
stakeholders think an industry should behave�the model they hold in their mind.
This model has a strong hold, like a set of strong beliefs; thus, changing a
paradigm is difficult.
A paradigm shift is a major
change in the way the world thinks about something.
One example of a paradigm shift
occurred in the photography industry when cameras became digital. Kodak, a
company with a history spanning more than a hundred years, was fixated on film
and slides, and the cameras that used these photographic modes. As digital
photography became widely adopted, Kodak refused to act on the paradigm shift
and continued to focus on film and cameras and more film. Essentially, Kodak�s
leaders forgot that the business they were in was not about photography but
about people. And people�consumers�had become less interested in film cameras;
they were more interested in recording their lives and preserving memories. The
modality mattered less to them that the activity. The irony is that Kodak
invented digital photography but chose not to pursue the technology for the
commercial market (Lucas and Goh 2009). Steve Jobs of Apple Computer saw the
potential of making the digital camera part of the popular iPhone, providing an
effortless way to take pictures that met the needs of most photography
consumers.
TELEMEDICINE
Involves the use of electronic
communication and information technologies to provide or support clinical care
at a distance.
This is an example of the second
curve. This concept was introduced by healthcare futurist Ian Morrison in 1996.
He posits that service and product innovation go through a series of curves.
Each curve represents a product or service that matures over time and is then
replaced by either a new or improved service or product. Entities that operate
in an industry undergoing a paradigm shift must move past the first curve or be
doomed to failure. In healthcare, the second curve is represented by
telemedicine, web-based medical services, on-demand medical services, and new
information technologies used to analyze and understand patient populations and
their needs. Those practices that fail to enter the second curve will become
obsolete as well. An important aspect of paradigm shifts is that they cause
participants� knowledge base to shrink; every player starts over to build a new
model of care.
The transition point from the
first curve to the second curve is called the strain.
PAY FOR PERFORMANCE
(P4P)
Mechanism whereby providers are
reimbursed on the basis of their level of success in meeting specific
performance measures.
Here, the demand for and
provision of healthcare shift from being experienced predominantly the old way
to predominantly the new way, for example, from office visits to virtual
visits. The strain is a difficult point in a practice�s operational life, and
many businesses fail during this period. The organization must function in both
paradigms simultaneously, aiming to move safely from the first curve to the
second curve. Because the US healthcare system is changing incrementally from
volume-based reimbursement (the old paradigm) to value-based reimbursement or
pay for performance (the new paradigm), the second curve challenge for medical
practices is that they must continue to operate in a volume-base system while slowly
transitioning to the value paradigm. At the time of this writing, the majority
of revenue for medical practices remains volume based (Center for Healthcare
Quality and Payment Reform 2013).
REVENUE
The amounts received by or due to
a practice for goods or services it provides to customers.
Receipts are cash revenues;
revenues may also be represented by accounts receivable.
What Is Value?
Value is a function of cost and quality, as demonstrated by
the following equation:
Value = f (Cost/Quality)
In practical terms, value is what
we are willing to pay for: what we see as a fair exchange of our resources
(money) for something we receive (healthcare). Cost comprises all the economic
and noneconomic input needed to receive the service. It includes money, of
course, but also such factors as waiting time, access issues, and perception of
caring, and many others that may be particular to the individual expending the
cost.
Quality is a measure of how good
the service is. In healthcare, it can be determined by many factors. Some
questions that may help ascertain quality include the following:
◆ Did I get well?
◆ Was the service timely?
DETERMINANTS OF HEALTH
Another important issue in
practice management, and healthcare administration in general, is understanding
the determinants of health. (Review the select factors listed in exhibit 1.12 that
go into determining health.) Many determinants are outside of individuals�
control, such as in what generation or era one is born and one�s biological
sex, race, and other genetic and biological factors. Others, including
individual behaviors; family and community networks; living and working
conditions; and broad social, economic, cultural, health, and environmental
conditions, are controllable to greater or lesser degrees. All these
determinants can have a tremendous impact on overall health.
Every practice must consider its
role in mitigating these issues, which go beyond what are traditionally
considered to be �healthcare issues.� Practices should engage patients in
improving self-care and self-management, and they must be leaders and advocates
for change in the lifestyle behaviors that have led to increases in the disease
burden.
Furthermore, public policy plays
a major role in health determinants, such as equity of care, and healthcare
professionals should advocate for improvements to health policy that influences
these issues.
CHANGES IN HEALTH COVERAGE
Since health insurance became
commonplace after World War II, numerous changes have occurred in how
healthcare is paid for. Originally, health insurance was primary indemnity
coverage. This coverage provided payment to physicians or repaid the patient
for the out-of-pocket costs incurred by the patient in seeking medical
treatment as set forth in the policy.
BAD DEBT
Amount owed to a practice that
will not be paid.
Managed care became common in the
1980s and has gone through a number of transitions over the years. A relatively
recent invention in health insurance, the consumer directed health plan (CDHP),
is having a profound impact on the medical environment.
CDHPs provide coverage for
medical services, but only after a substantial out-of-pocket deductible has
been met by the patient. This requirement has led some patients to delay care
or fail to pay the provider for care received because they do not have
sufficient funds to cover the deductible. The latter results in the provider or
medical practice encountering increasing amounts of bad debt.
Healthcare finance is covered in
detail in a later chapter.
CHANGES IN ORGANIZATIONAL
STRUCTURE
In modern times, the predominant
form of medical practice has been solo practice or small practice groups and
partnerships. However, as the US healthcare system has evolved in response to
value-based reimbursement and other environmental factors, consolidation of
medical practices is occurring. Much more about this topic is covered
throughout the remainder of the book.
ENVIRONMENTAL FACTORS
Forces that influence the
business but are external to the business itself, such as public policy, regulations,
and economic conditions.
THE COMPLEXITY OF THE HEALTHCARE
ENVIRONMENT
The healthcare environment has
become highly complex and will only continue to increase in complexity.
Numerous new technologies and services as well as increasing volumes of
information lead to new management challenges. For example, as discussed in
depth in chapters 6 and 7, the move from using the International Classification
of Diseases, Ninth Edition, Clinical Modification (ICD-9-CM) to ICD 10 for
documenting diagnostic codes for reimbursement increased the number of codes
from approximately 14,000 to more than 69,000. In addition, an entirely
different set of codes, Current Procedural Terminology codes, recently
increased to more than 71,000 codes from the previous set of 3,824 codes (CDC
2015).
SCIENTIFIC AND TECHNOLOGICAL
CHANGE
The technological achievements in
healthcare have been nothing short of remarkable. Consider that just a few
years ago major surgery was a common treatment option for a person suffering
from stomach ulcers, requiring a hospital stay and posing surgical risk. Today,
many people with stomach ulcers can be treated with a simple over-the-counter
medicine known as a proton pump inhibitor.
(back
to content)
2.2
History of Use of Traditional Herbal Medicines h
By definition, �traditional� use of
herbal medicines implies substantial historical use, and this is certainly true
for many products that are available as �traditional herbal medicines�.
In many developing countries, a
large proportion of the population relies on traditional practitioners and
their armamentarium of medicinal plants in order to meet health care needs.
Although modern medicine may exist side-by-side with such traditional practice,
herbal medicines have often maintained their popularity for historical and
cultural reasons. Such products have become more widely available commercially,
especially in developed countries. In this modern setting, ingredients are
sometimes marketed for uses that were never contemplated in the traditional
healing systems from which they emerged. An example is the use of ephedra (= Ma
huang) for weight loss or athletic performance enhancement (Shaw, 1998). While
in some countries, herbal medicines are subject to rigorous manufacturing
standards, this is not so everywhere. In Germany, for example, where herbal
products are sold as �phytomedicines�, they are subject to the same criteria
for efficacy, safety and quality as are other drug products. In the USA, by
contrast, most herbal products in the marketplace are marketed and regulated as
dietary supplements, a product category that does not require pre-approval of
products on the basis of any of these criteria. These matters are covered
extensively in Section 3 below.
1.1 The role of herbal medicines
in traditional healing
The pharmacological treatment of
disease began long ago with the use of herbs (Schulz et al., 2001). Methods of
folk healing throughout the world commonly used herbs as part of their
tradition. Some of these traditions are briefly described below, providing some
examples of the array of important healing practices around the world that used
herbs for this purpose.
1.1.1 Traditional Chinese
medicine
Traditional Chinese medicine has
been used by Chinese people from ancient times.
Although animal and mineral
materials have been used, the primary source of remedies is botanical. Of the
more than 12 000 items used by traditional healers, about 500 are in common use
(Li, 2000). Botanical products are used only after some kind of processing,
which may include, for example, stir-frying or soaking in vinegar or wine. In
clinical practice, traditional diagnosis may be followed by the prescription of
a complex and often individualized remedy.
Traditional Chinese medicine is
still in common use in China. More than half the population regularly uses traditional
remedies, with the highest prevalence of use in rural areas. About 5000
traditional remedies are available in China; they account for approximately one
fifth of the entire Chinese pharmaceutical market (Li, 2000).
1.1.2 Japanese traditional medicine
Many herbal remedies found their
way from China into the Japanese systems of traditional healing. Herbs native
to Japan were classified in the first pharmacopoeia of Japanese traditional
medicine in the ninth century (Saito, 2000).
1.1.3 Indian traditional medicine
Ayurveda is a medical system
primarily practiced in India that has been known for nearly 5000 years. It
includes diet and herbal remedies, while emphasizing the body, mind and spirit
in disease prevention and treatment (Morgan, 2002).
1.2 Introduction of traditional
herbal medicines into Europe, the USA and other developed countries
The desire to capture the wisdom
of traditional healing systems has led to a resurgence of interest in herbal
medicines (Tyler, 2000), particularly in Europe and North America, where herbal
products have been incorporated into so-called �alternative�, �complementary�,
�holistic� or �integrative� medical systems.
During the latter part of the
twentieth century, increasing interest in self-care resulted in an enormous
growth in popularity of traditional healing modalities, including the use of
herbal remedies; this has been particularly true in the USA. Consumers have
reported positive attitudes towards these products, in large part because they
believe them to be of �natural� rather than �synthetic� origin, they believe
that such products are more likely to be safe than are drugs, they are
considered part of a healthy lifestyle, and they can help to avoid unnecessary
contact with conventional �western� medicine.
While centuries of use in
traditional settings can be used as testimony that a particular herbal
ingredient is effective or safe, several problems must be addressed as these
ingredients are incorporated into modern practice.
One problem is that ingredients
once used for symptomatic management in traditional healing are now used in
developed countries as part of health promotion or disease prevention
strategies; thus, acute treatment has been replaced by chronic exposure (e.g.,
herbal products used for weight loss, Allison et al., 2001). This means that a
statement about �thousands of years of evidence that a product is safe� may not
be valid for the way the product is now being used. This does not expressly
mean that an ingredient is unsafe; it does mean that safety in the modern
context cannot be assumed.
A second problem is that efficacy
and effectiveness have rarely been demonstrated using modern scientific
investigations. An evidence-based approach to this issue has only recently been
implemented, and the results reveal that for most herbal products, considerable
gaps in knowledge need to be remedied before one can be convinced about their
efficacy.
One of the most difficult issues
to contend with in translating traditional herbal practices into conventional
�western� medicine is the individualization of prescriptions containing
multiple herbal and other ingredients. There is little incentive for
standardization of products for a mass market, when the intention has been to
provide an individual prescription. To the small grower or the traditionally
trained herbalist, standardization means understanding the growth conditions,
the time of harvesting, the manner of extraction or other preparation of
material so that a reliable (albeit small amount of) active ingredient can be
offered to people. To the manufacturer or distributor of large quantities that
will be sold in a supermarket or a health food store, standardization refers to
industrial production under defined conditions, using so-called Good
Manufacturing Practices (GMP) (Food & Drug Administration, 2002) akin to
those used for drug production.
In the USA, there is both
small-scale and large-scale production of herbal products and there can be wide
variation in their content and quality in the marketplace. Regulations in the
USA do not yet require that dietary supplement manufacturers adhere to standard
manufacturing practices, and so quality is not guaranteed (see Section 3). The
public becomes discouraged by reports that products taken from store shelves do
not consistently contain the ingredients�or in the amounts�that are claimed on
the label.
For herbal products in common
use, evidence of efficacy may be based upon traditional use, testimonials,
clinical studies, both controlled and uncontrolled, and randomized,
double-blind, placebo-controlled trials. For the most part, however, there is a
lack of systematic clinical studies to support claims.
Safety of some herbal ingredients
has been recently called into question, in part because of the identification
of adverse events associated with their use and, increasingly, because of the
demonstration of clinically relevant interactions between herbs and
prescription drugs.
Adverse events (stroke, heart
attacks, heart-rate irregularities, liver toxicity, seizures, psychoses and
death) associated with use of ephedra for weight loss, body-building effects
and increased energy or kava-kava (also known as kawa), widely used in Europe
and increasingly in Canada to treat anxiety, nervousness, insomnia, pain and
muscle tension, for example, have caused some countries to issue regulations
restricting or banning these products (e.g. Health Canada Online, 2002a,b).
Only a few herbs in common use have been suspected of causing cancer. These
include Aristolochia, Rubia tinctorum, Morinda officinalis and Senecio
riddellii, as discussed in detail below.
SOME TRADITIONAL HERBAL MEDICINES
2. Use of Traditional Herbal
Medicines in Developed Countries
2.1 Origin, type and botanical
data
Plants and their secondary
metabolite constituents have a long history of use in modern �western� medicine
and in certain systems of traditional medicine, and are the sources of
important drugs such as atropine, codeine, digoxin, morphine, quinine and
vincristine.
Use of herbal medicines in
developed countries has expanded sharply in the latter half of the twentieth
century. Monographs on selected herbs are available from a number of sources,
including the European Scientific Cooperative on Phytotherapy (ESCOP, 1999),
German Commission E (Blumenthal et al., 1998) and the World Health Organization
(WHO, 1999). The WHO monographs, for example, describe the herb itself by a
number of criteria (including synonyms and vernacular names) and the herb part
commonly used, its geographical distribution, tests used to identify and
characterize the herb (including macroscopic and microscopic examination and
purity testing), the active principles (when known), dosage forms and dosing,
medicinal uses, pharmacology, contra-indications and adverse reactions. Other
resources that provide detailed information about herbal products in current
use include the Natural Medicines Comprehensive Database (Jellin, 2002) and
NAPRALERT (Natural Products ALERT) (2001).
Information about other available
databases has been published by Bhat (1995).
2.2 Medicinal applications,
beneficial effects and active components
In some cases, the active
principles of plant-derived products have been isolated and characterized, and
their mechanisms of action are understood (e.g., ephedrine alkaloids in some
species of Ephedra). For many, however, including virtually all of the most
common products in the marketplace, such information is incomplete or
unavailable.
This is in large part due to the
complexity of herbal and botanical preparations; they are not pure compounds.
It is also a function of the traditionally-held belief that the synergistic
combination of several active principles in some herbal preparations is
responsible for their beneficial effects.
2.3 Trends in use���������
Data on the global nutrition products industry, in which
herbal and botanical products are often included, are given in Table 1.
 a
a
SOME TRADITIONAL HERBAL MEDICINES
Table 1. The global nutrition products industry in 1999,
including herbal and botanical products (in millions of US $)
|
Country
|
Vitamins/
minerals
|
Herbs/
botanicals
|
Sports,
meal
replacement,
homeopathy,
specialty
|
Natural
Foods
|
Natural
personal
care
|
Functional
foods
|
Total
|
|
USA
|
7070
|
4070
|
4320
|
9470
|
3590
|
1680
|
44520
|
|
Europe
|
5 670
|
6 690
|
2 510
|
8 280
|
3 660
|
15 390
|
42 200
|
|
Japan
|
3 200
|
2 340
|
1 280
|
2 410
|
2 090
|
11 830
|
23 150
|
|
Canada
|
510
|
380
|
250
|
700
|
330
|
1 500
|
3 670
|
|
Asia
|
1 490
|
3 170
|
970
|
710
|
880
|
1 450
|
8 670
|
|
Latin
America
|
690
|
260
|
250
|
460
|
250
|
360
|
2 270
|
|
Australia
and New Zealand
|
300
|
190
|
90
|
340
|
140
|
540
|
1 600
|
|
Eastern
Europe and Russia
|
350
|
220
|
250
|
180
|
40
|
269
|
1 300
|
|
Middle
East
|
180
|
90
|
60
|
70
|
30
|
140
|
570
|
|
Africa
|
160
|
80
|
70
|
80
|
10
|
120
|
520
|
|
Total
global
|
19 260
|
17 490
|
9 960
|
22 700
|
11 020
|
47 670
|
128 470
|
From Nutrition Business Journal (2000), derived from a
number of sources. Totals may not add up due to rounding.
a. Natural foods: foods grown or marketed with a focus on
the perceived benefits of �foods derived from natural sources� and that are, to
varying degrees, free of pesticides, additives, preservatives, and refined
ingredients
b. Functional foods: foods fortified with added or
concentrated ingredients to improve health and/or performance
Sales of dietary supplement
products, including herbal and botanical supplements, in the USA increased
dramatically during the 1990s, stimulated in the latter part of the decade by
the Dietary Supplements Health and Education Act of 1994 (DSHEA) (Tyler, 2000).
This pattern of growth has been replicated elsewhere in the world (Table 2),
although more recently, sales of herbal products have apparently experienced a
decline.
In the European Union (EU), in
general, herbal products for which therapeutic claims are made must be marketed
and regulated as drugs, while those that do not make such claims may be found
in the food or cosmetic categories. Attempts are at present being made to
harmonize the scientific and regulatory criteria that govern the marketing of
herbal products (AESGP, 1998).
Table 2: Trends in the global nutrition products industry,
1997�2000 (in millions of US $)
|
|
1997
|
1998
|
1999
|
2000
|
|
Vitamins/minerals
|
18 000
|
18 870
|
19 620
|
20 440
|
|
Herbs/botanicals
|
15 990
|
16 980
|
17 490
|
18 070
|
|
Sports,
meal replacement, homeopathy, specialty
|
8 760
|
9 310
|
9 960
|
10 710
|
|
Natural
foodsa
|
16 690
|
19 910
|
22 700
|
25 420
|
|
Natural
personal care
|
9 620
|
10 280
|
11 020
|
11 850
|
|
Functional
foodsb
|
40 320
|
43 940
|
47 670
|
51 480
|
|
Total
|
109 380
|
119 290
|
128 470
|
137 980
|
From Nutrition Business Journal (2000), derived from a
number of sources
a. Natural foods: foods grown or marketed with a focus on
the perceived benefits of �foods derived from natural sources� and that are, to
varying degrees, free of pesticides, additives, preservatives, and refined
ingredients
b. Functional foods: foods fortified with added or
concentrated ingredients to improve health and/or performance
In 1994, when the Dietary
Supplements Health and Education Act (DSHEA) was passed in the USA,
approximately 50% of the adult population of the country was reported to use
dietary supplements and sales of all products combined were approximately $4
billion. This category of products includes vitamins, minerals and a variety of
other ingredients; herbal products accounted for about one quarter of those
sales. In 2000, the last year for which comparable data are available, again
50% of the adult population reported use of dietary supplements, and sales were
close to $15 billion; herbals accounted for nearly one third of those sales.
Table 3 identifies some trends in herbal supplement use in the USA from 1997 to
2000.
Table 3: Ten top-selling herbs in the USA, 1997�2000 (in
millions of US $) a
|
|
1997
|
1998
|
1999
|
2000
|
|
Combination
herbsb
|
1 659
|
1 762
|
1 740
|
1 821
|
|
Ginkgo
biloba
|
227
|
300
|
298
|
248
|
|
Echinaceac
|
203
|
208
|
214
|
210
|
|
Garlic (Allium
sativum)
|
216
|
198
|
176
|
174
|
|
Ginsengd
|
228
|
217
|
192
|
173
|
|
St
John�s wort (Hypericum perforatum)
|
100
|
308
|
233
|
170
|
|
Saw
palmetto (Serenoa repens)
|
86
|
105
|
117
|
131
|
|
Soy
(soya)
|
NA
|
NA
|
36
|
61
|
|
Valerian
(Valeriana officinalis)
|
30
|
41
|
57
|
58
|
|
Kava-kava
|
22
|
44
|
70
|
53
|
|
Total
herbal supplements
|
NA
|
NA
|
4 070
|
4 130
|
NA, not available
a. From Nutrition Business
Journal (2001) and Schulz et al. (2001). US consumer sales via all channels
(includes all retail channels, direct sales, multilevel marketing, mail order
and practitioner sales)
b. Combination herbs include
products sold for weight management, athletic performance enhancement or energy
enhancement and often include mixtures of several herbal extracts, as well as
single-compound ingredients. Others that have appeared in the top 10 list in
earlier years, but not in 2000, include: goldenseal (Hydrastis canadensis),
cranberry, bilberry (European blueberry), aloe (see monograph on Rubia
tinctorum, Morinda officinalis and anthraquinones in this volume).
c. Two types of coneflower
preparation can be recommended and prescribed today: alcoholic extracts made
from the root of the pale purple coneflower (Echinacea pallida) and juices
expressed from the fresh aerial parts of the purple coneflower (Echinacea
purpurea). It is noteworthy that until about 1990, the root of Echinacea
pallida appears to have been regularly confused with that of the species
Echinacea angustifolia.
d. Panax ginseng is cultivated in
Asia; panax quinquefolius is cultivated in the USA.
In the 1990s, the USA saw the
growth of government organizations concerned with dietary supplements, such as
the National Institutes of Health (NIH) National Center for Complementary and
Alternative Medicine and Office of Dietary Supplements, and the National Cancer
Institute (NCI) Chemoprevention Program of the Division of Cancer Prevention
and Control. Organizations involved with dietary supplements such as the
American Nutraceutical Association and the Foundation for Innovative Medicine,
as well as industry trade associations such as the American Herbal Products
Association, the Consumer Healthcare Products Association, the National Natural
Foods Association, the Utah Natural Products Alliance and the Council for
Responsible Nutrition have been expanding during the 1990s.
In Canada, herbal use has also
increased. Berger (2001) noted, in summarizing the results of a 2001 survey of
2500 persons, 15 years of age and older, that herbal remedies were used by 38%
of respondents, up from 28% in 1999. A survey in 1998 of the most popular
remedies reported in Canada is given in Table 4. In 1994, the European herbal
medicine market was worth over �1.8 billion [US$ 2.8 billion] at retail selling
prices. Although the UK market was smaller than that of Germany (in 1994 it was
�88 million, compared with �1400 million), it had one of the highest forecast
growth rates in Europe (Shaw, 1998).
Table 4: Top 10 most popular herbal remedies in Canadaa
|
Echinacea
|
54
|
19
|
|
Garlic (Allium
sativum)
|
52
|
18
|
|
Ginsengb
|
42
|
15
|
|
Camomile
(Chamomilla recutita)c
|
38
|
13
|
|
Ginkgo
biloba
|
20
|
7
|
|
Evening
primrose (Oenothera biennis)
|
20
|
7
|
|
Devil�s
claw (Harpagoghytum procumbens)
|
17 ���������
|
6
|
|
St
John�s wort (Hypericum perforatum)
|
17
|
6
|
|
Tea tree
oil (Melaleuca alternifolia)
|
15
|
5
|
|
Valerian
(Valeriana officinalis)
|
13
|
5
|
From Non-Prescription Drug Manufacturers Association of
Canada (1998), Sibbald (1999) and Schultz et al. (2001)
a. From a survey of 6849 adults in April 1998
b. See Table 3.
c. Reported previously as Matricaria chamomilla (WHO, 1999)
The European market for herbal medicinal products was
estimated to be worth $5.6 billion at public price level in 1995 (AESGP, 1998).
3. Awareness, Control, Regulation and Legislation on Use
3.1 WHO guidelines for herbal medicines
In 1992, the WHO Regional Office
for the Western Pacific invited a group of experts to develop criteria and
general principles to guide research work on evaluating herbal medicines (WHO,
1993). This group recognized the importance of herbal medicines to the health
of many people throughout the world, stating: �A few herbal medicines have
withstood scientific testing, but others are used simply for traditional reasons
to protect, restore, or improve health. Most herbal medicines still need to be
studied scientifically, although the experience obtained from their traditional
use over the years should not be ignored. As there is not enough evidence
produced by common scientific approaches to answer questions of safety and
efficacy about most of the herbal medicines now in use, the rational use and
further development of herbal medicines will be supported by further
appropriate scientific studies of these products, and thus the development of
criteria for such studies�.
The document covered such topics
as developing protocols for clinical trials using herbal medicines, evaluating
herbal medicine research, guidelines for quality specifications of plant
materials and preparations, and guidelines for pharmacodynamic and general
pharmacological studies of herbal medicines and for toxicity investigations of
herbal medicines.
WHO has also issued Guidelines
for the Assessment of Herbal Medicines (WHO, 1996). These guidelines defined
the basic criteria for the evaluation of quality, safety and efficacy of herbal
medicines with the goal of assisting national regulatory authorities,
scientific organizations and manufacturers in assessing documentation,
submissions and dossiers in respect of such products. It was recommended that
such assessments take into account long-term use in the country (over at least
several decades), any description in the medical and pharmaceutical literature
or similar sources or documentation of knowledge on the application of a herbal
medicine, and marketing authorizations for similar products. Although prolonged
and apparently uneventful use of a substance usually offers testimony of its
safety, investigation of the potential toxicity of naturally occurring
substances may reveal previously unsuspected problems. It was also recommended
that regulatory authorities have the authority to respond promptly to new
information on toxicity by withdrawing or limiting the licenses of registered
products containing suspect substances, or by reclassifying the substances to
limit their use to medical prescription. The guidelines stressed the need for
assessment of efficacy including the determination of pharmacological and
clinical effects of the active ingredients, and labeling which includes a
quantitative list of active ingredient(s), dosage, and contraindications.
3.2 The European Union
The Association Europ�enne des
Sp�cialit�s Pharmaceutiques Grand Public (Association of the European
Self-Medication Industry; AESGP) has carried out a study for the European
Commission on herbal medicinal products in the European Union (EU).
The following summary is taken
from this report (AESGP, 1998).
The importance of herbal
medicinal products varies from one country to another.
These products are not a
homogeneous group. In general, they are either fully licensed medicinal
products with efficacy proven by clinical studies or by references to published
scientific literature (in accordance with Article 4.8 a (ii) of Council
Directive 65/65/EEC) (European Commission, 1965) or are available as products
with a more or less simplified proof of efficacy according to their national
use. Many Member States have these two categories, but there are major
discrepancies between the Member States in the classification of individual
herbal drug preparations and products into one of these categories as well as
in the requirements for obtaining a marketing authorization.
SOME TRADITIONAL HERBAL MEDICINES
3.2.1 Definition of herbal
medicinal products
According to Council Directive
65/65/EEC (European Commission, 1965), which has been implemented in national
law in all Member States, medicinal products require prior marketing approval
before gaining access to the market. In almost all Member States, herbal
medicinal products are considered as medicinal products, and are, in principle,
subject to the general regulations for medicines as laid down in the various
national medicine laws. In many cases, a specific definition of herbal
medicinal products is available, which is in line with the EU Guideline
�Quality of Herbal Medicinal Products�. This includes plants, parts of plants
and their preparations, mostly presented with therapeutic or prophylactic
claims. Different categories of medicinal products containing plant
preparations exist or are in the process of being created. For instance, draft
legislation in Spain includes the definitions �herbal medicinal products� and
�phytotraditional products�. The latter are not considered as �pharmaceutical
specialties� and are therefore not classified as herbal medicinal products.
3.2.2 Classification of herbal products
Generally, herbal products are
classified as medicinal products if they claim therapeutic or prophylactic
indication, and are not considered as medicinal products when they do not make
these claims. Products not classified as medicinal in most cases belong to the
food or cosmetic areas, although they sometimes contain plants which have
pharmacological properties. For example, senna pods (from Cassia plants, used
as laxatives) (see General Remarks and monograph on Rubia tinctorum, Morinda
officinalis and anthraquinones in this volume) can be marketed as food in
Belgium. Specific categories of non-medicinal products exist in some Member
States, such as the so-called �therapeutic supplement products� in Austria. In
Ireland, Spain and the United Kingdom, there exist preparations defined as
medicinal products, which are under specific conditions exempt from licensing
requirements.
3.2.3 Combination products
Herbal ingredients used in
combination are widely used in Europe, and their assessment is often performed
according to specific guidelines. Combinations of herbal and homeopathic
ingredients exist in a few countries. Their assessment follows rather strict
criteria, usually those of a �full� application procedure. Combinations of
herbal ingredients and vitamins are available in many countries.
3.2.4 Documentation of quality,
safety and efficacy
A marketing authorization for a
herbal medicinal product is, in principle, granted based on an extensive
dossier in terms of proof of quality, safety and efficacy in all Member States,
with the exception of Denmark and Finland, where it is possible to use only
references to published data for herbal medicinal products. Luxembourg, in
practice, only grants marketing authorization based on the assessment of other
countries.
In principle, according to
Article 4.8 (a) (ii) of Council Directive 65/65/EEC (European Commission,
1965), the option of using reviews on published data is available in all Member
States. However, this �bibliographical� option is sometimes only available
through assessment on a case-by-case basis or not used in practice. Austria
permits this type of application for safety documentation only.
3.2.5 ESCOP and WHO monographs
European Scientific Cooperative
on Phytotherapy (ESCOP) (see Awang, 1997) or WHO monographs may be used in many
Member States as a summary of published data.
Many regulatory authorities
regard them as helpful documentation for clarifying efficacy and safety.
The European Commission (EC), the
EMEA (European Agency for the Evaluation of Medicinal Products) Executive
Director and the EMEA Management Board established the EMEA Ad Hoc Group in
1997. This Working Group is made up of representatives from the Member States
(primarily health authorities) and representatives from the European
Parliament, the EC and the European Pharmacopoeia. The Working Group has
reviewed the criteria for the demonstration of quality, pre-clinical safety and
clinical efficacy in marketing authorization applications for herbal medicinal
products as set out in the Council Directives. The Working Group has proposed
requirements for nonclinical testing of herbal drug preparations based on a
draft EC Guideline for old substances with long market histories (EMEA, 2000).
The Group has also discussed the appropriate role of scientific monographs
prepared by the WHO and ESCOP.
3.2.6 Simplified proof of
efficacy
Various traditional herbal
medicinal products exist in many Member States in addition to fully licensed
herbal medicinal products. For these products, national authorities usually
verify the safety and ensure a sufficient level of quality. For proof of
efficacy, the level of requirements is sometimes adjusted to take into account
the long-term experience and is therefore simplified. For example, a specific
simplified procedure exists in Austria, Belgium, France and Germany. Most other
countries in the EU do not use this strategy.
3.2.7 Further developed products
For herbal medicinal products
that have been proposed for non-traditional indications or are modified from
their traditional form (e.g., highly processed or special extracts), a full
license is required in most cases, and efficacy has to be proven by clinical
studies. In several countries, such products are not used.
SOME TRADITIONAL HERBAL MEDICINES
53
3.2.8 Individual supply
Herbal medicinal products (like
other medicinal products) are made up and/or supplied to individual patients
following a one-to-one consultation between patient and practitioner. Some
herbal medicinal products are made according to accepted formulae and are
prepared by pharmacists. According to Article 2.4 of Council Directive
65/65/EEC (European Commission, 1965), a marketing authorization is not needed.
A specific situation exists in the United Kingdom, where a practitioner,
according to Section 12 of the Medicines Act 1968 (Griffin, 1998), may supply
products to a customer without a license.
3.2.9 Products from foreign
countries
The quality of imported medicinal
plants and their preparations is assessed differently in different Member
States. In some cases, no specific regulations exist concerning the control of
raw materials or crude drugs, particularly for products that enter the market
as foodstuffs or other products that are not controlled in the same way as
medicinal products. Finished products are often treated as new chemical
entities with full proof of quality, safety and efficacy being required.
3.2.10 Good manufacturing
practices and quality control
All Member States apply the
manufacturing requirements of Council Directive 75/319/EEC (European
Commission, 1975) to herbal medicinal products. Starting materials for herbal
medicinal products are in principle controlled in accordance with the European
Pharmacopoeia in all Member States. Good manufacturing practice inspections are
carried out in nearly all Member States.
The European Pharmacopoeia was
created in 1964; its efforts have resulted in the creation of 83 monographs on
herbal drugs which are used either in their natural state after desiccation or
concentration or for the isolation of natural active ingredients (Council of
Europe, 1996).
3.2.11 Post-marketing
surveillance
The adverse reaction reporting
systems of the Member States also monitor herbal medicinal products if they are
authorized medicinal products. This system has demonstrated its effectiveness
in the case of several withdrawals of marketing authorizations for herbal
medicinal products due to safety concern in connection with certain plants.
Consumer reports could provide a
picture of the spectrum of adverse reactions to herbal medicinal products and
alert authorities to potential problems; the degree of acceptance of such
reports varies between Member States.
3.2.12 Advertising, distribution
and retail sale
All Member States have
implemented Council Directive 92/28/EEC (European Commission, 1992a) on
advertising in national law. This directive covers herbal products if they are
authorized as medicinal products.
Wholesale marketing of all
medicinal products as well as authorized herbal medicinal products is covered
by Council Directive 92/25/EEC (European Commission, 1992b). The retail sale of
herbal medicinal products is restricted to pharmacies in Belgium, France,
Greece, Ireland, Italy, Luxembourg, Portugal and Spain. It is permitted in
other outlets in the case of certain herbal medicinal products in Austria,
Denmark, Finland, Germany, the Netherlands, Sweden and the United Kingdom.
Distance selling and teleshopping are not permitted for herbal medicinal
products in most countries.
3.2.13 Differences between Member
States
Herbal medicinal products are
regarded as medicinal products in most of the Member States and have, in
theory, the option of obtaining marketing authorization in the same way as all
other medicinal products. However, the legal systems of the Member States
differ in the classification of herbal products, in the availability of an
application process for a marketing authorization based on a full application,
bibliographical application or simplified proof of efficacy, and in the
permitted outlets for retail distribution. Member States have different
traditions regarding the therapeutic use of medicinal plant preparations, which
may make it more difficult for manufacturers of herbal medicinal products to
apply for marketing authorization using the decentralized procedure.
3.3 Individual countries
(Calixto, 2000)
3.3.1 France
The French Medicines Agency
(Agence du M�dicament) grants marketing authorizations based on abridged
dossiers by making reference to traditional use. The shortened procedure
requires limited or no pharmacological, toxicological and clinical tests and is
detailed in the Agency Instructions No. 3. The list of drugs with accepted traditional
uses was first published in 1985 by the Ministry of Health and has subsequently
been revised several times (Table 5). Traditional use of approximately 200
herbal drugs or preparations derived from these drugs has been recognized for
minor indications. Agency Instructions No. 3 includes rules for labeling and
packaging of herbal medicinal products. If the drug is not specifically
included in the list, there is no option to use an abridged procedure (AESGP,
1998). As of 1997, local medicinal plants were on the A list of the French
Pharmacopoeia (Castot et al., 1997) which groups the 454 herbs which
benefit/risk ratio is considered as positive when traditionally used.
SOME TRADITIONAL HERBAL MEDICINES
Table 5: Examples of plants and indications from
the French Agency Instructions
No. 3 (Cahiers de l�Agence No. 3) (Agence du
M�dicament)
|
Medicinal plant
|
Information for the medical profession
|
Information for the public
|
|
Valeriana
Officinalis
|
Traditionally
used in the symptomatic
treatment
of neurotonic conditions of adults
and
children, notably in cases of mild
sleeping
disorders
|
Traditionally
used to reduce nervousness
in
adults and children, notably in case of
sleeping
disorders
|
|
Matricaria
Chamomilla
|
Traditionally
used topically as a soothing and antipruriginous application for
dermatological ailments and as a protective treatment for cracks, grazes,
chapped skin and insect bites.
Traditionally
used in the symptomatic treatment of digestive upsets such as epigastric
distension, slow digestion, eructation and flatulence.
Traditionally
used to stimulate appetite.
Traditionally
used in cases of eye irritation or
discomfort
due to various causes (smoky
atmospheres,
sustained visual effort,
swimming
in the sea or swimming baths,
etc.).
Traditionally
used locally (mouth and throat
washes,
lozenges) as an analgesic in
conditions
of the oral cavity and/or larynx.
|
Traditionally
used topically as a soothing application and to calm the itching of skin ailments
and in cases of cracks, grazes, chapped skin and insect bites.
Traditionally
used to promote digestion.
Traditionally
used to stimulate appetite.
Traditionally
used in cases of eye
irritation
or discomfort due to various
causes
(smoky atmospheres, sustained
visual
effort, swimming in the sea or
swimming
baths, etc.). (Precaution: use
only for
mild conditions. If the symptoms
increase
or persist for more than two
days,
consult a doctor).
Traditionally
used for the temporary relief
of sore
throat and/or transient hoarseness.
|
|
Cassia
sennaa
|
Short-term
treatment of occasional
constipation.
|
This
medicinal product is a stimulant
laxative;
it stimulates bowel evacuation.
It is
intended for the short-term treatment
of
occasional constipation.
|
|
Hypericum
Perforatum
|
Traditionally
used topically as a soothing and
antipruriginous
application for dermatological
ailments
and as a protective treatment for
cracks,
grazes, chapped skin and insect bites.
Traditionally
used for sunburn, superficial
burns or
small area and nappy rash.
Traditionally
used locally (mouth and throat
washes,
lozenges) as an analgesic in
conditions
of the oral cavity and/or larynx.
|
Traditionally
used topically as a soothing
application
and to calm the itching of skin
ailments
and in cases of cracks, grazes,
chapped
skin and insect bites (Precaution:
do not
use before exposure to the sun).
Traditionally
used for sunburn,
superficial
burns or small area and nappy
rash
(Precaution: do not use before
exposure
to the sun).
Traditionally
used for the temporary relief
of sore
throat and/or transient hoarseness.
|
|
Plantago
major L.
|
Traditionally
used topically as a soothing and
antipruriginous
application for dermatological
ailments
and as a protective treatment for
cracks,
grazes, chapped skin and insect bites.
Traditionally
used in cases of eye irritation or
discomfort
due to various causes (smoky
atmospheres,
sustained visual effort,
swimming
in the sea or swimming baths,
etc.).
|
Traditionally
used topically as a soothing
application
and to calm the itching of skin
ailments
and in cases of cracks, grazes,
chapped
skin and insect bites (Precaution:
do not
use before exposure to the sun).
Traditionally
used in cases of eye
irritation
or discomfort due to various
causes
(smoky atmospheres, sustained
visual
effort, swimming in the sea or
swimming
baths, etc.). (Precaution: use
only for
mild conditions. If the symptoms
increase
or persist for more than two
days,
consult a doctor).
|
From AESGP (1998)
a. See General Remarks
Castot et al. (1997) have
reviewed the surveillance or pharmacovigilance of herbal medicines in France.
Between 1 and 15 October 1996, the authors observed 15 publications or
publicities in 23 magazines widely available in France; these publications/
publicities offered for sale by mail a number of medicinal plants found or not found
on the list of 34 �approved� plants. (These plants were listed in 1979 by the
government in reason of lack of reported toxicity in traditional use or
following complete bibliographic investigation.)
Between 1985 and 1995, the French
national surveillance system registered 341 cases of undesirable effects
possibly linked to herbal medicines; this figure represents only 0.35% of the
total adverse effects from all drugs reported during the same period.
The number of adverse effects
from herbal medicines is almost certainly under-reported.
The population concerned was
largely female (73%) with a mean age of 50 years; reasons for taking herbal
medicines were constipation, obesity and anxiety. Undesirable effects reported
were quite diverse, including allergic and cutaneous responses, eczema, liver
damage (linked to germander (Teucrium chamaedrys, tonic, diuretic)), digestive
problems (linked to laxative plants), neurological effects such as vertigo
(linked to plants classified as sedatives) and blood pressure fall and
hypokalaemia (linked to plant laxatives containing anthraquinones (see
monograph in this volume)). Outcome of these cases was generally favourable
(Castot et al., 1997).3.3.2 Germany (see Kraft, 1999; Calixto, 2000)
Keller (1991) summarized the legal
requirements for the use of phytopharmaceutical drugs in the Federal Republic
of Germany. The legal status for herbal remedies was defined by the Medicines
Act of 24 August 1976. For finished drugs a marketing authorization is
obligatory. Herbal finished drugs have to comply with the same criteria for
quality, safety and efficacy as all other finished drugs. Finished herbal drugs
may be authorized for marketing in one of three ways:
(i) Evaluation and validation of
old medicines. Finished drugs registered in 1978 possessed a provisional
marketing authorization and could remain on the market until the end of April
1990. The medical evaluation of these drugs was mainly based on published data
and was carried out by a special expert committee, the Commission E (Expert
Commission for Herbal Remedies). The preparation of new monographs by
Commission E ended in 1993 (Sandberg & Corrigan, 2001).
(ii) Standardized marketing
authorization. Medicines that do not represent a direct or indirect risk for
health can be exempted from the need for an individual marketing authorization
by reference to a previously existing monograph.
(iii) Individual application for
marketing authorization. In this procedure, complete documentation including
the results of analytical tests, results of pharmacological and toxicological
tests and results of clinical or other medical tests are required.
In addition, drugs sold outside
pharmacies and only for traditional uses without clinical evidence for efficacy
have to be labeled as �traditionally used� (Table 6).
3.3.3 United Kingdom
A number of papers have discussed
the situation regarding herbal medicines in the United Kingdom. De Smet (1995)
recommended that herbal products be licensed as special products �medicines�;
he estimated that unlicensed preparations accounted for over 80% of herbal
sales. Many medicine-like products on the British herbal market remain
unregistered for two reasons: acceptable data on efficacy, safety and quality
may not be available, and the licensing fee is high. Traditional experience
with herbs can be a useful tool in detecting acute toxicity, but is less useful
in detecting rare adverse reactions or those that develop after long-term
exposure or after a latent period.
Therefore, traditional experience
needs to be supplemented with orthodox data from research and post-marketing
surveillance. Such post-marketing surveillance is only partly helpful, as
herbal suppliers and traditional practitioners are not obliged to report
suspected adverse reactions and herbal products are of variable quality.
Table 6: Examples of plants and indications from the German
�traditional� list
Active ingredients Dosage form Indication �Traditionally
used for ��
Ginseng root (liquid extract prepared with wine)
Liquid for oral administration
Improvement of the general condition St John�s wort (aqueous
liquid extract)
Liquid for oral administration
Improvement of the condition in case of nervous stress
Garlic + mistle herb + hawthorn flowering tops
Sugar-coated tablets Support of cardiovascular function
Garlic oil Gastro-resistant capsules
For prevention of general atherosclerosis
Hamamelis leaf (aqueous liquid extract)
Cream Support of skin function
Ginger + juniper berries Tables Support of digestive
function
Onion (oily viscous extract) Capsules Prevention of general
atherosclerosis
Melissa leaf Sugar-coated tablets Improvement of the
condition in case of nervous stress, for support of stomach function
Dandelion root (aqueous solid extract)
Capsules Support of the excretory function of the kidney
Adapted from AESGP (1998)
Shaw (1998) has discussed the safety aspects of herbal
remedies in the United Kingdom. The legal status of herbal remedies/medicines
in the United Kingdom can be broadly divided into three categories:
(i) Most herbal products are unlicensed and therefore no
medicinal claims can be made. These are regarded as food supplements and come
under food legislation (Ministry of Agriculture, Fisheries and Food (MAFF),
1998).
(ii) Licensed medicinal products require evidence of
quality, safety and efficacy and are regulated by the Medicines Control Agency.
(iii) Herbal medicines supplied by a herbalist are exempt
from licensing under the 1968 Medicines Act.
Since 1996, the Medicines Control
Agency has included adverse reaction reports on unlicensed herbal remedies
within its remit and now monitors all three categories (Griffin, 1998).
The House of Lords Science and
Technology Committee in early 1999 reviewed a large amount of oral and written
evidence from a wide variety of sources in order to scrutinize complementary
and alternative medicine (CAM) including herbal medicines (Mills, 2001). The
report noted that public satisfaction with CAM was high and that use of CAM was
increasing. Evidence was required that CAM has an effect above and beyond
placebo, and this information needed to be available to the public. The current
lack of regulation of CAM did not protect the public interest adequately.
Acupuncture and herbal medicine should be subject to statutory regulation under
the Health Act 1999, as should possibly non-medical homeopathy. The regulatory
status of herbal medicines was viewed as particularly unsatisfactory. The
report recommended that training for CAM professionals should be standardized
and independently accredited and, for many, should include basic biomedical
science. Conventional health professionals should become more familiar with CAM
and those working in the best-regulated CAM professions should work towards
integration with conventional medicine.
3.3.4 United States
In the USA, the Food Drug and
Cosmetics Act characterizes a product primarily on the basis of its intended
use. For a botanical product, this intended use may be as a food (including a
dietary supplement), a drug (including a biological drug), a medical device
(e.g., gutta-percha) or a cosmetic as shown by, among other things, the
products� accompanying labeling claims, advertising materials, and oral or
written statements (21 Code of Federal Regulations (CFR) 201.128) (Food and
Drug Administration (FDA), 2000).
For products classified as drugs,
the FDA regulates them under the authority of the Food Drug and Cosmetics Act
and its amendments. Under current regulations, if there is no marketing history
in the USA for a botanical drug product, if available evidence of safety and
effectiveness does not warrant inclusion of the product in an existing,
approved category of OTC (over-the-counter) drugs, or if the proposed
indication would not be appropriate for non-prescription use, the manufacturer
must submit a new drug application to obtain FDA approval to market the product
for the proposed use. If existing information on the safety and efficacy of a
botanical drug product is insufficient to support a new drug application, new
clinical studies will be needed to demonstrate safety and effectiveness.
Most botanical products in the
USA are marketed as dietary supplements. Under the Dietary Supplement Health
and Education Act of 1994 (DSHEA), an orally ingested product that meets the
definition of a �dietary supplement� under section 201(ff) of the Food Drug and
Cosmetics Act may be lawfully marketed using a statement that (1) claims a
benefit related to a classical nutrient deficiency disease (and discloses the
prevalence of the disease in the USA); (2) describes how the product is
intended to affect the structure or function of the human body; (3)
characterizes the documented mechanism by which the product acts to maintain
such structure or function; or (4) describes general well-being derived from
consumption of the product (section 403 r (6)(A) of the Food Drug and Cosmetics
Act, 21 U.S.C. 343 r(6)(A)). The term �dietary supplement� is defined in
section 201 (ff) of the Act and means a product (other than tobacco) intended
to supplement the diet that contains one or more of certain dietary
ingredients, such as a vitamin, a mineral, a herb or another botanical
substance, an amino acid, a dietary substance for use by people to supplement
the diet by increasing the total dietary intake, or a concentrate, metabolite,
constituent, extract, or combination of the preceding ingredients (Chang,
1999). A dietary supplement is a product that is intended for ingestion in a
form described in section 411C(1)(B)(i) of the Act (i.e., tablet, capsule
powder, softgel, gelcap and liquid), which is not represented as conventional
food, or as the sole item of a meal or of the diet, and which is labelled as a
dietary supplement. It is the responsibility of the manufacturer to ensure that
a dietary ingredient used in a dietary supplement is safe for its intended use.
The FDA has issued regulations
defining the types of statement that can be made concerning the effect of a
dietary supplement on the structure and function of the body.
The regulations distinguish these
statements from the types of statement that require prior approval as drug
claims or prior authorization as health claims.
Safety monitoring of dietary
supplements focuses on the post-marketing period. The FDA receives spontaneous
reports of suspected adverse events through a variety of means, including
through a programme called MEDWATCH, the FDA Medical Products Reporting Program
(Goldman & Kennedy, 1998). The post-marketing surveillance system for foods
and dietary supplements, called the Adverse Event Reporting Systems, is a
passive system that relies on voluntary reporting by concerned parties,
primarily health professionals and consumers (AESGP, 1998).
The DSHEA extended the definition
of dietary supplements beyond vitamins and minerals and established a formal
definition of a dietary supplement using new criteria.
The Congressionally mandated
Commission on Dietary Supplement Labels (CDSL) suggested that some botanicals
may qualify as OTC products under existing statutes; these state that a product
may avoid �new drug� premarket approval requirements and may be eligible for
marketing under an OTC drug monograph if the product is generally recognized as
safe (GRAS) and effective under the conditions for use for which it is labelled
and if the product has been used �to a material extent and for a material time�
under those conditions. The FDA�s response to the Commission stated that it
does not regard marketing experience outside the USA to meet conditions of
historical use.
Angell and Kassirer (1998) stated
that the primary factor that sets alternative medicine, including its most
common form, herbal medicine, apart from conventional medicine is �that it has
not been scientifically tested and its advocates largely deny the need for such
testing�. Angell and Kassirer defined �testing� as the gathering of evidence of
safety and efficacy, as required by the FDA. �There cannot be two kinds of
medicine � conventional and alternative. There is only medicine that has been
adequately tested and medicine that has not, medicine that works and medicine
that may or may not work.
Once a treatment has been tested
rigorously, it no longer matters whether it was considered alternative at the
outset. If it is found to be reasonably safe and effective, it will be
accepted. Alternative treatments should be subjected to scientific testing no
less rigorous than that required for conventional treatments�.
SOME TRADITIONAL HERBAL MEDICINES
3.3.5 Canada
The Canadian Food and Drug Act
and findings of an Expert Advisory Committee on Herbs and Botanical
Preparations were consulted by Kozyrskyj (1997) to provide an overview of the
issues regarding regulation of herbal products in Canada. Case reports of
herbal toxicity were identified to illustrate some of the hazards of herbal
products, and references were provided to guide health professionals in
searching the literature for clinical trials that have evaluated the efficacy
of these drugs.
Herbal products not registered as
drugs in Canada are sold as foods and are thus exempt from the drug review
process that evaluates product efficacy and safety. An Expert Advisory
Committee on Herbs and Botanical Preparations was formed in 1984 to advise the
Health Protection Branch (HPB). HPB published lists of hazardous herbal
products in 1987, 1989, 1992 and 1993. The last publication elicited a large
response from consumers and the herbal industry. As of 1995, the list was still
under review (Kozyrskyj 1997).
The recently formed Office of
Natural Health Products (currently the Natural Health Products Directorate)
(Sibbald, 1999) is responsible for all regulatory functions including, but not
limited to pre-market assessment for product labeling, licensing of
manufacturers, post-approval monitoring and compliance and implementation of
the recommendations of the standing House Health Committee.
In December 2000, the provincial
government of British Columbia approved regulations that established
traditional Chinese medicine as an alternative form of primary health care. The
cost is not covered under Canadian medicare and practitioners face several
practice restrictions. For example, �no acupuncturist or herbalist may treat an
active serious medical condition unless the client has consulted with a medical
practitioner, naturopath or dentist or doctor of traditional Chinese medicine,
as appropriate� (Johnson, 2001).
3.3.6 Chile
In 1992 the Unidad de Medicina
Tradicional was established with the aims of incorporating traditional medicine
with proven efficacy into health programmes and of contributing to the
establishment of their practice. Herbal medicines are legally differentiated
into: (a) drugs intended to cure, alleviate or prevent diseases; (b) food
products for medicinal use and with therapeutic properties; and (c) food
products for nutritional purposes (Calixto, 2000).
Herbal products with therapeutic
indications and/or dosage recommendations are considered to be drugs.
Distribution of these products is restricted to pharmacies. Aregistration for
marketing authorization is needed for herbal products, homeopathic products,
and other natural products. An application for such registration consists of
the complete formula, the labeling, samples of the product, and a monograph
which permits identification of the formula and characteristics of the product
(Zhang, 1998).
3.3.7 Japan (Zhang, 1998; Eguchi
et al., 2000; Saito, 2000)
Japanese traditional medicine, as
used in Japanese society for more than a thousand years, may be divided into
folk medicine and Chinese medicine (or Kampo medicine). Kampo medicine is so
popular that the per capita consumption of herbal medicine in Japan seems to be
the highest in the world. One hundred and forty-six Kampo drugs are registered
as drugs by the Ministry of Health and Welfare (MHW) and are included in
coverage under the National Health Insurance. Acceptance of Kampo drugs took
place without clinical validation studies. In 1989, about 80% of physicians
reported prescribing Chinese medicine. Physicians generally recognize Chinese
medicine as a complement to modern medicine; traditional drugs are viewed in
Japanese society as safe.
Raw herbs which have long been
used as folk medicine and which have also been used for a considerable period
as components of an industrial product are each described in a corresponding
monograph. These products are freely usable for the purposes indicated in the
monograph. Local traditional usage is not sufficient for approval as a drug;
the claims and rules of combinations of herbal ingredients are determined on
the basis of the pharmacological actions of the ingredients. If a monograph is
not available, the claims reported in the Japanese Pharmacopoeia are used as a
guide.
In the evaluation of a Chinese
medicine, importance is given to �empirical facts or experience�, such as
reference data, clinical test reports, etc., rather than the pharmacological
action of each ingredient. Safety and efficacy have been estimated based on
general methods employed by modern medical science. In 1972 the MHW designated
210 formulae as OTC drugs; this selection was based primarily on the experience
of doctors actually practising traditional Chinese medicine. In 1976, the MHW
specified 146 formulations as �National Health Insurance (NHI) applicable
prescription drugs�. In the case of an application for approval of a
prescription drug other than those previously listed, specified data on safety,
stability, comparison with other drugs, clinical test results, etc. must be
submitted.
New Kampo drugs are regulated in
essentially the same way as �western� drugs in Japan. The same data required
for new �western� drugs are required for new Kampo drugs, including data from
three-phase clinical trials.
Since 1971, the MHW has been
running a programme for re-evaluation of all drugs marketed before 1967; a new
system to re-evaluate the efficacy and safety for all drugs every five years
was launched in 1988.
An Advisory Committee for Kampo
drugs was established in 1982 in close association with the MHW in order to
improve quality control of Kampo drugs. Since the 1986 Good Manufacturing
Practice Law, the standard applied to all pharmaceutical drugs has also applied
to Kampo drugs. In addition, in 1985, guidelines for ethical extract products
in oriental medicine formulations were developed.
The MHW has three major systems
for collection of adverse reaction data. The first is a voluntary system involving
2915 monitoring hospitals. The second system � the Pharmacy Monitoring System �
which includes 2733 pharmacies, collects data on cases SOME TRADITIONAL HERBAL
MEDICINES 63 of adverse reactions to OTC drugs. The third system is Adverse
Reaction Reporting from Manufacturers. These cases are reported to the MHW by
the responsible company, with information arising from medical conferences and
from journals.
3.3.8 Korea (Republic of)
The Pharmaceutical Act of 1993
explicitly allowed pharmacists to prescribe and dispense herbal drugs (Cho,
2000).
3.3.9 China
Many herbal medicines have been
used for hundreds of years and it is assumed in many cases that they must work.
For example, about 7000 species of plants are used in China as herbal
medicines, but only 230 of the most commonly used ones have been subject to
in-depth pharmacological, analytical and clinical studies.
The 2000 edition of the Chinese
pharmacopoeia included 784 items on traditional Chinese medicines and 509 on
Chinese patent medicines. Herbal medicines in China are normally considered as
medicinal products with special requirements for marketing.
New drugs have to be investigated
and approved according to the Drug Administration Law. New traditional Chinese
medicines are classified under five categories based on the Amendment and
Supplement Regulation of Approval of new traditional medicines:
Class 1
(1) Artificial alternatives of Chinese crude drugs.
(2) Newly discovered Chinese crude drugs and their
preparations.
(3) Active constituents extracted from Chinese crude drugs
and their preparations.
(4) Active constituents extracted from a composite
formulation of traditional Chinese medicines.
Class 2
(1) Injection of traditional Chinese medicines
(2) Use of new medicinal parts of Chinese crude drugs and
their preparations.
(3) Effective fractions extracted from Chinese crude drugs
or natural drugs and their preparations.
(4) Chinese crude drugs artificially developed in an animal
body and their preparations.
(5) Effective fractions extracted from a composite
formulation.
Class 3
(1) New composite formulations of traditional Chinese
medicines.
(2) Composite preparations of traditional Chinese medicines
and chemical drugs with the main efficacy due to the traditional Chinese
medicine.
(3) Domestically cultivated or bred crude drugs originally
imported and commonly used in China, and their preparations.
Class 4
(1) Preparation with a change of dosage form or route of
administration.
(2) Botanical crude drugs acclimatized from their origin, or
crude drugs from a domesticated wild animal in China.
Class 5
Marketing drugs with new indications or syndromes.
In Hong Kong in 1989, the
Government appointed a Working Party to review and make recommendations for the
use and practice of traditional Chinese medicines. In 1995 the preparatory
Committee on Chinese medicines was formed to manage the implementation of these
recommendations: as a result 31 potent Chinese medicines that may potentially
cause adverse effects have been identified. Proprietary preparations containing
a combination of herbal ingredients and conventional drugs are regulated in the
same manner as other conventional drugs.
The majority of suppliers are
state-owned or state-connected. The extensive pharmacopoeia relating to
traditional Chinese medicine allows the parallel manufacturing and sale of both
pharmaceutical drugs and traditional herbal blends (Chan, 1997; Zhang, 1998).
3.3.10 Saudi Arabia
Registration of medicinal
products by the Ministry of Health is obligatory, as is that of products, in
addition to drugs, with medicinal claims or containing active ingredients
having medicinal effects such as herbal preparations, health and supplementary
food, medicated cosmetics, antiseptics or medical devices (Zhang, 1998).
3.3.11 South Africa (Zhang, 1998)
The trade in crude indigenous
herbal products is completely unregulated. A large number of South Africans
consult traditional healers, generally in addition to medical practitioners.
There are about 200,000 traditional healers in the country.
Once a health-related claim is
made for a finished herbal product, that product must go through a full drug
evaluation in the Medicines Control Council (MCC) before marketing.
Specific regulations for
registration and control of new �traditional� herbal medicines do not exist.
Old medicines, including such well known herbal medicines as senna or aloe, are
already registered by the MCC, according to internationally accepted standards
of efficacy and safety. Pharmaceutical standards need to be consistent with
those of the United States Pharmacopeia or the British Pharmacopoeia.
SOME TRADITIONAL HERBAL MEDICINES
3.3.12 Australia and New Zealand
(Moulds & McNeil, 1988; Zhang, 1998)
The Therapeutic Goods Act 1989
sets out the legal requirements for the import, export, manufacture and supply
of medicines in Australia. It details the requirements for listing or
registering all therapeutic goods in the Australian Register of Therapeutic
Goods (ARTG), as well as many other aspects of the law including advertising, labeling
and product appearance. Australian manufacturers of therapeutic goods must be
licensed and their manufacturing processes must comply with the principles of
Good Manufacturing Practice (GMP). All medicines manufactured for supply in
Australia must be listed or registered in the ARTG, unless they are
specifically exempt or excluded. Listed medicines are considered to be of lower
risk than registered medicines. Most complementary medicines (e.g., herbal,
vitamin and mineral products) are examples of listed products.
Medicines assessed as having a
higher level of risk must be registered (not listed). Registered medicines
include non-prescription (low-risk, OTC) medicines and prescription (high-risk)
medicines. Complementary medicines (also known as �traditional� or
�alternative� medicines) include vitamin, mineral, herbal, aromatherapy and
homeopathic products. Complementary medicines may be either listed or
registered, depending on their ingredients and the claims made. Most
complementary medicines are listed in the ARTG and some are registered
(Therapeutics Good Administration, 1999).
In New Zealand, supplements in
the market place are largely manufactured in the USA. Regulations are not
restrictive; there are no limits on ingredients or potencies and �structure/function�
claims are allowed.
THE HISTORY OF HEALTH AND HEALING
IN AFRICA
Over the past two decades or so,
historians have developed a complex literature on the history of health and
healing in Africa. This course examines why the topic of health and healing
occupies such a central role in our understanding of Africa�s pasts.
Drawing on the works of both
historians and anthropologists, we explore the creative and shifting ways in
which Africans have sought to compose healthy communities through the expansion
of therapeutic repertoires. The course covers a wide chronological span and
considers a variety of topics, including: faith and healing; therapy management
and medical pluralism; debility and bodily misfortune; the use of
contraceptives; epidemics and colonial planning; the HIV/AIDS epidemic; and the
relationship between public healing and political authority. This is a
fascinating history of how changes in health and healing are inseparable from
broader changes in control over political institutions and the organization of
economic production. It is a history situated at the core of some of the most
critical challenges facing contemporary African societies and one that
therefore begs for critical understanding.
(back
to content)
2.3 Herbal medicine c
Herbal medicine (also herbalism)
is the study of pharmacognosy and the use of medicinal plants, which are a basis
of traditional medicine. There is limited scientific evidence for the
safety and efficacy of plants used in 21st century herbalism, which generally does
not provide standards for purity or dosage. The scope of herbal medicine
commonly includes fungal and bee products, as well as minerals, shells and
certain animal parts. Herbal medicine is also called phytomedicine or
phytotherapy.
�
An antique selection of herbal medicines
Paraherbalism describes
alternative and pseudoscientific practices of using unrefined plant
or animal extracts as unproven medicines or health-promoting agents.
Paraherbalism relies on the belief that preserving various substances from a
given source with less processing is safer or more effective than manufactured
products, a concept for which there is no evidence.
History
 �
�
A physician preparing an elixir, from an Arabic version of
Dioscorides's pharmacopoeia, 1224
Archaeological evidence indicates
that the use of medicinal plants dates back to the Paleolithic age,
approximately 60,000 years ago. Written evidence of herbal remedies dates back
over 5,000 years to the Sumerians, who compiled lists of plants. Some ancient
cultures wrote about plants and their medical uses in books called herbals. In
ancient Egypt, herbs are mentioned in Egyptian medical papyri, depicted in tomb
illustrations, or on rare occasions found in medical jars containing trace
amounts of herbs. In ancient Egypt, the Ebers papyrus dates from about 1550 BC,
and covers more than 700 compounds, mainly of plant origin. The earliest known
Greek herbals came from Theophrastus of Eresos who, in the 4th century BC,
wrote in Greek Historia Plantarum, from Diocles of Carystus who wrote during
the 3rd century BC, and from Krateuas who wrote in the 1st century BC. Only a
few fragments of these works have survived intact, but from what remains,
scholars noted overlap with the Egyptian herbals. Seeds likely used for herbalism
were found in archaeological sites of Bronze Age China dating from the Shang
dynasty (c. 1600�1046 BC). Over a hundred of the 224 compounds mentioned in the
Huangdi Neijing, an early Chinese medical text, are herbs. Herbs were also commonly
used in the traditional medicine of ancient India, where the principal
treatment for diseases was diet.� De
Materia Medica, originally written in Greek by Pedanius Dioscorides (c. 40�90
AD) of Anazarbus, Cilicia, a physician and botanist, is one example of herbal
writing used over centuries until the 1600s.
MODERN HERBAL MEDICINE
The World Health Organization
(WHO) estimates that 80 percent of the population of some Asian and African
countries presently use herbal medicine for some aspect of primary health care.
Some prescription drugs have a basis as herbal remedies,
including artemisinin, digitalis, quinine and taxanes.
REGULATORY REVIEW
In 2015, the Australian
Government's Department of Health published the results of a review of
alternative therapies that sought to determine if any were suitable for being
covered by health insurance; herbalism was one of 17 topics evaluated for which
no clear evidence of effectiveness was found. Establishing guidelines to assess
safety and efficacy of herbal products, the European Medicines Agency provided
criteria in 2017 for evaluating and grading the quality of clinical research in
preparing monographs about herbal products. In the United States, the National
Center for Complementary and Integrative Health of the National Institutes of
Health funds clinical trials on herbal compounds, provides fact sheets
evaluating the safety, potential effectiveness and side effects of many plant
sources, and maintains a registry� of
clinical research conducted on herbal products.
According to Cancer Research UK
as of 2015, "there is currently no strong evidence from studies in people
that herbal remedies can treat, prevent or cure cancer".
PREVALENCE OF USE
The use of herbal remedies is
more prevalent in people with chronic diseases, such as cancer, diabetes,
asthma and end-stage kidney disease. Multiple factors such as gender, age,
ethnicity, education and social class are also shown to have association with
prevalence of herbal remedies use.
HERBAL PREPARATIONS
Leaves of Eucalyptus olida being packed into a steam distillation
unit to gather its essential oil
There are many forms in which
herbs can be administered, the most common of which is a liquid consumed as a
herbal tea or a (possibly diluted) plant extract.
Herbal teas, or tisanes, are the
resultant liquid of extracting herbs into water, though they are made in a few
different ways. Infusions are hot water extracts of herbs, such as chamomile or
mint, through steeping. Decoctions are the long-term boiled extracts, usually
of harder substances like roots or bark. Maceration is the cold infusion of
plants with high mucilage- content, such as sage or thyme.� To make macerates, plants are chopped and
added to cold water.� They are then left
to stand for 7 to 12 hours (depending on herb used). For most macerates, 10
hours is used.
Tinctures are alcoholic extracts
of herbs, which are generally stronger than herbal teas. Tinctures are usually
obtained by combining pure ethanol (or a mixture of pure ethanol with water)
with the herb. A completed tincture has an ethanol percentage of at least 25%
(sometimes up to 90%). Non-alcoholic tinctures can be made with glycerin but it
is believed to be less absorbed by the body than alcohol based tinctures and
has a shorter shelf life. Herbal wine and elixirs are alcoholic extract of
herbs, usually with an ethanol percentage of 12�38%. Extracts include liquid
extracts, dry extracts, and nebulisates. Liquid extracts are liquids with a
lower ethanol percentage than tinctures. They are usually made by vacuum
distilling tinctures.
Dry extracts are extracts of
plant material that are evaporated into a dry mass. They can then be further refined
to a capsule or tablet.
The exact composition of an
herbal product is influenced by the method of extraction. A tea will be
rich in polar components because water is a polar solvent. Oil on the other
hand is a non-polar solvent and it will absorb non-polar compounds. Alcohol
lies somewhere in between.
 �
�
A herb shop in the souk of Marrakesh, Morocco
Many herbs are applied topically
to the skin in a variety of forms. Essential oil extracts can be applied to the
skin, usually diluted in a carrier oil. Many essential oils can burn the skin
or are simply too high dose used straight; diluting them in olive oil or
another food grade oil such as almond oil can allow these to be used safely as
a topical.� Salves, oils, balms, creams
and lotions are other forms of topical delivery mechanisms. Most topical applications
are oil extractions of herbs. Taking a food grade oil and soaking herbs in it
for anywhere from weeks to months allows certain phytochemicals to be extracted
into the oil. This oil can then be made into salves, creams, lotions, or simply
used as an oil for topical application. Many massage oils, antibacterial
salves, and wound healing compounds are made this way.
Inhalation, as in aromatherapy, can be used as a treatment.
SAFETY
 �
�
Datura stramonium has been used in Ayurveda for various
treatments, but contains alkaloids, such as atropine and scopolamine, which may
cause severe toxicity.
Consumption of herbs may cause
adverse effects. Furthermore, "adulteration, inappropriate formulation, or
lack of understanding of plant and drug interactions have led to adverse
reactions that are sometimes life threatening or lethal." Proper
double-blind clinical trials are needed to determine the safety and efficacy of
each plant before medical use.
Although many consumers believe
that herbal medicines are safe because they are natural, herbal medicines and
synthetic drugs may interact, causing toxicity to the consumer. Herbal remedies
can also be dangerously contaminated, and herbal medicines without established
efficacy, may unknowingly be used to replace prescription medicines.
Standardization of purity and
dosage is not mandated in the United States, but even products made to the same
specification may differ as a result of biochemical variations within a
species of plant.� Plants have chemical
defense mechanisms against predators that can have adverse or lethal effects on
humans. Examples of highly toxic herbs include poison hemlock and nightshade.
They are not marketed to the public as herbs, because the risks are well known,
partly due to a long and colorful history in Europe, associated with
"sorcery", "magic" and intrigue. Although not frequent, adverse
reactions have been reported for herbs in widespread use. On occasion serious
untoward outcomes have been linked to herb consumption. A case of major
potassium depletion has been attributed to chronic licorice ingestion, and
consequently professional herbalists avoid the use of licorice where they
recognize that this may be a risk. Black cohosh has been implicated in a case
of liver failure.� Few studies are
available on the safety of herbs for pregnant women, and one study found that use
of complementary and alternative medicines are associated with a 30% lower
ongoing pregnancy and live birth rate during fertility treatment.
Examples of herbal treatments
with likely cause-effect relationships with adverse events include aconite,
which is often a legally restricted herb, ayurvedic remedies, broom, chaparral,
Chinese herb mixtures, comfrey, herbs containing certain flavonoids,
germander, guar gum, liquorice root, and pennyroyal. Examples of herbs that may
have long-term adverse effects include ginseng, which is unpopular among
herbalists for this reason, the endangered herb goldenseal, milk thistle,
senna, against which herbalists generally advise and rarely use, aloe vera
juice, buckthorn bark and berry, cascara sagrada bark, saw palmetto, valerian,
kava, which is banned in the European Union, St. John's wort, khat, betel nut,
the restricted herb ephedra, and guarana.
There is also concern with
respect to the numerous well-established interactions of herbs and drugs. In consultation
with a physician, usage of herbal remedies should be clarified, as some
herbal remedies have the potential to cause adverse drug interactions when used
in combination with various prescription and over-the-counter pharmaceuticals,
just as a patient should inform a herbalist of their consumption of orthodox
prescription and other medication.
For example, dangerously low
blood pressure may result from the combination of an herbal remedy that lowers blood
pressure together with prescription medicine that has the same effect. Some herbs
may amplify the effects of anticoagulants. Certain herbs as well as common
fruit interfere with cytochrome P450, an enzyme critical to much drug
metabolism.
In a 2018 study, FDA
identified active pharmaceutical additives in over 700 of analyzed
dietary supplements sold as "herbal", "natural" or
"traditional".� The undisclosed
additives included "unapproved antidepressants and designer
steroids", as well as prescription drugs, such as sildenafil or
sibutramine.
LABELING ACCURACY
A 2013 study found that one-third of herbal supplements
sampled contained no trace of the herb listed on the label.� The study found products adulterated with
contaminants or fillers not listed on the label, including potential
allergens such as soy, wheat, or black walnut. One bottle labeled as St. John's
wort was found to actually contain Alexandrian senna, a laxative.
Researchers at the University of
Adelaide found in 2014 that almost 20 percent of herbal remedies surveyed were
not registered with the Therapeutic Goods Administration, despite this being a
condition for their sale. They also found that nearly 60 percent of products
surveyed had ingredients that did not match what was on the label. Out of 121
products, only 15 had ingredients that matched their TGA listing and packaging.
In 2015, the New York Attorney
General issued cease and desist letters to four major U.S. retailers (GNC, Target,
Walgreens, and Walmart) who were accused of selling herbal supplements that
were mislabeled and potentially dangerous. Twenty-four products were tested by
DNA barcoding as part of the investigation, with all but five containing
DNA that did not match the product labels.
PRACTITIONERS OF HERBALISM
|
 �A herbalist gathers
the flower heads of Arnica montana �A herbalist gathers
the flower heads of Arnica montana
|
In some countries, formalized
training and minimum education standards exist for herbalists, although these
are not necessarily uniform within or between countries. In Australia, for
example, the self-regulated status of the profession (as of 2009) resulted in
variable standards of training, and numerous loosely-formed associations
setting different educational standards. One 2009 review concluded that
regulation of herbalists in Australia was needed to reduce the risk of
interaction of herbal medicines with prescription drugs, to implement clinical
guidelines and prescription of herbal products, and to assure self-regulation
for protection of public health and safety. In the United Kingdom, the training
of herbalists is done by state-funded universities offering Bachelor of Science
degrees in herbal medicine. In the United States, according to the American
Herbalist Guild, "there is currently no licensing or certification
for herbalists in any state that precludes the rights of anyone to use, dispense,
or recommend herbs." However, there are U.S. federal restrictions for
marketing herbs as cures for medical conditions, or essentially practicing as
an unlicensed physician.
UNITED STATES HERBALISM FRAUD
Over the years 2017�21, the U.S.
Food and Drug Administration (FDA) issued warning letters to numerous herbalism
companies for illegally marketing products under "conditions that cause
them to be drugs under section 201(g)(1) of the Act [21 U.S.C. � 321(g)(1)],
because they are intended for use in the diagnosis, cure, mitigation,
treatment, or prevention of disease and/or intended to affect the structure or
any function of the body" when no such evidence existed. During the
COVID-19 pandemic, the FDA and U.S. Federal Trade Commission issued warnings to
several hundred American companies for promoting false claims that herbal
products could prevent or treat COVID-19 disease.
GOVERNMENT REGULATIONS
The World Health Organization
(WHO), the specialized agency of the United Nations (UN) that is concerned with
international public health, published Quality control methods for medicinal
plant materials in 1998 to support WHO Member States in establishing quality
standards and specifications for herbal materials, within the overall
context of quality assurance and control of herbal medicines.
In the European Union (EU),
herbal medicines are regulated under the Committee on Herbal Medicinal
Products.
In the United States, herbal
remedies are regulated dietary supplements by the Food and Drug Administration
(FDA) under current good manufacturing practice (cGMP) policy for dietary
supplements. Manufacturers of products falling into this category are not
required to prove the safety or efficacy of their product so long as they do
not make 'medical' claims or imply uses other than as a 'dietary supplement',
though the FDA may withdraw a product from sale should it prove harmful.
Canadian regulations are
described by the Natural and Non-prescription Health Products Directorate which
requires an eight-digit Natural Product Number or Homeopathic Medicine Number on
the label of licensed herbal medicines or dietary supplements.
Some herbs, such as cannabis and
coca, are outright banned in most countries though coca is legal in most of the
South American countries where it is grown. The Cannabis plant is used as an
herbal medicine, and as such is legal in some parts of the world. Since 2004,
the sales of ephedra as a dietary supplement is prohibited in the United States
by the FDA, and subject to Schedule III restrictions in the United Kingdom.
SCIENTIfiC CRITICISM
Herbalism has been criticized as
a potential "minefield" of unreliable product quality, safety
hazards, and potential for misleading health advice.� Globally, there are no standards across
various herbal products to authenticate their contents, safety or efficacy, and
there is generally an absence of high-quality scientific research on
product composition or effectiveness for anti-disease activity. Presumed claims
of therapeutic benefit from herbal products, without rigorous evidence of
efficacy and safety, receive skeptical views by scientists.
Unethical practices by some
herbalists and manufacturers, which may include false advertising about health benefits
on product labels or literature, and contamination or use of fillers during
product preparation, may erode consumer confidence about services and
products.
(back
to content)
Paraherbalis m
�
An example of a herbal medicine resource:� the bark of the cinchona tree contains
quinine, which today is a widely prescribed treatment for malaria. The
unpurified bark is still used by some who can not afford to purchase more
expensive antimalarial drugs.
Paraherbalism is the
pseudoscientific use of extracts of plant or animal origin as supposed
medicines or health-promoting agents. Phytotherapy differs from plant-derived
medicines in standard pharmacology because it does not isolate and standardize
the compounds from a given plant believed to be biologically active.� It relies on the false belief that preserving
the complexity of substances from a given plant with less processing is safer and
potentially more effective, for which there is no evidence either condition
applies.
Phytochemical researcher Varro
Eugene Tyler described paraherbalism as "faulty or inferior herbalism
based on pseudoscience", using scientific terminology but lacking
scientific evidence for safety and efficacy. Tyler listed� ten fallacies that distinguished herbalism
from paraherbalism, including claims that there�
is a conspiracy to suppress safe and effective herbs, herbs can not
cause harm, that whole herbs are more effective than molecules isolated from
the plants,� herbs are superior to drugs,
the doctrine of signatures (the belief that the shape of the plant indicates
its function) is valid, dilution of substances increases their potency (a
doctrine of the pseudoscience of homeopathy), astrological alignments are
significant, animal� testing is not
appropriate to indicate human effects, anecdotal evidence is an effective means
of proving a substance works and herbs were created by God to cure disease.
Tyler suggests that none of these beliefs have any basis in fact.
TRADITIONAL SYSTEMS
�
Ready to drink macerated medicinal liquor with goji berry,
tokay gecko, and ginseng, for sale at a traditional medicine market in Xi'an,
China.
AFRICA
Up to 80% of the population in Africa uses traditional medicine
as primary health care.
AMERICAS
Native Americans used about 2,500
of the approximately 20,000 plant species that are native to North America.
In Andean healing practices, the
use of Entheogens, in particular the San Pedro cactus (Echinopsis pachanoi) is
still a vital component, and has been around for millennia.
CHINA
Some researchers trained in both Western and traditional
Chinese medicine have attempted to deconstruct ancient medical texts in the
light of modern science. In 1972, Tu Youyou, a pharmaceutical chemist,
extracted the anti-malarial drug artemisinin from sweet wormwood, a traditional
Chinese treatment for intermittent fevers.
INDIA
�
A platter of herbal medicines at Goa, India
In India, Ayurvedic medicine has
quite complex formulas with 30 or more ingredients, including a sizable number
of ingredients that have undergone "alchemical processing", chosen to
balance dosha. In Ladakh, Lahul-Spiti and Tibet, the Tibetan Medical System is
prevalent, also called the 'Amichi Medical System'. Over 337 species of
medicinal plants have been documented by C.P. Kala. Those are used by Amchis,
the practitioners of this medical system. The Indian book, Vedas, mentions
treatment of diseases with plants.
INDONESIA
�
Different types of Indonesian jamu herbal medicines held in
bottles
In Indonesia, especially among
the Javanese, the jamu traditional herbal medicine may have originated in the
Mataram Kingdom era, some 1300 years ago. The bas-reliefs on Borobudur depict the
image of people grinding herbs with stone mortar and pestle, a drink seller, an
herbalist, and masseuse treating people. The Madhawapura inscription from
Majapahit period mentioned a specific profession of herbs mixer and
combiner (herbalist), called Acaraki. The book from Mataram dated from circa
1700 contains 3,000 entries of jamu herbal recipes, while Javanese classical
literature Serat Centhini (1814) describes some jamu herbal concoction recipes.
Though possibly influenced
by Indian Ayurveda systems, the Indonesia archipelago holds numerous indigenous
plants not found in India, including plants similar to those in Australia
beyond the Wallace Line. Jamu practices may vary from region to region, and are
often not recorded, especially in remote areas of the country. Although
primarily herbal, some Jamu materials are acquired from animals, such as honey,
royal jelly, milk and Ayam Kampung eggs.
BELIEFS
Herbalists tend to use extracts
from parts of plants, such as the roots or leaves, believing that plants are
subject to environmental pressures and therefore develop resistance to threats
such as radiation, reactive oxygen species and microbial attack to survive,
providing defensive phytochemicals of use in herbalism.
USE OF PLANTS BY ANIMALS
Indigenous healers often claim to
have learned by observing that sick animals change their food preferences to
nibble at bitter herbs they would normally reject. Field biologists have
provided corroborating evidence based on observation of diverse species, such as
chickens, sheep, butterflies, and chimpanzees. The habit of changing diet
has been shown to be a physical means of purging intestinal parasites. Sick
animals tend to forage plants rich in secondary metabolites, such as tannins
and alkaloids.
2.4
MEDICINAL PLANTS����������������������������������������������������������������������������������������������������������������
(back to content)
Medicinal plants, also called
medicinal herbs, have been discovered and used in traditional medicine
practices since prehistoric times. Plants synthesize hundreds of chemical
compounds for functions including defense against insects, fungi, diseases, and
herbivorous mammals. Numerous phytochemicals with potential or established
biological activity have been identified. However, since a single plant
contains widely diverse phytochemicals, the effects of using a whole plant as
medicine are uncertain. Further, the phytochemical content and pharmacological
actions, if any, of many plants having medicinal potential remain unassessed by
rigorous scientific research to define efficacy and safety.
�
The bark of willow trees contains salicylic acid, the active
metabolite of aspirin, and has been used for millennia to relieve pain and
reduce fever.
�
Medicinal plants
The earliest historical records
of herbs are found from the Sumerian civilization, where hundreds of medicinal
plants including opium are listed on clay tablets, c. 3000 BC. The Ebers
Papyrus from ancient Egypt, c. 1550 BC, describes over 850 plant medicines. The
Greek physician Dioscorides, who worked in the Roman army, documented over 1000
recipes for medicines using over 600 medicinal plants in De materia medica, c.
60 AD; this formed the basis of pharmacopoeias for some 1500 years. Drug
research sometimes makes use of ethnobotany to search for pharmacologically
active substances, and this approach has yielded hundreds of useful compounds.
These include the common drugs aspirin, digoxin, quinine, and opium. The
compounds found in plants are of many kinds, but most are in four major
biochemical classes: alkaloids, glycosides, polyphenols, and terpenes.
Medicinal plants are widely used
in non-industrialized societies, mainly because they are readily available and
cheaper than modern medicines. The annual global export value of the thousands
of types of plants with medicinal properties was estimated to be US$2.2 billion
in 2012.� In 2017, the potential global
market for botanical extracts and medicines was estimated at several hundred
billion dollars. In many countries, there is little regulation of traditional
medicine, but the World Health Organization coordinates a network to encourage
safe and rational usage. Medicinal plants face both general threats, such as
climate change and habitat destruction, and the specific threat of
over-collection to meet market demand.
HISTORY
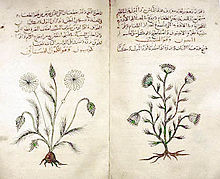
Dioscorides's 1st century De materia medica, seen here in a
c. 1334 copy in Arabic, describes some 1000 drug recipes based on over 600
plants.
PREHISTORIC TIMES
Plants, including many now used
as culinary herbs and spices, have been used as medicines, not necessarily
effectively, from prehistoric times. Spices have been used partly to counter
food spoilage bacteria, especially in hot climates, and especially in meat
dishes which spoil more readily. Angiosperms (flowering plants) were the
original source of most plant medicines.
Human settlements are often surrounded
by weeds used as herbal medicines, such as nettle, dandelion and chickweed.
Humans were not alone in using herbs as medicines: some animals such as
non-human primates, monarch butterflies and sheep ingest medicinal plants
when they are ill. Plant samples from prehistoric burial sites are among the
lines of evidence that Paleolithic peoples had knowledge of herbal medicine.
For instance, a 60,000-year-old Neanderthal burial site, "Shanidar
IV", in northern Iraq has yielded large amounts of pollen from eight plant
species, seven of which are used now as herbal remedies. Also, a mushroom was
found in the personal effects of �tzi the Iceman, whose body was frozen in the
�tztal Alps for more than 5,000 years. The mushroom was probably used against
whipworm.
ANCIENT TIMES
The Ebers Papyrus (c. 1550 BC) from Ancient Egypt describes
the use of hundreds of plant medicines.
In ancient Sumeria, hundreds of medicinal plants including
myrrh and opium are listed on clay tablets from around 3000 BC. The ancient
Egyptian Ebers Papyrus lists over 800 plant medicines such as aloe, cannabis,
castor bean, garlic, juniper, and mandrake.
From ancient times to the
present, Ayurvedic medicine as documented in the Atharva Veda, the Rig Veda and
the Sushruta Samhita has used hundreds of pharmacologically active herbs and
spices such as turmeric, which contains curcumin. The Chinese pharmacopoeia,
the Shennong Ben Cao Jing records plant medicines such as chaulmoogra for
leprosy, ephedra, and hemp. This was expanded in the Tang Dynasty Yaoxing Lun.
In the fourth century BC, Aristotle's pupil Theophrastus wrote the first
systematic botany text, Historia plantarum. In around 60 AD, the Greek
physician Pedanius Dioscorides, working for the Roman army, documented over
1000 recipes for medicines using over 600 medicinal plants in De materia
medica. The book remained the authoritative reference on herbalism for over
1500 years, into the seventeenth century.
MIDDLE AGES
Illustration of a 1632 copy of Avicenna's 1025 The Canon of
Medicine, showing a physician talking to a female patient in a garden, while
servants prepare medicines.
In the Early Middle Ages,
Benedictine monasteries preserved medical knowledge in Europe, translating and
copying classical texts and maintaining herb gardens. Hildegard of Bingen wrote
Causae et Curae ("Causes and Cures") on medicine. In the Islamic
Golden Age, scholars translated many classical Greek texts including
Dioscorides into Arabic, adding their own commentaries. Herbalism
flourished in the Islamic world, particularly in Baghdad and in Al-
Andalus.� Among many works on medicinal
plants, Abulcasis (936�1013) of Cordoba wrote The Book of Simples, and Ibn
al-Baitar (1197�1248) recorded hundreds of medicinal herbs such as Aconitum,
nux vomica, and tamarind in his Corpus of Simples. Avicenna included many
plants in his 1025 The Canon of Medicine. Abu-Rayhan Biruni, Ibn Zuhr, Peter of
Spain, and John of St Amand wrote further pharmacopoeias.
EARLY MODERN
An early illustrated book of medicinal plants, The Grete
Herball, 1526
The Early Modern period saw the
flourishing of illustrated herbals across Europe, starting with the 1526
Grete Herball. John Gerard wrote his famous The Herball or General History of
Plants in 1597, based on Rembert Dodoens, and Nicholas Culpeper published his
The English Physician Enlarged. Many new plant medicines arrived in Europe as
products of Early Modern exploration and the resulting Columbian Exchange, in
which livestock, crops and technologies were transferred between the Old World
and the Americas in the 15th and 16th centuries. Medicinal herbs arriving in
the Americas included garlic, ginger, and turmeric; coffee, tobacco and coca
travelled in the other direction. In Mexico, the sixteenth century Badianus
Manuscript described medicinal plants available in Central America.
19TH AND 20TH CENTURIES
The place of plants in medicine
was radically altered in the 19th century by the application of chemical
analysis. Alkaloids were isolated from a succession of medicinal plants, starting
with morphine from the poppy in 1806, and soon followed by ipecacuanha and
strychnos in 1817, quinine from the cinchona tree, and then many others. As
chemistry progressed, additional classes of pharmacologically active substances
were discovered in medicinal plants. Commercial extraction of purified
alkaloids including morphine from medicinal plants began at Merck in 1826.
Synthesis of a substance first discovered in a medicinal plant began with
salicylic acid in 1853. Around the end of the 19th century, the mood of
pharmacy turned against medicinal plants, as enzymes often modified the
active ingredients when whole plants were dried, and alkaloids and glycosides
purified from plant material started to be preferred. Drug discovery from
plants continued to be important through the 20th century and into the 21st, with
important anti-cancer drugs from yew and Madagascar periwinkle.
CONTEXT
Medicinal plants are used with
the intention of maintaining health, to be administered for a specific
condition, or both, whether in modern medicine or in traditional medicine. The
Food and Agriculture Organization estimated in 2002 that over 50,000 medicinal
plants are used across the world. The Royal Botanic Gardens, Kew more
conservatively estimated in 2016 that 17,810 plant species have a medicinal
use, out of some 30,000 plants for which a use of any kind is documented.
In modern medicine, around a
quarter[a] of the drugs prescribed to patients are derived from medicinal
plants, and they are rigorously tested. In other systems of medicine, medicinal
plants may constitute the majority of what are often informal attempted
treatments, not tested scientifically. The World Health Organization
estimates, without reliable data, that some 80 percent of the world's
population depends mainly on traditional medicine (including but not limited to
plants); perhaps some two billion people are largely reliant on medicinal
plants. The use of plant-based materials including herbal or natural health
products with supposed health benefits, is increasing in developed
countries. This brings attendant risks of toxicity and other effects on human
health, despite the safe image of herbal remedies. Herbal medicines have been
in use since long before modern medicine existed; there was and often still is
little or no knowledge of the pharmacological basis of their actions, if any,
or of their safety. The World Health Organization formulated a policy on
traditional medicine in 1991, and since then has published guidelines for them,
with a series of monographs on widely used herbal medicines.
Medicinal plants may provide three main kinds of
benefit:� health benefits to
the people who consume them as medicines; financial benefits to
people who harvest, process, and distribute them for sale; and society-wide
benefits, such as job opportunities, taxation income, and a healthier
labour force. However, development of plants or extracts having potential
medicinal uses is blunted by weak scientific evidence, poor practices in
the process of drug development, and insufficient financing.
PHYTOCHEMICAL BASIS
All plants produce chemical
compounds which give them an evolutionary advantage, such as defending against
herbivores or, in the example of salicylic acid, as a hormone in plant defenses.
These phytochemicals have potential for use as drugs, and the content and known
pharmacological activity of these substances in medicinal plants is the
scientific basis for their use in modern medicine, if
scientifically confirmed. For instance, daffodils (Narcissus)
contain nine groups of alkaloids including galantamine, licensed for use against
Alzheimer's disease. The alkaloids are bitter-tasting and toxic, and
concentrated in the parts of the plant such as the stem most likely to be eaten
by herbivores; they may also protect against parasites.
Modern knowledge of medicinal
plants is being systematised in the Medicinal Plant Transcriptomics Database,
which by 2011 provided a sequence reference for the transcriptome of some
thirty species. The major classes of pharmacologically active phytochemicals
are described below, with examples of medicinal plants that contain them.
ALKALOIDS
Alkaloids are bitter-tasting
chemicals, very widespread in nature, and often toxic, found in many medicinal
plants. There are several classes with different modes of action as drugs, both
recreational and pharmaceutical. Medicines of different classes include atropine,
scopolamine, and hyoscyamine (all from nightshade), the traditional medicine
berberine (from plants such as Berberis and Mahonia), [b] caffeine (Coffea),
cocaine (Coca), ephedrine (Ephedra), morphine (opium poppy), nicotine
(tobacco), [c] reserpine (Rauvolfia serpentina),� quinidine�
and quinine (Cinchona), vincamine (Vinca minor), and vincristine
(Catharanthus roseus).
|

The opium poppy Papaver somniferum is the source of the alkaloids
morphine and codeine.
|
|
The alkaloid nicotine from tobacco binds directly to the body's
Nicotinic acetylcholine receptors, accounting for its pharmacological
effects.
|
|

Deadly nightshade, Atropa belladonna, yields tropane alkaloids
including atropine, scopolamine and hyoscyamine.
|
GLYCOSIDES
Anthraquinone glycosides are
found in medicinal plants such as rhubarb, cascara, and Alexandrian senna.
Plant-based laxatives made from such plants include senna, rhubarb and Aloe.
The cardiac glycosides are
powerful drugs from medicinal plants including foxglove and lily of the valley.
They include digoxin and digitoxin which support the beating of the heart, and
act as diuretics.
|
Senna alexandrina, containing anthraquinone glycosides, has been used
as a laxative for millennia.

|
|

The foxglove, Digitalis purpurea, contains digoxin, a cardiac
glycoside. The plant was used on heart conditions long before the glycoside
was identified.
|
|
Digoxin is used to treat atrial fibrillation, atrial
flutter and sometimes heart failure.
|
POLYPHENOLS
Polyphenols of several classes
are widespread in plants, having diverse roles in defenses against plant
diseases and predators. They include hormone-mimicking phytoestrogens and
astringent tannins. Plants containing phytoestrogens have been administered for
centuries for gynecological disorders, such as fertility, menstrual, and
menopausal problems. Among these plants are Pueraria mirifica, kudzu,
angelica,] fennel, and anise.
Many polyphenolic extracts, such
as from grape seeds, olives or maritime pine bark, are sold as dietary
supplements and cosmetics without proof or legal health claims for
beneficial health effects. In Ayurveda, the astringent rind of the
pomegranate, containing polyphenols called punicalagins, is used as a medicine.
|

Angelica, containing phytoestrogens, has long been used for
gynaecological disorders.
|
|
Polyphenols include phytoestrogens (top and middle), mimics of animal
estrogen (bottom).
|
TERPENES
Terpenes and terpenoids of many
kinds are found in a variety of medicinal plants, and in resinous plants such as
the conifers. They are strongly aromatic and serve to repel herbivores. Their
scent makes them useful in essential oils, whether for perfumes such as rose
and lavender, or for aromatherapy. Some have medicinal uses: for example,
thymol is an antiseptic and was once used as a vermifuge (anti-worm medicine).
|

The essential oil of common thyme (Thymus vulgaris), contains the
monoterpene thymol, an antiseptic and antifungal.
|
|
Thymol is one of many terpenes found in plants.

|
|
In practice
Licensed commercial cultivation of opium poppies, Tasmania, 2010

|
CULTIVATION
Medicinal plants demand intensive
management. Different species each require their own distinct conditions of
cultivation. The World Health Organization recommends the use of rotation to
minimise problems with pests and plant diseases. Cultivation may be traditional
or may make use of conservation agriculture practices to maintain organic
matter in the soil and to conserve water, for example with no-till farming
systems. In many medicinal and aromatic plants, plant characteristics vary
widely with soil type and cropping strategy, so care is required to obtain satisfactory
yields.
PREPARATION
�
A Medieval physician preparing an extract from a medicinal
plant, from an Arabic Dioscorides, 1224
Medicinal plants are often tough and
fibrous, requiring some form of preparation to make them convenient to
administer. According to the Institute for Traditional Medicine, common methods
for the preparation of herbal medicines include decoction, powdering, and
extraction with alcohol, in each case yielding a mixture of substances.
Decoction involves crushing and then boiling the plant material in water to
produce a liquid extract that can be taken orally or applied topically.� Powdering involves drying the plant material
and then crushing it to yield a powder that can be compressed into tablets.
Alcohol extraction involves soaking the plant material in cold wine or distilled
spirit to form a tincture.
Traditional poultices were made
by boiling medicinal plants, wrapping them in a cloth, and applying the
resulting parcel externally to the affected part of the body.
When modern medicine has identified
a drug in a medicinal plant, commercial quantities of the drug may either be
synthesised or extracted from plant material, yielding a pure chemical.
Extraction can be practical when the compound in question is complex.
USAGE
�
A herbalist's shop in the souk of Marrakesh, Morocco
Plant medicines are in wide use
around the world. In most of the developing world, especially in rural areas,
local traditional medicine, including herbalism, is the only source of health
care for people, while in the developed world, alternative medicine including
use of dietary supplements is marketed aggressively using the claims of
traditional medicine. As of 2015, most products made from medicinal plants had
not been tested for their safety and efficacy, and products that were marketed
in developed economies and provided in the undeveloped world by traditional
healers were of uneven quality, sometimes containing dangerous contaminants.
Traditional Chinese medicine makes use of a wide variety of plants, among other
materials and techniques. Researchers from Kew Gardens found 104 species used
for diabetes in Central America, of which seven had been identified in at
least three separate studies. The Yanomami of the Brazilian Amazon, assisted by
researchers, have described 101 plant species used for traditional medicines.
Drugs derived from plants
including opiates, cocaine and cannabis have both medical and recreational
uses. Different countries have at various times made use of illegal drugs,
partly on the basis of the risks involved in taking psychoactive drugs.
EFFECTIVENESS
The bark of the cinchona tree contains the alkaloid quinine,
traditionally given for malaria.
Plant medicines have often not
been tested systematically, but have come into use informally over the
centuries. By 2007, clinical trials had demonstrated potentially useful
activity in nearly 16% of herbal medicines; there was limited in vitro or in
vivo evidence for roughly half the medicines; there was only phytochemical
evidence for around 20%; 0.5% were allergenic or toxic; and some 12% had
basically never been studied scientifically. Cancer Research UK caution
that there is no reliable evidence for the effectiveness of herbal remedies for
cancer.
A 2012 phylogenetic study built a
family tree down to genus level using 20,000 species to compare the medicinal
plants of three regions, Nepal, New Zealand and the Cape of South Africa. It
discovered that the species used traditionally to treat the same types of
condition belonged to the same groups of plants in all three regions, giving a
"strong phylogenetic signal".�
Since many plants that yield pharmaceutical drugs belong to just these
groups, and the groups were independently used in three different world regions,
the results were taken to mean
1) that these plant groups do
have potential for medicinal efficacy,
2) that undefined
pharmacological activity is associated with use in traditional medicine, and 3)
that the use of a phylogenetic groups for medicines in one region may predict their
use in the other regions.
REGULATION
The practice of Ayurveda in India, such as the running of
this Ayurvedic pharmacy in Rishikesh, is regulated by a government department,
AYUSH.
The World Health Organization
(WHO) has been coordinating a network called the International Regulatory Cooperation
for Herbal Medicines to try to improve the quality of medical products made
from medicinal plants and the claims made for them. In 2015, only around 20% of
countries had well-functioning regulatory agencies, while 30% had none, and
around half had limited regulatory capacity. In India, where Ayurveda has been practised
for centuries, herbal remedies are the responsibility of a government
department, AYUSH, under the Ministry of Health & Family Welfare.
WHO has set out a strategy for
traditional medicines with four objectives: to integrate them as policy into
national healthcare systems; to provide knowledge and guidance on their safety,
efficacy, and quality; to increase their availability and affordability; and to
promote their rational, therapeutically sound usage. WHO notes in the strategy
that countries are experiencing seven challenges to such implementation, namely
in developing and enforcing policy; in integration; in safety and quality,
especially in assessment of products and qualification of practitioners;
in controlling advertising; in research and development; in education and
training; and in the sharing of information.
DRUG DISCOVERY
The anticancer drug taxol was developed after screening of
the Pacific yew, Taxus brevifolia (foliage and fruit shown) in 1971.
�
The pharmaceutical industry has
roots in the apothecary shops of Europe in the 1800s, where pharmacists
provided local traditional medicines to customers, which included extracts like
morphine, quinine, and strychnine. Therapeutically important drugs like
camptothecin (from Camptotheca acuminata, used in traditional Chinese medicine)
and taxol (from the Pacific yew, Taxus brevifolia) were derived from
medicinal plants. The Vinca alkaloids vincristine and vinblastine, used as
anti-cancer drugs, were discovered in the 1950s from the Madagascar periwinkle,
Catharanthus roseus.
Hundreds of compounds have been
identified using ethnobotany, investigating plants used by indigenous
peoples for possible medical applications. Some important phytochemicals,
including curcumin, epigallocatechin gallate, genistein and resveratrol are
pan-assay interference compounds, meaning that in vitro studies of their
activity often provide unreliable data. As a result, phytochemicals have
frequently proven unsuitable as the lead substances in drug discovery. In the
United States over the period 1999 to 2012, despite several hundred
applications for new drug status, only two botanical drug candidates had
sufficient evidence of medicinal value to be approved by the Food and Drug
Administration.
The pharmaceutical industry has remained
interested in mining traditional uses of medicinal plants in its drug discovery
efforts. Of the 1073 small-molecule drugs approved in the period 1981 to 2010,
over half were either directly derived from or inspired by natural substances.
Among cancer treatments, of 185 small-molecule drugs approved in the period
from 1981 to 2019, 65% were derived from or inspired by natural substances.
SAFETY
The Thornapple Datura stramonium has been used for asthma,
because it contains the alkaloid atropine, but it is also a powerful and
potentially fatal hallucinogen.
Plant medicines can cause adverse
effects and even death, whether by side-effects of their active substances, by
adulteration or contamination, by overdose, or by inappropriate prescription.
Many such effects are known, while others remain to be explored
scientifically. There is no reason to presume that because a product
comes from nature it must be safe:� the
existence of powerful natural poisons like atropine and nicotine shows this to
be untrue. Further, the high standards applied to conventional medicines do not
always apply to plant medicines, and dose can vary widely depending on the
growth conditions of plants: older plants may be much more toxic than young
ones, for instance.
Pharmacologically active plant
extracts can interact with conventional drugs, both because they may provide an
increased dose of similar compounds, and because some phytochemicals interfere
with the body's systems that metabolise drugs in the liver including the
cytochrome P450 system, making the drugs last longer in the body and have a more
powerful cumulative effect. Plant medicines can be dangerous during pregnancy.
Since plants may contain many different substances, plant extracts may have
complex effects on the human body.
QUALITY, ADVERTISING, AND LABELLING
Herbal medicine and dietary
supplement products have been criticized as not having sufficient standards or
scientific evidence to confirm their contents, safety, and presumed
efficacy. A 2013 study found that one-third of herbal products sampled
contained no trace of the herb listed on the label, and other products were
adulterated with unlisted fillers including potential allergens.
THREATS
Where medicinal plants are harvested
from the wild rather than cultivated, they are subject to both general and
specific threats. General threats include climate change and habitat loss
to development and agriculture. A specific threat is over-collection to
meet rising demand for medicines. A case in point was the pressure on wild
populations of the Pacific yew soon after news of taxol's effectiveness
became public. �The threat from
over-collection could be addressed by cultivation of some medicinal plants, or
by a system of certification to make wild harvesting sustainable. A
report in 2020 by the Royal Botanic Gardens, Kew identifies 723 medicinal
plants as being at risk of extinction, caused partly by over-collection.
(back
to content)
2.5 Origin of Traditional Medicine n
The origin and history of
traditional medicine in Health Care Delivery as far as humanity is concerned is
as old as the history of man himself. The Book of Beginnings recorded God as
the manufacturer and originator of herbal medicine. And God Said, let the earth
bring forth grass, the herb yielding seed, and the fruit tree yielding fruit
after his kind, whose seed is in itself, upon the earth and it was so. And the
earth brought forth grass, and herb yielding seed after his kind and the tree
yield fruit, whose seed was in itself after his kind and God saw that it was
good. (Genesis 1:10-11)
Before the creation of man, the
Holy Book recorded that the Creator did not permit rain to fall upon the earth
because there has not been created the man that will utilize the herbs that the
earth will produce. After creating man, God made him the Estate Manager and
Caretaker of after planting a botanical Garden in Eden. He told man that some
of the fruits and herbs are good for food while others can be poisonous and are
capable of causing death (Gen 2:5.7.8.9.15,16,17).
Attesting to the above assertion,
Ekeopara in his book, African Traditional Religion, An Introduction, averred:
It is quite probable that man as soon as he has reached the stage of reasoning
found out through trial and error that plants can be used as food, that some
might be poisonous and may even lead to death when eaten while some had
medicinal value and power. The entire essence of traditional medicine revolves
around the use of natural herbs in the bodily, spiritual, emotional and
psychological healing of the total man. God is the source of nature and the
manufacturer of the herbs. Therefore, God is the source of traditional or
herbal medicine. King David in Psalm 104:14 stated thus: �He causes the grass
to grow for the cattle and herbs for the service of man.
Onunwa, observed that healing is
a part of the whole complex religious attempt by man to bring the physical and
spiritual aspects of the universe as well as man who lives in it into the
desired consistent harmony. The idea of �wholeness� is therefore not alien to
the African mind. Healing becomes a cardinal religious practice because African
cosmology demands that life in the world must be kept free from problem
especially ill-health and obstacles that may hinder the fulfilment of desired
goals. In the traditional African world view, health and healing are connected
just in the same way they are with the fundamental theme of life. Herbs were
the first medicines used by pre historic man. They are, therefore, part of
every cultural tradition and have helped the development and growth of herbal
medicine in Nigeria.
Still on the history of
traditional medicine, Ekeopara noted that: Before the advent of western
medicine our fore-bearers depended largely on traditional medicine and healing
methods for the treatment of ailments and the cure of various types of
diseases.
Mhame states that: Since the
early 1970, the World Health Organization (WHO) has reportedly advocated for
the recognition of Traditional Health Practitioners (THPs) as Primary Health
Care Provider and for the integration of traditional medicine into the National
Health System. Several calls have been made on Federal Government of Nigeria to
take responsibility for the health of their people and to formulate national
policies, regulations and standard, as part of comprehensive national health
programs to ensure appropriate, safe and effective use of traditional medicine.
Traditional medicine and its
practitioners were officially recognized by the Alma Ata declaration in 1978 as
an important resource for achieving the targeted goal of rendering good health
care services for all by the year 2000. Since then, member States and the World
Health Organization governing bodies have adopted a number of resolutions and
declaration on traditional medicine. Notable among the resolutions are on
�Promoting the Role of Traditional Medicine in Health Systems: A Strategy for
the African Region�. This resolution v as adopted by WHO Regional Committee for
Africa in Ouagadougou, Burkina Faso, on August 31. 2000 and the declaration of
the Decade of African Traditional Medicine (2000-20 10) by the Heads of State
and Government in Lusaka, Zambia in July 2001. It was also resolved that a day
be observed annually as African Traditional Medicine Day all over Africa and
other parts of the world including Nigeria. That day is 31st day of August. The
year 2010 marked a Decade since the institution of African Traditional Medicine
Day. African Traditional Medicine Day was commemorated in 2003 in South Africa
in conjunction with the 53 session of WHO Regional Committee for �African
Traditional Medicine, our Culture, and Our Future� which Nigeria also attended.
This singular act has created enabling environment for training and
collaboration between practitioners of traditional medicine and conventional
medicine for networking and information exchange.
TYPES OF TRADITIONAL HEALERS
The traditional healer, as
defined by the WHO (1976), is a person who is recognized by the community in
which he lives as competent to provide health care by using vegetable, animal
and mineral substances and certain other methods based on the social, cultural
and religious background, as well as on the knowledge, attributes and beliefs
that are prevalent in the community, regarding physical, mental and social
well-being and the causation of disease and disability the following are the
different types of healers in traditional African society:
� Traditional Herbalists:
Herbalists use mainly herbs, that is, medicinal plants or parts of such
plants-whole root, stem, leaves, stem bark or root bark, flowers, fruits,
seeds, but sometimes animal parts, small whole animal � snails, snakes,
chameleons, tortoises, lizards, etc: inorganic residues -alum, camphor, salt,
etc and insects, bees, black ants etc. is such herbal preparations may be
offered in the form of (i) powder, which could be swallowed or taken with pap
(cold or hot) or any drink, (ii) powder, rubbed into cuts or incisions made on
an part of the body with a sharp knife, (iii) preparation, soaked for some time
in water or local gin, decanted as required before drinking; the materials
could also be boiled- in water, cooled and strained (iv) preparation pounded
with native soap and used for bathing; such �medicated soaps� are commonly used
for skin diseases, (v) pastes, pomades or ointments, in a medium of palm oil or
shea butter, or (vi) soup which is consumed by the patient. The herbalist cures
mainly with plants which he gathers fresh. When seasonal plants have to be
used, these plants are collected when available and are preserved usually by
drying to eliminate moisture.
� Traditional Birth Attendants
(TBAs): The World Health Organization defines a traditional birth attendant
(TBA) as a person who assists the mother at childbirth and who initially
acquired her skills delivering babies by herself or by working with other birth
attendants. In the northern parts of the country, TBAs are of the female sex
only, whereas in some other parts both males and females are involved. TBAs
occupy a prominent position in Nigeria today as between 60-8 5 per cent of
births delivered in the country and especially in the rural communities are by
the TBAs.
They know how to diagnose
pregnancy, confirm it and determine the position of the growing foetus. They
have been seen to provide pre-natal and postnatal care and so combine
successfully the duties of the modern-day mid-wife. Highly experienced TBAs
have been recognized to assist in obstetric and Paediatrics care, as they
manage simple maternal and hah hood illnesses. As a result of their exposure
and experience, and more particularly the TBA�s concept of human reproduction,
as exemplified by pregnancy and childbirth being normal biological functions of
human life linked holistically to cultural/social practices, TBAs have been
trained to assist in orthodox� medicine practices at the primary health care
level.
With their extra hands, a greater
coverage of primary health care leading to improved maternal or child health
and the lowering of maternal and child mortality and morbidity, have been
achieved. TBAs are usually old and experienced women who see their assignments
primarily as contributing their skill for the good of the community. With
experienced TBAs, child delivery by Caesarean section is not common since it is
hardly necessary to seek surgical help during child birth.
3. Traditional Surgeons: The
various forms of surgery recognised in traditional medical care include: (i)
the cutting of tribal marks: traditional surgeons usually cut tribal marks into
the cheeks, bellies, etc. and charred herbal products are usually rubbed into
these bleeding marks to effect healing, (ii) male and female circumcision
(Clitoridectomy): traditional surgeons carry out these simple surgical
operations with special knives and scissors: blood-letting operations and
wounds that result from these operations are usually treated with snail body
fluid or pastes prepared from plants.
These practices are, however,
fast dying out in urban areas; (iii) removal of whitlow: diseased toes or
fingers are usually cut open and treated. Piercing of ear lobes: particularly
in the youth to allow the fixing of ear rings. Extraction of tooth: infected
teeth or teeth with holes, that bring pain to the mouth are removed and treated
with herbal medicines prepared in local gin.
4. Traditional Medicinal
Ingredient Dealers: These dealers, more often women, are involved in buying and
selling of plants, animals and insects, and minerals used in making herbal
preparations. Some of them, who indulge in preparing herbal concoctions or
decoctions for the management or cure of febrile conditions in children or some
other diseases of women and children, may qualify to be referred to as
traditional healers.
5. Traditional Psychiatrists: The
traditional psychiatrist specializes mainly in the treatment of lunatics and
those with mental disorders. Lunatics are usually restrained from going violent
by chaining them with iron or by clamping them down with wooden shackles.
People w ith mental disorders who are violent, particularly those that are
demon possessed, are usually called or beaten to submission and then given
herbal hypnotics or highly sedative herbal potions to calm them, in order to
bring them to a state of mental, emotional and psychological calmness as well
as tranquility. Treatment and rehabilitation of people with mental disorders
usually take long periods.
Unlike the bone setter, the
traditional psychiatrist and the traditional birth attendant whose duties are
well defined and specialized, the herbalist is the general practitioner in
traditional medicine. He is expected to be knowledgeable in all the various
aspects of healing and in the functioning of the various organs of the body.
Much is expected of him, as by his wealth of experience and knowledge he is
expected to determine the nature of the patient�s illness, treat him and also
predict the course of his treatment. In a typical traditional setting, he combines
the role of the present day doctor with that of the pharmacist and the nurse.
6. Practitioners of Therapeutic
Spiritism: These practitioners include diviners or fortune tellers, who may be
seers, alfas and priests, and use supernatural or mysterious forces,
incantations, may prescribe rituals associated with the community�s religious
worship and adopt all sorts of inexplicable things to treat various diseases.
The practitioners are usually consulted for diagnosis of diseases, their causes
and treatment. With their ability to deal with the unseen, and the
supernatural, they are usually held in high esteem in the community. They are
believed to have extra-sensory perception and can see beyond the ordinary man.
They can receive telepathic messages, can consult oracles, spirit guides etc.
and perform well where other traditional healers and orthodox doctors fail.
Their activities include, making prayers, citing and singing of incantations, making
invocations and preparing sacrificial materials to appease unknown gods. It is
believed that diseases which are caused by supernatural forces will be readily
diagnosed and treated by these practitioners. This, in itself stems from the
belief that certain medical ingredients � unusually large trees that are
believed to house spirits, astronomic herbs, grave-yard plants like the physic
nut, protective plants such as the wild colocynth or Sodom apple or even some
reproductive herbs like the sausage tree or the tree of life itself� have
spiritual powers and can be effectively utilized by these practitioners for the
good of all.
The instructions which these
practitioners use include magic stones which are usually thrown to the ground.
Sounds so produced are read and interpreted. Some take replies of messages in a
pool or glass of water. Others depend on the throwing of cowries, coins,
kola-nut seeds, divining rods, keys or sticks, etc. Divination has come of age,
its various functions linked with religion, creation myths, cosmology et
cetera.
REASONS FOR GROWING PATRONAGE FOR TRADITIONAL MEDICINE
Health is the most precious of
all things and it is the foundation of all happiness. Traditional medicine has
developed in various communities in Nigeria in response to the health needs of
the people. Many communities have since creation, developed various traditional
systems using locally- available resources for the alleviation of their health
pob1em. As once noted some 13 years ago, traditional medicine is as old as the
hills in Nigeria. The development of traditional medicine in Nigeria has led to
the emergence of various categories of healers, the various healing methods,
strategies and medicines or remedies now known. The British colonial masters
brought in orthodox medicine and, today, both systems of medicine exist in the
country; both have the primary objective to cure, manage or prevent diseases
and maintain good health.
It is important to stress the
relevance of traditional medicine to the majority of Nigerians. Most Nigerians,
especially those living in rural communities don�t have access to orthodox
medicine and it is estimated that about 75 per cent of the populace still
prefer to solve their health problems consulting traditional healers. Where
such access exists, the rising cost of imported medications and other
commodities used for medicines have posed a big problem. Besides, many rural
communities have great faith in traditional medicine, particularly the
inexplicable aspects as they believe that it is the wisdom of their
fore-fathers which also recognizes their socio-cultural and religious
background, which orthodox medicine seems to neglect. Recent reports show that
more people in the world embrace traditional medicine.
To Ann Angbazo, several people have
somewhat lost confidence in the efficacy of orthodox medicine. Analysts
attribute the people�s loss of confidence in orthodox medicine to factors such
as drug counterfeiting and drug reactions, as well as the affordability and
accessibility of the traditional healthcare delivery. They also observe that
traditional medicine has been used to cure various life-threatening ailments in
all parts of the world at lower costs, e en before the discovery of some
medications. The general acceptance of traditional medicine is even attested to
by the World Health Organization (WHO).
SOME DISEASES AND THEIR TRADITIONAL HERBAL CURES
There is abundant justification for the use of herbs by the
various traditional healers identified. Disease conditions identified in traditional
medicine include:
(1) Cardiovascular disease
hypertension, stroke etc. for which the antihypertensive herbs. the African
Rauwolfia and the Negro coffee have been used to cure.
(2) Diseases of the nervous system-convulsions, insomnia
etc. for which the parrot�s beak and the African Rauwolfia also offer a good
remedy.
(3) Diseases of the alimentary system-diarrhoea, dysentery
etc. for which basil is useful.
(4) Diseases of the endocrine system-diabetes etc. for which
the leaves of the common roused periwinkle or mormodica are valuable.
(5) Diseases of the respiratory system - asthma, cough etc.
for which the lemon grass is of value.
(6) Diseases of the genital-urinary system, gonorrhoea,
haematuria, etc. for which the bush banana is useful.
(7) Diseases of the skin-wounds, dermatonycosis etc. for
which the craw-craw plant is very useful.
(8) Diseases associated with the ear, nose and throat ache,
sinusitis etc. for which the resurrection plant is usually recommended and
(9) Diseases caused by microbes, viruses, insects etc. -
infections, malaria etc. for which garlic, clove, the African mahogany etc.
have been found useful.
Numerous other diseases or
complaints of a special nature such as hernia, snake bite, atiliritis, gout
etc. have been treated using herbs alone or in admixture with animal parts and
minerals. Today, plant medicines include vincristine and vinblastine isolated
from the rose periinkle and used to treat childhood leukaemia and Hodgkin�s
disease, reserpine extracted from the African or Indian Rauwolfia and used in
tranquillisers, diogenin extracted from the am and used in the treatment of
rheumatism and to produce oral contraceptives and the shea butter hich showed
nasal decongestant activity etc.
Non-plant medicines include the
bee venom which is used in the treatment of arthritis and the cixet cat
exudates which have shown anticonvulsant effects. Plant extracts and chemicals
with muscle relaxant properties have been used by the TBAs to assist in child
deli\ cries. All these facts point to the values of medicinal plants and their
importance in traditional medicine in present day Nigeria.
(back
to content)
2.6 Contributions of Traditional Medicine
to Healthcare Development j
It is an incontrovertible fact
that traditional medicine has recorded meaningful and notable contributions
which cannot be dismissed with a wave of the hand in Health Care De1iery
Services not only in Nigeria alone but in many countries of Africa at large.
Busia noted that:
Globally there is now a general
recognition that traditional medicines, the medicines once described as
primitive could be mankind�s saving grace and therefore, within the past three
decades, the changing view of herbs in particular as traditional medicine has
moved from that of �witches brew� to major medicine.
It is estimated that out of a
global population of 6.3billon people in the world, about 4 billion people
patronize the use of plants to meet their primary health care needs. It is also
discovered that approximately about half the people living in urban cities in
various states of Nigeria regularly make use of what is regarded as
Complementary and Alternative Medicine. This increase in the demand and
availability of services for Complementary Medicine has outpaced the developmental
policy of the Federal Governments of Nigeria and the health sector.
� Remarkable Feats: In Nigeria,
traditional medicine has been the main source of health care for the vast
majority of people. It is currently estimated that between 70 and 80% -Africans
use traditional medicine for the management of both communicable and non
communicable diseases such as cancer, malaria, HIV/AIDS, diabetes, Hypertension
and tuberculosis. It is also noted that a high percentage of the rural populace
patronize traditional midwifery for their maternal and neonatal health
problems. Traditional Birth Attendants (TBA5) assists in majority of birth
delivery of pregnant women in most Nigerian villages and communities.
Other areas where traditional
medicine has contributed to the improvement of Health Care Delivery System
includes the recent HI V/AIDS menace where Dr. Abalaka, discovered curative
herbs for the dreaded disease which many patients have been reported treated on
private consultation. The disagreement he had with the Nigerian Medical
Association has hindered the wider scope of beneficiaries of his discovery.
Herbs are also used in quick healing of open injuries, stopping of bleeding,
miscarriages, toothache, extraction of bullets from gun shots, etcetera.
Primary Source of Modern
Medicine: Kasilo, notes that �traditional Medicine has demonstrated great
potential of therapeutic benefits in its contribution to modern medicine. An
estimate of more than 30% of modern medicine is directly or indirectly sourced
from traditional herbs such as analgesics (aspirin, Belladonna) anticancer
medicines (Vincristine and Vinbiastine) anti-malaria (quinine, artemisinin);
Anti-hypertensive agents (reserpine) and decongestants (ephedrine). As part of
the contributions of traditional medicine in Health Care Delivery System in
Nigeria, Ekeopara notes that:
...to make a barren woman
productive, a special concoction specially prepared to cleanse the reproductive
organs is administered to the woman three times daily for a period of three
days. Rituals might accompany such administrations if it is believed that there
is a spiritual agency involved in the barrenness.
This connotes that traditional
medicine has a lot to still contribute today in treating barrenness among
women.
Manpower Coverage: In most
Nigerian villages and communities, Traditional Health Practitioners (TI-IPs)
generally are far more in number than doctors. In Nigeria and our neighbouring
country, Ghana for example, statistics have shown that there are 25,000 and
10.000 patients for every medical doctor where as there are 200 and 100
patients respectively for C\ cry traditional Health practitioner. In view of
the acute shortage of medical doctors in the country, it becomes an
incontrovertible fact that Traditional Health Practitioners through traditional
medicines have contributed immensely to the raising of manpower for healthcare
coverage in Nigeria.
� Reduction of Child Mortality: A
study carried out by WHO showed that in Ghana, Mali and Nigeria the first line
of treatment for 60% of children with high fever resulting from malaria is the
use of herbal medicines. Going further in affirming the contributions of
Traditional Medicine in Health Care Delivery, Obinna, making an overview of
Traditional Medicine in Nigeria and other ECO WAS member States notes that at
the 2009 African traditional medicine Day held in Lagos, the Lagos State
Governor, Babatunde Fashola unequivocally opined that:
The pivotal role of traditional
medicine in health care delivery in Africa and its potential to contribute to
the attainment of the health-related provisions of the Millennium Development
Goals MDGS) stressing that the reduction of child mortality, improving of
maternal health and combating HIV/AIDS, malaria, tuberculosis, leprosies, child
malnutrition, among to how far we are able to harness the hidden potential of
our traditional medicine.
Commenting on the contributions
of traditional medicine in Health Care Delivery System in Nigeria; Ekeopara
commended:
�The Roman Catholic Church in
Nigeria whose monks in Delta State, Nigeria, are devoting a lot of energy in
research, in traditional medicine and healing. Their efforts have resulted in
the production of various types of traditional medicine that are being
patronized by many in Nigeria, for the cure of different ailments. These monks
have resolved to find a cure for the dreaded human decimator and killer �
HIV/AIDS. This effort should be encouraged and funded by the government and
donor agencies for the overall development of traditional medicine and healing
in Africa.
Onunwa, in his book Studies in
Igbo Traditional Religion averred that in recent times, most of the
practitioners of traditional healing have started to improve on their
techniques, which includes the use of modern clinic system and introduction of
some forms of new medication as an additional aid to the use of herbs and
roots. In some of the traditional healing homes, the liquids extracted from
leaves are stored in clean bottles, decently labeled and displayed on the
shelves for patients to see and buy. He went further to state that: A lot of
new things are happening in the traditional healing practices in recent times.
A recent breakthrough claimed by one middle aged native doctor from Mbano in
the South Igbo area is yet to be validated by modern research. The man, Dr.
Njoku Nwigwe, did not only claim to have discovered how African herbs and roots
could be used to cure stomach ulcers, pile and parasites in the human body
without patients undergoing any surgical operation but also claimed to have
made the discoveries known to the Chief Pharmacist in the Imo State Ministry of
Health Owerri, Nigeria. The ministry is yet to confirm the validity of this
claim.
If this is true it is a plus to traditional medicine.
DIFFERENT TRADITIONAL HEALTH CARE SERVICES
As part of its contribution to
the development of Health Care Delivery Systems in Nigeria, traditional
medicine has various Traditional Health Care Services through which it meets up
with the health needs and challenges of the people. Busia observes that, in
African traditional medicine, the curative, training, primitive and
rehabilitative services are referred to as clinical services. These traditional
health care services are provided through tradition and culture prescribed
under a particular philosophy. He went further to note that, the traditional
norms, taboos and culture which are the bedrock of clinical practice of
traditional medicine form the major reason for the acceptability of traditional
health practitioners in their various communities of service.
The philosophical clinical care
embedded in these guiding traditions, culture and taboos have contributed in no
small measure in making traditional medicine acceptable and highly demanded by
majority of the populace. These various health care services are:
Protective Services: A major part
of African Traditional Medicine is for protective and preventive healthcare
services. This guarantees spiritual and physical immunity from attack of
physical sickness or spiritual forces. To this end Gelfand avers that: Roots,
leaves or parts of animals or birds boiled in water or pulverized in fire from
the basic ingredients of (traditional) medicine..., represent the major forces
of nature. The vapour and smoke produced in boiling and pulverizing the
medicines symbolize the air. In applying them to the human body, the link
between nature and humanity is established in a very intense way and it
generates power to protect and heal. The linkage is also implied in the use of
charms and amulets which are medicines that protect.
This implies that traditional medicine has to do with nature
healing.
� Curative Services: Most of the
herbal medicines are also used to render curative ser ices for various ailments
afflicting humankind. This is quite pivotal to the impact of traditional
medicine in any given community.
� Destructive Services: There is
element of evil in every good. There is also element of poison in every food.
Traditional medicine even though it is used to render good services can as well
be used to achieve evil motives. �There are medicines for good fortune, love,
success, security of person and property... and there are also medicines
against sorcery and witchcraft�. However, Magesa adds that, �significantly, all
medicines contain all that ought to be used for the benefit of humanity, but
can also be put to detrimental use by immoral individuals�.
� General Health Services:
Kasilo, states that, general health services are services provided to clients
by non-specialized health care providers. The general traditional health
practitioner under general services can handle normal conditions like malaria,
stomach upset, respiratory problems, rheumatism, arthritis, sexual
dysfunctions, anemia and parasitic infections.
� Mental Health Services: Traditional
Medicine-men or Herbalists have proven to be very resourceful in rendering
effective services to people with mental cases. They most often make use of
divination to unravel the mental and psychological problems of their patients.
DR Ination plays a key role in the treatment of neurosis and helps in
re-tracing a patients� condition from its metaphysical past and influences its
interplay with the present and future.
� Midwifery Services: Midwifery
is a health care profession in which providers give prenatal care to expecting
mothers, attend to the birth of their infants and provide post-partum care to
the mother and her infant. Traditional Midwives are autonomous practitioners
who are specialists in a low-risk pregnancy, childbirth and the post-partum stage.
They help women to have healthy pregnancy and natural birth experience. They
are trained to handle delivery situations that are also out of the norms.
In the African traditional
setting, traditional midwives handle delivery cases intelligently. In the past
30 years, concerted efforts have been made in Nigeria to improve the ki1Is and
practices of traditional midwives, often referred to as Traditional Birth
Attendants (TBAs). For the traditional midwives to be able to provide optimal
care an enabling environment has to be provided and their collaboration with
Orthodox nurses and doctors in health services strengthened.
� Bone Setting Services: A bone
setter is a practitioner of joint manipulation. Before the advent of
Chiropractors, Osteopaths and physical therapist and even establishment of
orthopaedic hospitals, traditional bone setters were the main providers of this
type of treatment. Bone setters do reduce joint dislocations and re-set bone
fractures. Many traditional bone setters make use of splints, bandages,
plasters and clutches in the practice. They have been credited with success in
treating very bad cases which were initially mismanaged in some orthopaedic
hospitals. There are cases where orthopaedic surgeons had wanted to cut off a
broken limb but when the relatives of the patients transferred them to the
traditional bone setters, what was described as hopeless previously became
treated by the traditional healers without amputation. Some physiotherapists
have confessed that they on several occasions refer some cases to the
traditional bone setters.
� Training and Promotional
Services: The traditional medicine-men or herbalists engage themselves not only
in ministering healing to the sick but also in rendering training services to
young apprentices. Apprenticeship is a system or practice whereby training is
given to a new generation of intending practitioners in order for them to
acquire some skills to help in serving their communities. Training and
promotional aspects of African traditional medicine services help to inculcate
good characters in the practitioners which make them to be responsible.
Accommodating, hardworking, good listeners as well as develop confidence in
themselves, their traditions and cultural heritage.
� Rehabilitative Services:
Traditionally, there is no system of skills development for disabled or
physically challenged people in the Traditional African Community which would
lead to their public or self employment. Each family or community in the spirit
of �being your brother�s keeper rather than brother�s killer�, helps in the
rehabilitation of their own disabled persons. This social communal assistance
which is called �Ubuntu philosophy� gives the disabled a sense of belonging
creating an accommodating way of living through tradition, culture, norms and
taboos. Every disabled person therefore is accepted and recognized as part of
the family or community and is supported to lead a functional and fulfilled
life in spite of his apparent disability. With this kind of communal social
support every physically challenged person discovers ability in his disability.
This brings about mental, emotional and psychological healing to the physically
challenged person.
METHODS OF TRADITIONAL HEALING
There are various methodological
processes involved in the administration of traditional medicine in Nigeria
through which the goal of restoration of human health is achieved. They are
namely:
� Knowledge of Herbs: The major
method in the administration of traditional healing via local herbs is through
a good knowledge of herbs and roots and the right application of the same to
the patients who need them. Onunwa notes that treatment most times commences
with simple herbs and antidotes which may be administered for one day or two.
He further stated that the art of healing has been traditionally associated
with the thorough knowledge of the use of herbs and roots and the appropriate
rituals to perform at the appropriate time. Kasilo noted that the traditional
knowledge of herbs has played a significant role in the healthcare systems in
Nigeria and other countries of the African Region for centuries. Traditional
medicines are presently used by nearly 80% of the population. Owing to the
global resurgence in the use of natural products and the advent of the biotechnological
industry, traditional knowledge is increasingly becoming a source of modern
drug development and biotechnological inventions. Despite the important role of
traditional knowledge, traditional communities are unable to protect their
knowledge through the existing intellectual property system owing to the
failure of the knowledge to satisfy the requirements for intellectual property
protection. Parrinder, in his book West African Religion, observed that, �West
African doctors have a wide knowledge of the properties of many roots, barks,
leaves, and herbs. They are called �observers� of plants in Fon and workers in
roots in Furi�.
It is also noted that:
The traditional medicine men are not only knowledgeable in
the variety of roots and herbs that have therapeutic values, but also
understand the psychology of their people�s values. Their knowledge of the
healing powers in roots and leaves is amazing.
� Divination: When the condition
of the patient is not improved after the application of simple treatments, the
method of divination is applied whereby a diviner could be invited for
spiritual guidance as to ascertain the remote and esoteric cause of the
protracted ailment. The diviner may also recommend the type of medicine to be
applied for quick cure. Such recommendations may also involve rituals.
� Ritual Washing: Another method
of traditional healing is through ritual cleansing. This is carried out by the
traditional healer commonly called medicine-man on the patient. This is done
purposely to appease the deities and ancestors and restore a good and cordial
relationship between the patient and the deities so that their goodwill will
cause any medicine applied in making him to recover to be effective. To Onunwa,
the hospital is believed to be good for certain diseases whose treatment must
however, be validated by some ritual offerings at home. This is based on the
people�s world view. In spite of the contributions of modern medicine, some
traditional lgbo men still believe that healing is incomplete if some necessary
rituals are not performed. They do not completely despise the achievements of
Western medicine, but believe that there are some ailments which the hospitals
cannot cure.
iv. Diagnosis vaetiology: Common
ailments or problems are easily recognised and treated successfully, based on
the symptomatology of the disease. If the illness persists, recourse is made to
the practitioner of occultism/the diviner who� in his efforts to discover the
real cause of the disease, may consult various spirits including his oracle,
pre scribe appropriate rituals and make sacrifices to solicit the right answer.
This is because they believe that diseases can be caused by sorcery, ghosts,
breach of taboo, spirit intrusion and acts of the Supreme Being. It has also
been found that public opinion and rumours may help the diviner to trace the
cause of a disease. Diagnosis may also be achieved by visual, examination of
eyes, skin, urine, faeces etc.; taste, for example, of urine for sugar in the
diabetic, use of ants to detect sugar in the urine of the diabetic, palpation
that is through the sense of touch using palms, fingers or the analysis of a
patient�s dreams. Proper diagnosis is needed in the treatment of psychosomatic
and psychiatric cases just as in the eases of bone fractures and other
traumatic injuries. Generally, proper diagnosis is the key to most traditional
treatments.
v. Symptom Analysis: The patient
describes the symptoms as much as practicable. The healer also watches out for
these as well as analyses them and from the careful observations make his
prescriptions. For the various diseases, symptoms that are usually watched out
for include behavioural changes; fever or abnormal rise in body temperature;
jaundiced state, yellow colour in the eyes, urine, palm and fingers suggesting
possible 1ier problems; seizures as often experienced in convulsions, diarrhoea
in cases of poisoning; frequent stooling and vomiting; bleeding which may be
from the nose, mouth, gums, teeth, from private parts, anus; blood in the
urine; coughing and vomiting blood; breathing difficulty; sneezing; swelling
which may be minor and localised; general weakness of the body; and development
of rashes and even pain. Experienced herbalists can readily differentiate
constant or intermittent pains from sharp or dull ones and link them with
specific diseases. Signs: These are usually observed by experienced healers.
Modern-day healers are being encouraged to use stethoscopes and other simple
instruments to determine signs.
vi. Treatment: The herbalist
treats with medicines made up of plants, animals and minerals. He may also use
any of the therapeutic systems described earlier such as fasting and dieting
massage, therapeutic spiritism et cetera.
CHALLENGES FACING TRADITIONAL MEDICINE
There are myriads of serious
challenges militating against the progress and development of Traditional
Medical practice in Nigeria. Although a lot of progress has been made in
implementing the regional strategy on promoting the role of traditional
medicine in Health Care System, the Nigerian state has continued to face some
challenges that hamper the institutionalization of traditional medicine into
our National Health Care Systems. These challenges include:
� Poor Organizational Arrangement: There is limited
Organizational arrangement for the institutionalization of traditional medicine
such as:
� Poor allocation of financial resources for implementation
of traditional medicine activities
� Delay in the establishment of mechanisms for the official
recognition of traditional health practitioners.
� Lack of national policies in the country
� Limited national strategic plans for policy implementation
� Lack of mechanisms of collaboration between practitioners
of conventional and traditional medicine.
� Limited Research Data: There is also a challenge of
limited research data on the safety, efficacy and quality of traditional
medicines and documentation of traditional medicine practices.
� Oral Tradition/Documentation: The oral nature of the
knowledge of traditional medicinal herbs transmitted in various forms from one
generation to another without proper documentation poses a serious challenge in
the preservation of such knowledge.
� Non Inclusion in School Curriculum: Majority of the States
and Local Government
Councils are yet to include some aspects of traditional
medicine in the curricula of Health Science Students and other institutions of
higher learning.
� Lack of National Policy: Majority of countries are yet to
develop National Policies on the conservation of medicinal plants and get
engaged in large-scale cultivation of medicinal plants in botanical gardens.
� Quality Control: There is the challenge of ensuring the
safety and efficacy of herbal medicines, the quality of the source of raw
materials, cultivation and harvesting, field collection, transport and storage,
correct identification of species of medicinal plants.
� Effective Monitoring: Adverse events arising from
consumption of herbal medicines calls for effective monitoring. The issue of
misidentification, adulteration, wrong labeling, contamination with toxic
substances, over dosage, misuse of herbal medicines H both health-care
providers and consumers and the concomitant use of herbal medicine at the same
time with other orthodox medicines.
� Lack of Knowledge: There is challenge of lack of knowledge
of herbal medicine by Health Care regulatory authorities and agencies.
� Conservation/Preservation: Ernest Rukangira (38), observed
that African medicinal plant resources may be doomed to extinction by
overexploitation resulting from excessive commercialization, habitat
destruction and other natural and man-made destructive influence unless serious
conservation measures are taken to ensure their continued availability. This
can be done through establishment of medicinal plant garden and farms.
THE WAY FORWARD
If all the healing and curative
treasures divinely embedded in our medicinal plant by the Mother Nature (the
Supreme Being) will be adequately maximized in improving the health services
being rendered to our people, definite and decisive actions need to be taken.
These include:
� Research: Research in traditional medicine and development
need to be included in the national health research agenda.
� Curriculum: Traditional Medicine should be included in the
curricula of our primary, secondary and tertiary institutions.
� Collaboration: There should be a forum and enabling
environment provided for effective collaboration between Orthodox Medical and
Traditional Medicinal Practitioners. The gulf existing between them which give
room for jealousies and destructive criticisms should be narrowed.
� Protection: Mechanisms for the protection of intellectual
property rights and indigenous herbal knowledge should be developed.
� Training: Establishment of regular training programmes or
National Institute for Traditional or Alternative Medicine, for traditional
medicine practitioners should be encouraged.
� Budget: Countries should be encouraged to create a
budgetary allocation for traditional medicine in their National Health Budget
and include the expenditure of traditional medicinal care in National Health
Accounts.
� Legislation: Legislative framework and national policy for
the protection of the knowledge of medicinal plants as well as it preservation
from wanton destruction through reckless bush burning and tree-cutting should
be put in place.
� Documentation: Government should establish units or
departments for formal documentation of the details of the working of medicinal
plants from the existing oral tradition in order to guard against its
extinction or possible adulteration.
� Packaging & Marketing: The Federal Government and the
Federal Ministry of Health should establish governmental agencies that will
take care of both the packaging and the effective marketing of the traditional
herbals productions both within and outside the country. A Department of
Traditional/Alternative medicine should be created in all Health Ministries at
all levels of government.
(back
to content)
2.7 Traditional medicine
c
Traditional medicine (also known
as indigenous or folk medicine) comprises medical aspects of traditional
knowledge that developed over generations within the folk beliefs of various
societies, before the era of modern medicine. The World Health Organization
(WHO) defines traditional medicine as "the sum total of the
knowledge, skills, and practices based on the theories, beliefs, and experiences
indigenous to different cultures, whether explicable or not, used in the
maintenance of health as well as in the prevention, diagnosis, improvement or
treatment of physical and mental illness".�
Traditional medicine is often contrasted with scientific medicine.
Traditional medicine in a market in Antananarivo, Madagascar
Bot�nicas such as this one in Jamaica Plain, Boston, cater
to the Latino community and sell folk medicine alongside statues of saints,
candles decorated with prayers, lucky bamboo, and other items.
In some Asian and African
countries, up to 80% of the population relies on traditional medicine for their
primary health care needs. When adopted outside its traditional culture,
traditional medicine is often considered a form of alternative medicine.
Practices known as traditional medicines include traditional European medicine,
traditional Chinese medicine, traditional Korean medicine, traditional African
medicine, Ayurveda, Siddha medicine, Unani, ancient Iranian medicine,
traditional Iranian medicine, medieval Islamic medicine, Muti, and If�. Scientific
disciplines that study traditional medicine include herbalism, ethnomedicine,
ethnobotany, and medical anthropology.
The WHO notes, however, that
"inappropriate use of traditional medicines or practices can have negative
or dangerous effects" and that "further research is needed to
ascertain the efficacy and safety" of such practices and medicinal plants
used by traditional medicine systems. As a result, the WHO has implemented a
nine-year strategy to "support Member States in developing proactive
policies and implementing action plans that will strengthen the role
traditional medicine plays in keeping populations healthy."
USAGE AND HISTORY
CLASSICAL HISTORY
In the written record, the study of
herbs dates back 5,000 years to the ancient Sumerians, who described
well-established medicinal uses for plants. In Ancient Egyptian medicine, the
Ebers papyrus from c. 1552 BC records a list of folk remedies and magical
medical practices. The Old Testament also mentions herb use and cultivation in
regards to Kashrut.
Many herbs and minerals used in
Ayurveda were described by ancient Indian herbalists such as Charaka and Sushruta
during the 1st millennium BC. The first Chinese herbal book was the Shennong
Bencao Jing, compiled during the Han Dynasty but dating back to a much earlier
date, which was later augmented as the Yaoxing Lun (Treatise on the Nature of
Medicinal Herbs) during the Tang Dynasty. Early recognised Greek compilers of
existing and current herbal knowledge include Pythagoras and his followers,
Hippocrates, Aristotle, Theophrastus, Dioscorides and Galen.
Roman sources included Pliny the
Elder's Natural History and Celsus's De Medicina. Pedanius Dioscorides drew on
and corrected earlier authors for his De Materia Medica, adding much new
material; the work was translated into several languages, and Turkish, Arabic
and Hebrew names were added to it over the centuries. Latin manuscripts of De
Materia Medica were combined with a Latin herbal by Apuleius Platonicus
(Herbarium Apuleii Platonici) and were incorporated into the Anglo-Saxon codex Cotton
Vitellius C.III. These early Greek and Roman compilations became the backbone
of European medical theory and were translated by the Persian Avicenna (Ibn
Sīnā, 980�1037), the Persian Rhazes (Rāzi, 865�925) and the
Jewish Maimonides.
Some fossils have been used in traditional medicine since
antiquity.
MEDIEVAL AND LATER
Arabic indigenous medicine
developed from the conflict between the magic-based medicine of the
Bedouins and the Arabic translations of the Hellenic and Ayurvedic medical
traditions. Spanish medicine was influenced by the Arabs from 711 to
1492.� Islamic physicians and Muslim botanists
such as al-Dinawari and Ibn al-Baitar significantly expanded on the earlier
knowledge of materia medica. The most famous Persian medical treatise was
Avicenna's The Canon of Medicine, which was an early pharmacopoeia and
introduced clinical trials. The Canon was translated into Latin in the 12th
century and remained a medical authority in Europe until the 17th century. The
Unani system of traditional medicine is also based on the Canon.
Translations of the early
Roman-Greek compilations were made into German by Hieronymus Bock whose herbal,
published in 1546, was called Kreuter Buch. The book was translated into Dutch
as Pemptades by Rembert Dodoens (1517�1585), and from Dutch into English by
Carolus Clusius, (1526�1609), published by Henry Lyte in 1578 as A Nievve
Herball. This became John Gerard's (1545�1612) Herball or General Historie of
Plantes.� Each new work was a compilation
of existing texts with new additions.
Women's folk knowledge existed in
undocumented parallel with these texts. Forty-four drugs, diluents,
flavouring agents and emollients mentioned by Dioscorides are still
listed in the official pharmacopoeias of Europe. The Puritans took
Gerard's work to the United States where it influenced American
Indigenous medicine.
Francisco Hern�ndez, physician to
Philip II of Spain spent the years 1571�1577 gathering information in Mexico and
then wrote Rerum Medicarum Novae Hispaniae Thesaurus, many versions of which
have been published including one by Francisco Xim�nez. Both Hernandez and
Ximenez fitted Aztec ethnomedicinal information into the European
concepts of disease such as "warm", "cold", and
"moist", but it is not clear that the Aztecs used these categories.
Juan de Esteyneffer's Florilegio medicinal de todas las
enfermedas compiled European texts and added 35 Mexican plants.
Mart�n de la Cruz wrote an herbal
in Nahuatl which was translated into Latin by Juan Badiano as Libellus de
Medicinalibus Indorum Herbis or Codex Barberini, Latin 241 and given to King
Carlos V of Spain in 1552. It was apparently written in haste and
influenced by the European occupation of the previous 30 years. Fray
Bernardino de Sahag�n's used ethnographic methods to compile his codices that
then became the Historia General de las Cosas de Nueva Espa�a, published in
1793. Castore Durante published his Herbario Nuovo in 1585 describing medicinal
plants from Europe and the East and West Indies. It was translated into German in
1609 and Italian editions were published for the next century.
COLONIAL AMERICA
In 17th and 18th-century America,
traditional folk healers, frequently women, used herbal remedies, cupping and
leeching. Native American traditional herbal medicine introduced cures for
malaria, dysentery, scurvy, non-venereal syphilis, and goiter problems. Many of
these herbal and folk remedies continued on through the 19th and into the 20th
century, with some plant medicines forming the basis for modern pharmacology.
MODERN USAGE
The prevalence of folk medicine
in certain areas of the world varies according to cultural norms. Some modern
medicine is based on plant phytochemicals that had been used in folk medicine.
Researchers state that many of the alternative treatments are
"statistically indistinguishable from placebo treatments".
KNOWLEDGE TRANSMISSION AND CREATION
Indigenous medicine is generally transmitted
orally through a community, family and individuals until "collected".
Within a given culture, elements of indigenous medicine knowledge may be
diffusely known by many, or may be gathered and applied by those in a
specific role of healer such as a shaman or midwife. Three factors
legitimize the role of the healer � their own beliefs, the success of their
actions and the beliefs of the community. When the claims of indigenous
medicine become rejected by a culture, generally three types of adherents still
use it � those born and socialized in it who become permanent believers, temporary
believers who turn to it in crisis times, and those who only believe in
specific aspects, not in all of it.
DEfiNITION AND TERMINOLOGY
Traditional medicine may
sometimes be considered as distinct from folk medicine, and the considered to
include formalized aspects of folk medicine. Under this definition folk
medicine are longstanding remedies passed on and practiced by lay people. Folk
medicine consists of the healing practices and ideas of body physiology and
health preservation known to some in a culture, transmitted informally as
general knowledge, and practiced or applied by anyone in the culture having
prior experience.
FOLK MEDICINE
|
�
|
Curandera performing a limpieza in Cuenca, Ecuador
Many countries have practices
described as folk medicine which may coexist with formalized, science-based,
and institutionalized systems of medical practice represented by conventional
medicine. Examples of folk medicine traditions are traditional Chinese medicine,
Iranian traditional medicine, traditional Korean medicine, Arabic indigenous
medicine, Uyghur traditional medicine, Japanese Kampō medicine,
traditional Aboriginal bush medicine, Native Hawaiian Lāʻau
lapaʻau, and Georgian folk medicine, among others.
AUSTRALIAN BUSH MEDICINE
Generally, bush medicine used by
Aboriginal and Torres Strait Islander people in Australia is made from plant
materials, such as bark, leaves and seeds, although animal products may be used
as well. A major component of traditional medicine is herbal medicine, which is
the use of natural plant substances to treat or prevent illness.
NATIVE AMERICAN MEDICINE
American Native and Alaska Native
medicine are traditional forms of healing that have been around for thousands
of years. There are many ethnobotany plants involved in traditional medicine
for Native Americans and some are still used today.� When it comes to Native American traditional
medicine, the ideas surrounding health and illness within the culture are
virtually inseparable from the ideas of religion and spirituality. Healers
within indigenous communities go by many names ranging from medicine man or
woman to herbalist or even shaman and are considered spiritual or religious
leaders within their respective tribes. When it comes to healing, tribal
healers would look at a plant's characteristics to determine its efficacy for
the treatment of an illness. Specific plant characteristics such as plant
shape, smell, color, and taste could aid in determining how the plant could be
used as a remedy.� The Meskwaki tribe
found they could use the juice from Arum maculatum for snakebites. This was
inferred from the milky appearance of the juice from the plant which is said to
resemble snake venom, and the plant's shape resembled the head of a snake.
Native Americans used foxglove herb as a treatment for an illness they referred
to as dropsy or edema, which is fluid buildup typically in the lower
legs, and its common cause is heart failure. In modern medicine, foxglove
extract is still used under the name digitalis, and its purpose is to moderate
the heart rate. Native Americans were successful with some medical practices,
such as treating fevers, gastrointestinal conditions, skin rashes, setting
bones, as well as birthing babies, and aiding mothers in healing. A study conducted
within an IHS hospital that allows Navajo healers to visit patients found that
the hospital had an 80 percent success rate in getting comatose patients back to
consciousness, which is higher than the rate of present-day biomedical
management hospitals. The tribe Anthemideae used the plant family Asteraceae
for orthopedic aids and pulmonary aids, specifically the plant's Achillea
and Artemisia. A study conducted amongst 14 different tribes within North
America found that Asteraceae was the most widely used plant family for its
medicinal properties.
NATTUVAIDYAM
Nattuvaidyam was a set of
indigenous medical practices that existed in India before the advent of allopathic
or western medicine. These practices had different sets of principles and ideas
of the body, health and disease. There were overlaps and borrowing of ideas,
medicinal compounds used and techniques within these practices. Some of these
practices had written texts in vernacular languages like Malayalam, Tamil,
Telugu, etc. while others were handed down orally through various mnemonic
devices. Ayurveda was one kind of nattuvaidyam practised in south India. The
others were kalarichikitsa (related to bone setting and musculature),
marmachikitsa (vital spot massaging), ottamoolivaidyam (single dose medicine or
single time medication), chintamanivaidyam and so on. When the medical system
was revamped in twentieth century India, many of the practices and techniques
specific to some of these diverse nattuvaidyam were included in Ayurveda.
HOME REMEDIES
A home remedy (sometimes also
referred to as a granny cure) is a treatment to cure a disease or ailment that
employs certain spices, herbs, vegetables, or other common items. Home remedies
may or may not have medicinal properties that treat or cure the disease or
ailment in question, as they are typically passed along by laypersons (which
has been facilitated in recent years by the Internet). Many are merely used as
a result of tradition or habit or because they are effective in inducing the
placebo effect.
One of the more popular examples
of a home remedy is the use of chicken soup to treat respiratory infections
such as a cold or mild flu. Other examples of home remedies include duct
tape to help with setting broken bones; duct tape or superglue to treat plantar
warts; and Kogel mogel to treat sore throat. In earlier times, mothers were
entrusted with all but serious remedies. Historic cookbooks are frequently full
of remedies for dyspepsia, fevers, and female complaints. Components of the aloe
vera plant are used to treat skin disorders. Many European liqueurs or
digestifs were originally sold as medicinal remedies. In Chinese folk medicine,
medicinal congees (long-cooked rice soups with herbs), foods, and soups are
part of treatment practices.
CRITICISM
SAFETY CONCERNS
Although 130 countries have
regulations on folk medicines, there are risks associated with the use of them (i.e.
zoonosis, mainly as some traditional medicines still use animal-based
substances). It is often assumed that because supposed medicines are natural
that they are safe, but numerous precautions are associated with using herbal
remedies.
USE OF ENDANGERED SPECIES
�
Sometimes traditional medicines include parts of endangered
species, such as the slow loris in Southeast Asia.
Endangered animals, such as the slow loris, are sometimes
killed to make traditional medicines.
Shark fins have also been used in traditional
medicine, and although their effectiveness has not been proven, it is hurting
shark populations and their ecosystem.
The illegal ivory trade can partially be traced back to
buyers of traditional Chinese medicine. Demand for ivory is a huge factor in
the poaching of endangered species such as rhinos and elephants.
(back
to content)
2.8 TRADITIONAL AFRICAN MEDICINE
Traditional African medicine is a
range of traditional medicine disciplines involving indigenous herbalism and
African spirituality, typically including diviners, midwives, and herbalists.
Practitioners of traditional African medicine claim to be able to cure a
variety of diverse conditions including cancer, psychiatric disorders, high
blood pressure, cholera, most venereal diseases, epilepsy, asthma, eczema,
fever, anxiety, depression, benign prostatic hyperplasia, urinary tract infections,
gout, and healing of wounds and burns and even Ebola.
Diagnosis is reached through
spiritual means and a treatment is prescribed, usually consisting of a herbal
remedy that is considered to have not only healing abilities but also symbolic
and spiritual significance. Traditional African medicine, with its belief
that illness is not derived from chance occurrences, but through spiritual or
social imbalance, differs greatly from modern scientific medicine, which
is technically and analytically based. In the 21st century, modern
pharmaceuticals and medical procedures remain inaccessible to large numbers of
African people due to their relatively high cost and concentration of health facilities
in urban centres.
Traditional medicine was the
dominant medical system for millions of people in Africa prior the arrival of
the Europeans, who introduced western-based medicine, which was a noticeable
turning point in the history of this tradition and culture.� Herbal medicines in Africa are generally not
adequately researched, and are weakly regulated There is a lack of the detailed
documentation of the traditional knowledge, which is generally transferred
orally. Serious adverse effects can result from mis-identification or
misuse of healing plants.
The geographical reach of this article is Sub-Saharan
Africa. Though, of course neighbouring medical traditions influenced
traditional African medicine.
HISTORY
COLONIAL ERA
Modern science has considered
methods of traditional knowledge as primitive and under colonial rule some
traditional medical practices were outlawed. During this time, attempts were
also made to control the sale of herbal medicines. For example, after Mozambique
gained independence in 1975, attempts to control traditional medicine went as
far as sending diviner-healers to re-education camps as colonialism and
Christianity spread through Africa, colonialists built general hospitals and
Christian missionaries built private ones, with the hopes of making headway
against widespread diseases. However, little was done to investigate the
legitimacy of the traditional medical practices, despite the obvious role that
the traditional healers played in the basic health needs of their communities;
the colonial authorities along with doctors and health practitioners continued
to shun their contributions. It was also believed that during times of
conflict people were more likely to resort to supernatural explanations
and would seek treatment involving the supernatural.
MODERN PERIOD
 �Nurse at Koidu Hospital
in Sierra Leone consulting with patients
�Nurse at Koidu Hospital
in Sierra Leone consulting with patients
For various reasons, in the late
20th century the traditional systems of medical care in developing countries underwent
a major revival. These countries also realized that modern health care systems
and the technologies that they are dependent on are not locally manufactured
and maintained thus making them expensive and rendering the population
dependent on supply-chains that might be erratic or politicised. Due to this,
interest in integrating traditional African medicine into the continent's
national health care systems has increased and the use of traditional medicinal
plants is being encouraged in some countries. An African healer embraced this
concept by starting a 48-bed hospital, the first of its kind, in
Kwa-Mhlanga, South Africa, which combines traditional African methods with
other alternative medical practices such as homeopathy, iridology, and
traditional Asian medicine.
DIAGNOSTICS
The medical diagnoses and chosen
methods of treatment in traditional African medicine rely heavily on spiritual aspects,
often based on the belief that psycho-spiritual aspects should be addressed
before the medical aspects. There is the belief among the practitioners of
traditional healing that the ability to diagnose and treat illnesses are a gift
from God. Rather than looking for the medical or physical reasons behind an
illness (or a spell of bad luck), traditional healers attempt to determine the
root cause underlying it, which is believed to stem from a lack of balance
between the patient and their social environment or the spiritual world. In
other words, supernatural causes, not natural causes, are attributed to
illnesses. According to the type of imbalance the individual is experiencing,
an appropriate healing plant will be used, which is valued for its symbolic and
spiritual significance as well as for its medicinal effect.
When a person falls ill, a
traditional practitioner uses incantations to make a diagnosis. The
incantations are thought to give the air of mystical and cosmic connections.
Divination is typically used if the illness is not easily
identified,� otherwise, the
sickness may be quickly diagnosed and a remedy�
prescribed. Sometimes the practitioner will advise the patient to
consult a diviner who can give a diagnosis and recommend a treatment. It is
believed that contact with the spirit world through divination often requires
not only medication, but sacrifices.
TREATMENTS
Traditional practitioners use a wide variety of treatments
ranging from standard medical treatments to the pseudoscientific and
"magical". Treatments may include fasting, dieting, herbal therapies,
bathing, massage, and surgical procedures. Examples of the pseudoscientific
treatments include:
The use of
"bleed-cupping" (also called "wet cupping"), followed by herbal
ointment and herbal drugs to treat Migraines, coughs, abscesses, and pleurisy.
Some cultures rub hot herbal ointment across the patient's
eyelids to treat headaches.
A steaming mixture of herbs is
both consumed and inhaled in the treatment of Malaria. Fevers are often treated
using a steam bath.
Vomiting induced by emetics is used to treat alcoholism.
The fat of a boa constrictor is
used to treat gout and rheumatism, and is thought to relieve chest pain when
applied topically.
Animals are also sometimes used
to transfer the illness to afterward or for the manufacture of medicines for
zootherapy. For example, the bones of baboons are used to treat arthritis.
The terpenoids of the blister
beetle (Mylabris sp.) are rubbed into the skin as a treatment for skin
diseases.
Consensus between traders of the
components of the medication used by practitioners of traditional African
medicine regarding what should be used to treat different illnesses varies considerably,
even within a small area such as the Faraday Street market in Johannesburg,
South Africa. However, approximately 60%-80% of the people in Africa rely on
traditional remedies to treat themselves for various diseases. A 2018
systematic review estimated that close to 60% of the general population in
sub-Saharan Africa regularly use traditional and complementary medicine
products for themselves and to treat their animals for various diseases. Ebola
survivors in Sierra Leone have recently been reported to use traditional
medicine alone or together with conventional medicine.
MEDICINAL PLANTS
Prunus africana with stripped bark
There are many plants in Africa
that can be used for medicinal purposes and more than 4000 are used for this
purpose in the tropical regions of Africa. Medicinal plants are used in the
treatments of many diseases and illnesses, the uses and effects of which are of
growing interest to Western societies. Not only are plants used and chosen for
their healing abilities, but they also often have symbolic and spiritual significance.
For example, leaves, seeds, and twigs that are white, black and red are seen as
especially symbolic or magical and are believed to possess special properties.
Preparing and drying out freshly dug traditional medicines
(muti)
One example of a medicinal plant
is Pygeum (Prunus africana), which has been used as a treatment for mild benign
prostatic hyperplasia in Europe since the 1970s. Although used extensively in Africa,
there is insufficient evidence for its effectiveness in treating fever,
inflammation, kidney disease, malaria, stomach aches and other
conditions. In traditional African practice, the bark is made into tea, whereas
elsewhere in the world it is found in powders, tinctures, and pills.
A 2007 study investigated the
effectiveness of 16 plants, growing in South Africa's KwaZulu- Natal region, in
lowering blood pressure "by acting as an ACE inhibitor." Of the 16
plants, only one (Tulbaghia violacea) showed promise. It then was tested on
rats and "demonstrated hypotensive activity", i.e. reduction of blood
pressure. The plants included in the study were:
1. Amaranthus dubius, a flowering plant, also known as
spleen amaranth
2. Amaranthus hybridus, commonly known as smooth pig-weed or
slim amaranth
3. Amaranthus spinosus, also known as spiny amaranth
4. Asystasia gangetica, an ornamental ground cover known as
Chinese violet.
5. Centella asiatica, a small herbaceous annual plant
commonly referred to as Asiatic pennywort
6. Ceratotheca triloba, a tall annual plant that
flowers in summer sometimes referred to as poppy sue
7. Chenopodium album, also called lamb's quarters, this is a
weedy annual plant
8. Emex australis, commonly known as southern three corner jack
9. Galinsoga parviflora, commonly referred to as
gallant soldier
10. Justicia flava, also known as yellow justicia
11. Momordica balsamina, also known as the balsam apple
12. Oxygonum sinuatum, an invasive weed with no common name
13. Physalis viscosa, known as starhair ground cherry
14. Senna occidentalis, a very leafy tropical shrub, also
called septic weed
15. Solanum nodiflorum, also known as white nightshade
16. Tulbaghia violacea, a bulbous plant with hairless leaves
often referred to as society or wild garlic.
A 2008 literature survey was made
to assess the botanical knowledge and uses within traditional medicine in
Southern Africa for the genus Aloe within the family Asphodeloideae. Most
common medical uses were for the treatment of "infections, internal parasites,
digestive ailments and injuries." Socially the plants are used as ingredients
in tobacco snuff. A 2014 literature survey found that at least 12 palm species
in sub-Saharan Africa are used in various ritual practices, including the use of
palm oil in healing mixtures.
In 2016 an in vitro study of the
essential oil from Erigeron floribundus, used as a medicinal plant in
Cameroon, demonstrated good activity against Staphylococcus aureus,
"cytotoxicity on colon carcinoma cells" and "ferric reducing antioxidant
power." Among the constituents of the essential oil are spathulenol and
limonene.
As a result of a study conducted
from 2011 to 2016, a traditional medicine from the tropical Olon tree, and
another species of genus Zanthoxylum, was found to have synergistic compounds
that kill both mosquitoes and their plasmodium parasites.
A 2000 study of thirty-three
species of plants, found in the Eastern Cape province of South Africa, that are
considered weeds, alien invaders or problem plants were investigated for their
uses in traditional medicine. The plants included:
Anredera cordifolia leaves
Anredera cordifolia (iDlula).
Swollen feet from poor circulation and/or liver and kidney problems are treated
with a leaf poultice, while the sap is used to treat a rash caused by contact
with dirty water.
Cannabis Sativa plant
Araucaria bidwillii
(iNdiyandyiya). Grated bark mixed with water is consumed to treat amenorrhea
caused by congenital problems, tuberculosis and malnutrition.
Bidens pilosa (uMhlabangubo). The
water from the boiled roots is consumed to treat infertility in women. Bathing
in water in which the leaves have been soaked is believed to protect one from
evil spirits (imoya emdaka), ill feeling, jealousy or animosity. Also used to
treat diarrhoea, colic, rheumatism, syphilis, earache, constipation, intestinal
worms, Malaria, ring worm, jaundice and coughs.
�Carduus tenuiflorus plant
Cannabis sativa (iNtsango).
Various parts of the plant are used to treat asthma, bronchitis, headache,
epilepsy, pains, colds, influenza, labour pains, hypertension, diabetes,
malaria, blackwater fever, blood-poisoning, anthrax, dysentery, tetanus, menstrual
cramps and rabies.
Carduus tenuiflorus
(uMhlakavuthwa). The patient is given an emetic and instructed to vomit onto
the plant. The belief is that the plant will "suck out the cause of the
illness."
Datura stramonium plant
Datura stramonium
(uQhwangu-qhwangu). The leaves are used to treat pain and swelling (including
after a circumcision), boils and abscesses, measles, asthma and headaches,
tetanus, foot ailments and respiratory conditions.
Emex australis plant
Emex australis (iNkunzane). A
decoction of the root is used to treat constipation, biliousness and other
stomach complaints and to stimulate appetite.
Galenia secunda
(uMvenyathi).� The roots are mixed with
Emex australis, boiled and used to treat kidney pains in adults and colic in
babies.
Lantana camara plant
Lantana camara (iQunube). The roots are boiled and the
liquid consumed for lower back or abdominal pain, or used as an enema to treat gonococcal
infections and urinary tract infections. It is also used to treat coughs,
colds, jaundice, rheumatism and as a contraceptive.
Opuntia ficus-indica
(iTolofiya). A poultice of the cooked leaves is used to treat sores
between toes and the fingers caused by fungal infections. The belief is
that these sores are caused by "dirty blood" (igazi elimdaka).
Rumex sagittatus plant
Rumex sagittatus (iBhathatha). A
cold water infusion of the roots are used as a body wash as it is believed to
cleanse the body of misfortunes and evil.
�Schinus molle plant
�
Schinus molle (iPepile or
Peperboom). Fever and influenza are treated by consuming a leaf decoction
or steaming. A combination of leaves and bark is used to treat wounds.
Araujia sericifera (iQuwa). It is
used to treat amafufunyana, which is described by Ngubane as an extreme form of
depression coupled with psychotic symptoms such as delusions, hysteria, violent
outburst and suicide ideations. The roots are mixed with other medications to
treat it.
Argemone mexicana
(iKhakhakhakha).� This root decoction is
mixed with the roots of the rubus pinnatus (iqunube) and is administered
through the use of an enema to cure kidney pain.
Spirituality
Bedik diviner outside Iwol,
southeast Senegal (West Africa). He makes predictions base on the color of the
organs of sacrificed chickens.
Some healers may employ the use of
charms, incantations, and the casting of spells in their treatments. For
example, there is the belief among the Ibos of Nigeria that medicine men can
implant something into a person from a distance to inflict sickness on
them, in a process referred to asegba ogwu. To remove the malignant object, the
intervention of a second medicine man is typically required, who then removes
it by making an incision in the patient. A form of sympathetic magic is also
used, in which a model is made of the victim and it is believed that actions
performed on the model are transferred to the victim, in a manner similar to
the familiar voodoo doll. Superstitious beliefs regarding spirits are also
exploited and people are convinced that "spirits of deceased relatives
trouble the living and cause illness." In these instances, "medicine
men prescribe remedies, often in the form of propitiatory sacrifice, in
order to put them to rest so that they will no longer trouble the living,
especially children."
According to Onwuanibe, Africans
hold a religious world view which includes divine or spiritual intervention in
medical practice. For example, the !Kung people of the Kalahari Desert� believe that the great� God Hishe created all things� and, therefore, controls all sickness and
death. Hishe presents himself to these medicine men in dreams and
hallucinations, giving them curative power and this god is generous enough to
give this power to the medicine men, they are expected to practice healing
freely. The !Kung medicine men effect a treatment by performing a tribal dance.
TRADITIONAL MEDICINAL PRACTITIONERS
|
�
|
Inyanga/Sangoma from Johannesburg, South Africa
�Successful Cesarean
section performed by indigenous healers in Kahura, Uganda. As observed by R. W.
Felkin in 1879.
Many traditional medicinal
practitioners are people without formal education, who have rather received
knowledge of medicinal plants and their effects on the human body from their
forebears and by observation. Traditional practitioners and their practices
vary but common features among them are a personal involvement in the healing process;
protection of the therapeutic knowledge by keeping it a secret; and being
rewarded for their services.
In a manner similar to orthodox
medicinal practice, the practitioners of traditional medicine specialize in
particular areas of their profession. Some, such as the inyangas of Eswatini
are experts in herbalism, whilst others, such as the South African sangomas, are
experts in spiritual healing as diviners, and others specialize in a
combination of both forms of practice. There are also traditional bone setters
and birth attendants. Herbalists are becoming more and more popular in Africa
with an emerging herb trading market in Durban that is said to attract between
700,000 and 900,000 traders per year from South Africa, Zimbabwe, and
Mozambique. Smaller trade markets exist in virtually every community. Their
knowledge of herbs has been invaluable in African communities and they among
the few who could gather them in most societies. Midwives also make extensive
use of indigenous plants to aid childbirth.�
African healers commonly "describe and explain illness in terms of
social interaction and act on the belief that religion permeates every aspect
of human existence."
PAYMENTS
Traditional healers, like any
other profession, are rewarded for their services. In African societies, the
payment for a treatment depends on its efficacy. They do not request payment
until after the treatment is given. This is another reason many prefer traditional
healers to western doctors who require payment before the patient has assessed
the effectiveness of the treatment. The payment methods have changed over time,
with many practitioners now asking for monetary payment, especially in urban settings,
rather than their receiving good in exchange, as happened formerly. There are
also a growing number of fraudulent practitioners who only interested in making
money, especially in urban areas.
LEARNING THE TRADE
Some healers learn the trade
through personal experience while being treated as a patient who decide to
become healers upon recovery.� Others become
traditional practitioners through a "spiritual calling" and,
therefore, their diagnoses and treatments are decided through belief in
supernatural intervention. Another route is to receive the knowledge and skills
passed down informally from a close family member such as a father or uncle, or
even a mother or aunt in the case of midwives. Apprenticeship to an established
practitioner, who formally teaches the trade over a long period of time and is
paid for their tutoring, is another route to becoming a healer.
IMPORTANCE
In Africa, traditional healers
and remedies made from indigenous plants play a crucial role in the health of
millions since as many as 85% of African routinely use these services for
primary health care in Sub-Saharan Africa. The relative ratios of traditional
practitioners and university trained doctors in relation to the whole
population in African countries underscores this importance. Across Sub-Saharan
Africa, from Ghana to Eswatini there are, on average almost, 100 traditional practitioners
for every university trained doctor. This equates to one traditional healer for
every 200 people in the Southern African region, which is a much greater
doctor-to- patient ratio than is found in North America. In many parts of Africa
there are few practitioners trained in modern medicine and traditional healers
are a large and influential group in primary health care and an integral part
of the African culture.� Without them,
many people would go untreated.
Medications and treatments that
Western pharmaceutical companies manufacture are far too costly and not
available widely enough for most Africans.�
Many rural African communities are not able to afford the high price of
pharmaceuticals and can not readily obtain them even if they were affordable;
therefore, healers are their only means of medical help. Because this form of
medicine is "the most affordable and accessible system of health care for
the majority of the African rural population," the African Union declared
2001 to 2010 to be the Decade for African Traditional Medicine with the goal of
making "safe, efficacious, quality, and affordable traditional
medicines available to the vast majority of the people."
Excessive use of plants is an ecological risk, as this may
lead to their extinction.
TRADITIONAL AFRICAN MEDICINE IN RELATION TO WOMEN
Women in Sub-Saharan rural
African communities are almost entirely responsible for domestic work in their
households. These women are often at higher risk for disease and poverty than
their male counter-parts and have less control over their daily lives than
them.� A literature survey from 2001
found that these women defined �good health� as the ability to perform
domestic duties and the state of being disease free. Furthermore, the study found
that they attributed poor health to supernatural, evil forces, that illness is
seen as a form of punishment from spirits. In another study, which explored the
HIV/AIDS epidemic in Ghana, women identified HIV/AIDS with reprobate
behaviour, such as �prostitution, promiscuity, and extramarital relationships�,
or traveling to areas outside the community.
These women endure arduous conditions
and a traditional healer plays an instrumental role in their daily lives. The
traditional healer provides health care to the rural communities and represents
him/herself as an honorable cultural leader and educator. An advantage of the
traditional healer in rural areas is that they are conveniently located within
the community. Modern medicine is normally not as accessible in rural areas
because it is much more costly. Older rural women particularly tend to utilize
traditional healers in their communities. Younger women and the urbanized have
been found to be renouncing the use of traditional healers.
A 2001 study of rural Ethiopian women
where HIV was present found that they rejected the presence of HIV in rural
villages and claimed it was an urban illness, despite the presence of HIV in
the rural communities. However, these women also claimed that their communities
did not advocate for prevention, but rather treated an illness once it was
present.
TRADITIONAL AFRICAN HEALERS AND THE HIV/AIDS EPIDEMIC ROLE
For HIV/AIDS victims, traditional
healers provided a local, familiar, and accessible option compared to
biomedical personnel who were usually overbooked and located farther away.
Traditional healers were seen as having an authoritative role in physical, psychological,
and spiritual aspects of health. In the early 1980s in southwestern Uganda, it
was reported that many locals infected with the disease ("Slim")
after showing symptoms of diarrhoea and weight- loss would consult traditional
healers due to their belief in the connection between the disease and
witchcraft.
CRITICISM
During the HIV/AIDS epidemic
traditional healers� methods were criticised by practitioners of modern
medicine, and in particular the use of certain herbal treatments for HIV/AIDS.
According to Edward Mills, herbal remedies are used as a therapy for
HIV-symptoms such as �dermatological disorders, nausea, depression, insomnia,
and weakness.� While some of these remedies have been beneficial, the
herbal treatments hypoxis and sutherlandia �may put the patients at risk for
antiretroviral treatment failure, viral resistance, or drug toxicity� since
they interact with antiretroviral treatments and prevent the expression of
CYP3A4 and P-glycoprotein. This results in the inhibition of drug metabolism
and transport. Peltzer et al. also found that an important issue with herbal
medicines used in traditional medicine is that when a patient decides to see a
doctor in addition to a traditional healer, they do not always mention that he
or she is taking an herbal medicine. Herbal medicines can interact with the
modern medicine prescribed by the doctor to treat HIV and negatively impact the
patient. Peltzer et al. mentions that a �IGM-1 seem to be effective in symptom
improvement, but generally no significant effect on antiviral or immunity
enhancement among reviewed herbs was seen� for the treatment of HIV. Since HIV is
such a volatile disease, it is imperative to try to boost the patient's
immunity, not just relieve symptoms.
The ethical issue, as presented
by modern medicine, is the complete lack of clinical trials to test any
traditional African medicine before practicing with it on the public. Modern medicine
in the United States is subject to The Nuremberg Code and the related
Declaration of Helsinki which are the basis for the Code of Federal Regulations
issued by the United States Department of Health and Human Services, to oblige
humane behavior in experimenting on the public for the good of society. Since
traditional African healers do not have to adhere to the Nuremberg code, there is
a potential danger to society when healers do not practice medicine humanely.
Traditional healers have also been
under scrutiny during the HIV/AIDS epidemic for unsanitary medical practices.
The �re-use of medical instruments and lack of hygienic habits such as hand
washing� have contributed to the spread of infectious diseases by traditional
healers. A study of traditional healers in Nigeria found that 60% of the
population was at risk because of the contamination spread by tradition
healers.
Women experience the most fatal
impact from the HIV/AIDS epidemic. When industrial development required the
labor of men from rural communities, the men often� left those communities and while away at the
migratory camps many of these men would have sex with prostitutes, become
infected with HIV and return home� with
it.Furthermore, since traditional medicine does not have an early detection
method, infectious diseases are often�
spread unknowingly, allowing the 3.1 million people infected with HIV in
sub-Saharan Africa to grow exponentially to 25.4 million in 2004. The
patriarchal culture that defines traditional marriages in rural areas,
places female sexuality under male control and decrees that women are not
permitted to discuss and practice safe sex with their partners, which results
in a higher risk for HIV exposure for women in rural areas.
MODERN MEDICINE
Sub-Saharan countries have found
ways to unite modern medicine with traditional medicine due to the urgency of the
HIV/AIDS epidemic. In South Africa, the Kundalia Foundation has provided
funding to train traditional healers on HIV/AIDS. The training included
prevention, safe sex, and knowledge about the virus.
RELATIONSHIP WITH MODERN MEDICINE
Traditional African medicine
served the people in Africa prior to the establishment of science- based
medicine, but with the arrival of Europeans this changed. Although modern
scientific medicine is successful in developed countries, it doesn't have
the same positive impact in many of the underdeveloped African countries.
Though science-based practices can make an impact in health care practices, in
certain areas such as in the spread of various diseases, it cannot integrate
wholly into the culture and society. This makes the traditional African
practitioners a vital part of their health care system. There are many reasons
why the modern medical system has not been as effective in Africa as it has in
more developed parts of the world. Hospitals and medical facilities are
difficult for many Africans to get to. With vast areas of land and poor
road and transportation systems, many native Africans have to travel immense
distances on foot to reach help. Once they arrive they are often required to
wait in line for up to 8 hours, especially in urban areas, as the lack of
clinics and resources cause over-crowding. Patients are often not told the
cause of their illness or much information about it all, so they have no way to
prevent or prepare for it. The technology used is usually of poor quality,
which impairs the quality of treatment. Modern medicine can also be too
expensive for the average African to afford, making it difficult for them
to receive proper care.� Finally, modern
medicine removes native Africans from the culture and tradition and forces them
into a setting that they are not comfortable with, away from their family and
traditions which are of utmost importance to them.� They do not get the proper spiritual healing that
their culture seeks and traditional ideology requires.
However, there has been more
interest expressed recently in the effects of some of the medicinal plants of
Africa. "The pharmaceutical industry has come to consider traditional
medicine as a source for identification of bio-active agents that can be
used in the preparation of medicine." Pharmaceutical industries are
looking into the medicinal effects of the most commonly and widely used plants
to use in drugs. In comparing the techniques of African healers and Western
techniques, T. Adeoze Lambo, a Nigerian psychiatrist, stated in 1979, "At
about three years ago, we made an evaluation, a programme of their work, and
compared this with our own, and we discovered that actually they were scoring
almost sixty percent success in their treatment of neurosis. And we were
scoring forty percent-in fact, less than forty percent."
EFFECTIVENESS
Herbal medicines in Africa are
generally not adequately researched, and are weakly regulated. There is a lack
of the detailed documentation of the traditional knowledge, which is generally
transferred orally. A literature survey in 2014, indicated that several African
medicinal plants contain bioactive anti-trypanosomal compounds that could be
used for the treatment of African trypanosomiasis ("Sleeping
sickness") but no clinical studies had been conducted on them. A 2008
literature survey found that only a small proportion of ethnoveterinary
medicine plants in South Africa had been researched for biological activity. A
literature survey conducted in 2013 identified several compounds (mostly glucosides,
sterols and sterolins) contained in the Hypoxis species, (known locally as inkomfe
or African potato) that had been isolated and tested with "promising
prospects reported in some studies". South African sangomas have been long
and vocal advocates of a local traditional plant called unwele or kankerbos
(Sutherlandia frutescens) claiming it assists in the treatment of HIV/AIDS,
cancer and tuberculosis. A review of preclinical data on Sutherlandia
frutescens show no toxity and justify controlled clinical studies. However,
when used in conjunction with antiretroviral treatments, the herbal treatments
hypoxis and sutherlandia �may put the patients at risk for antiretroviral
treatment failure, viral resistance, or drug toxicity� since they interact with
antiretroviral treatments and prevent the expression of CYP3A4 and
P-glycoprotein.
There have been attempts to assess some traditional
medicines through clinical trials, although none have so far reached phase III.
SAFETY
A small proportion of ethnoveterinary
medicine plants in South Africa have been researched for toxic effects. The possible
adverse effects of South African traditional medicines are not well documented;
there has been limited research into mutagenic properties and heavy metal
contamination. Serious adverse effects, even death, can result from
misidentification or misuse of healing plants. For example, various aloe
plants are widely used in traditional African medicine, but some varieties,
such as Aloe globuligemma, are toxic and can cause death. The potential for
traditional African medicine and pharmacokinetic interactions is unknown,
especially interactions between traditional treatments and antiretroviral drugs
for HIV/AIDS. Herbal treatments are frequently used in Africa as a primary
treatment for HIV/AIDS and for HIV-related issues. Collaboration with traditional
healers has been recommended to determine what herbal treatments are used for
HIV and to educate people supplying alternative treatments against unsafe
practices. Given the demands of the local population on the use of traditional
African medicine, it has been proposed that South African medical schools
should inform medical students about traditional, supplementary and alternative
medicine and the possible conflicts and interactions with modern
medicine. Use of traditional African medicines as antivirals instead of using
specific antiretroviral drugs, is especially a risk with HIV.
Cultural expectations play an
important role in treatment as a 1985 study amongst the Mende people of Sierra
Leone showed that treatment decisions were made "largely on traditional
notions of the efficacy of a medicine of a particular color, consistency,
taste, size and reputed success in treating analogous illnesses". This led
to the inappropriate use of many modern medicines by the Mende.
(back
to content)
2.9 Traditional and Modern Medicine: Harmonizing the Two Approaches i
Summary
1. Traditional medicine
2.1 Background and characteristics
2.2 Changes in trends of usage
2.3 Consumers, government and other stakeholders
3. Traditional and modern medicine
3.1 Integration of traditional medicine with modern medicine
3.2 The need for harmonization of traditional and modern
medicine
4. Evidence and traditional medicine
4.1 Acquisition of traditional medical knowledge
4.2. Evidence�based health care practice
5. Evidence of practice of traditional medicine
5.1 Basic science research in acupuncture
5.2 Clinical research on acupuncture
5.3 Basic science research in herbal medicine
5.4 Clinical research in herbal medicine
6. Harmonizing traditional and modern medicine: Conclusions
and recommendations
6.1 Towards harmonization of traditional and modern medicine
6.2 Operational recommendations
SUMMARY
The major aims of the meeting
held in Beijing China, from 22 to 26 November 1999 were to evaluate the
contemporary role of traditional medicine in maintaining health, to develop a
scientific approach to policy�making in traditional medicine, and, ultimately,
to assess how traditional medicine can be harmonized with modern medicine. The
meeting also provided a forum for identifying research requirements in
traditional medicine.
The meeting was attended by 24
temporary advisers, three consultants, one secretariat staff from the WHO
Regional Office for the Western Pacific, and 19 observers.
Participants presented review
papers on past research, barriers to the acceptance of traditional medicine,
research methodology and evidence�based medicine. Participants were divided
into sub�groups to deal with acupuncture, herbal medicine and socio�economic
aspects relevant to harmonization.
In the course of these
discussions, the meeting concluded that there were challenges to the
harmonization of traditional and modern medicine. Better access to information,
facilitating appropriate clinical trials, improving rigour in clinical trials,
improving education and collaboration of practitioners and researchers, and
respecting traditional practices in research, were all identified as important
steps towards achieving harmonization.
The group concluded that WHO
should continue to encourage governments to adopt policies to promote rational
and safe use of traditional medicine. WHO and its Member States should support
the harmonization and appropriate integration of traditional medicine with
modern medicine.
The group believed that evidence�based research could be an
essential step towards the harmonization. In addition to detailed
recommendations on steps for harmonizing the two approaches, the meeting also
provided the following recommendations:
(1) WHO should continue to
encourage governments to adopt policies to promote rational and safe use of
traditional medicine.
(2) WHO and its Member States
should support the harmonization and appropriate integration of traditional
medicine with modern medicine.
(3) Findings of well�designed and
well�performed research should be disseminated as widely as possible. This
should include the preparation and dissemination in English and native
languages of rigorous systematic reviews based on the research literature from various
countries.
(4) WHO should develop
appropriate mechanisms to improve dissemination of information on research
activities. It should assist in updating the available databases on traditional
medicine, preparing a document illustrative of the evidence�based approach to
clinical research in traditional medicine, and forming networks.
(5) WHO should continue to co-ordinate critical data
analysis on traditional remedies.
(6) Relevant governments and
professional agencies should ensure appropriate adverse event reporting and
recording mechanisms are in place.
(7) WHO should support training in research methodologies as
well as in traditional medicine.
(8) WHO and its Member States
should advocate, support and encourage conducting of high quality research.
(9) Research that establishes the
value of traditional medicine in promoting health and wellness beyond treating
diseases should be encouraged.
(10) Clinical trials of widely
used and established traditional remedies should be encouraged and undertaken
prior to obtaining the results of extensive �pre�clinical� basic research.
1. INTRODUCTION
Traditional medicine is the
ancient and culture�bound medical practice which existed in human societies
before the application of modern science to health. The practice of traditional
medicine varies widely, in keeping with the societal and cultural heritage of
different countries. Every human community responds to the challenge of
maintaining health and treating diseases by developing a medical system. Thus,
traditional medicine has been practiced to some degree in all cultures.
After the introduction of modern
medicine into the Region, traditional medicine was usually rejected by the
formal medical service system. Recently, however, attitudes towards traditional
medicine have changed. Traditional medicine is now widely used in the Region
and practiced side by side with modern medicine in most countries. Many
traditional remedies and therapies have transcended their original culture and
become �complementary/alternative� medicine in other countries.
Modern medicine developed very
quickly and made major contributions to disease control in the past century.
Interestingly, despite a rapid growth in knowledge and techniques in modern
medicine, the end of the last century also saw a dramatically increased
interest in traditional medicine. The increasing public demand for its use has
led to considerable interest among policy�makers, health administrators and
medical doctors on the possibilities of bringing traditional and modern
medicine together.
The practice of traditional
medicine is mainly based on conventional use and personal experience. The value
of traditional medicine (as well as many modern medical treatments) has not
been fully tested by using modern scientific means. Extensive accounts of use
and experiences from generation to generation provide
some evidence of the effectiveness of traditional medicine. However, scientific
research is needed to provide additional evidence of its safety and
effectiveness.
To evaluate the role of
traditional medicine in maintaining health, to develop a scientific approach to
policy�making in traditional medicine, and, ultimately, to focus on how
traditional medicine can be harmonized with modern medicine, WHO Regional
Office for the Western Pacific organized the consultation meeting on how to
harmonize the two approaches, from 22 to 26 November 1999 in Beijing, People�s
Republic of China.
1.1 Objectives of the meeting
The objectives of the meeting were to:
(1) review the outcome of recent
scientific research on traditional medicine and to confirm its value in
maintaining health;
(2) identify the scientific basis for evaluating the
efficacy of traditional medicine;
(3) discuss how to promote a dialogue of understanding
between traditional and modern medicine;
(4) identify research
requirements and research priorities for better understanding of the value of
traditional medicine in the Region; and
(5) propose sound research methodologies for objective.
1.2 Participants
The consultation group on the
harmonization of traditional and modern medicine was composed of 24 temporary
advisers, 3 consultants, 1 secretariat staff from the WHO Regional Office for
the Western Pacific and 19 observers.
(back
to content)
3.0 Alternative
Medicine c
Alternative medicine is any practice that aims to achieve
the healing effects of medicine, but which lacks biological plausibility and is
untested, untestable or proven ineffective. Complementary medicine (CM),
complementary and alternative medicine (CAM), integrated medicine or
integrative medicine (IM), and holistic medicine are among many rebrandings
that describe various ways alternative medicine is combined with mainstream
medicine. Alternative therapies share in common that they reside outside of
medical science and instead rely on pseudoscience. Traditional practices become
"alternative" when used outside their original settings without
proper scientific explanation and evidence. Frequently used derogatory
terms for the alternative are new-age or pseudo, with little distinction from
quackery.
AM, complementary and alternative
medicine (CAM), complementary medicine, heterodox medicine, integrative medicine
(IM), complementary and integrative medicine (CIM), new-age medicine,
pseudomedicine, unconventional medicine, unorthodox medicine, altmed
Claims������������������������������������������������������������������������������������
Alternatives to reality-based medical treatments
Some alternative practices are
based on theories that contradict the science of how the human body works;
others resort to the supernatural or superstitious to explain their effect. In
others, the practice is plausibly effective but has too many side effects.
Alternative medicine is distinct from scientific medicine, which employs
the scientific method to test plausible therapies by way of responsible
and ethical clinical trials, producing evidence of either effect or of no
effect. Research into alternative therapies often fails to follow proper research
protocols (such as placebo-controlled trials, blind experiments and calculation
of prior probability), providing invalid results.
Much of the perceived effect of
an alternative practice arises from a belief that it will be effective (the
placebo effect), or from the treated condition resolving on its own (the
natural course of disease). This is further exacerbated by the tendency to turn
to alternative therapies upon the failure of medicine, at which point the condition
will be at its worst and most likely to spontaneously improve.� In the absence of this bias, especially for
diseases that are not expected to get better by themselves such as cancer or
HIV infection, multiple studies have shown significantly worse outcomes
if patients turn to alternative therapies. While this may be because these
patients avoid effective treatment, some alternative therapies are actively
harmful (e.g. cyanide poisoning from amygdalin, or the intentional ingestion of
hydrogen peroxide) or actively interfere with effective treatments.
The alternative sector is a
highly profitable industry with a strong lobby, and faces far less
regulation over the use and marketing of unproven treatments. Its marketing
often advertises the treatments as being "natural" or
"holistic", in comparison to those offered by medical science.
Billions of dollars have been spent studying alternative medicine, with few or
no positive results. Some of the successful practices are only considered alternative
under very specific definitions, such as those which include all
physical activity under the umbrella of "alternative medicine".
DEfiNITIONS AND TERMINOLOGY
The terms alternative medicine,
complementary medicine, integrative medicine, holistic medicine, natural medicine,
unorthodox medicine, fringe medicine, unconventional medicine, and new age
medicine are used interchangeably as having the same meaning and are almost
synonymous in most contexts. Terminology has shifted over time,
reflecting the preferred branding of practitioners. For example, the
United States National Institutes of Health department studying alternative
medicine, currently named the National Center for Complementary and Integrative
Health (NCCIH), was established as the Office of Alternative Medicine
(OAM) and was renamed the National Center for Complementary and Alternative
Medicine (NCCAM) before obtaining its current name. Therapies are often framed
as "natural" or "holistic", implicitly and intentionally
suggesting that conventional medicine is "artificial" and
"narrow in scope".
�Marcia Angell:
"There cannot be two kinds of medicine � conventional and
alternative".
The meaning of the term
"alternative" in the expression "alternative medicine", is
not that it is an effective alternative to medical science, although some
alternative medicine promoters may use the loose terminology to give the appearance
of effectiveness. Loose terminology may also be used to suggest meaning that a
dichotomy exists when it does not, e.g., the use of the expressions
"Western medicine" and "Eastern medicine" to suggest that
the difference is a cultural difference between the Asiatic east and the
European west, rather than that the difference is between evidence-based
medicine and treatments that do not work.
ALTERNATIVE MEDICINE
Alternative medicine is
defined loosely as a set of products, practices, and theories that are
believed or perceived by their users to have the healing effects of medicine,
but whose effectiveness has not been established using scientific methods,
or whose theory and practice is not part of biomedicine, or whose theories or
practices are directly contradicted by scientific evidence or
scientific principles used in biomedicine.
"Biomedicine" or
"medicine" is that part of medical science that applies principles of
biology, physiology, molecular biology, biophysics, and other natural sciences
to clinical practice, using scientific methods to establish the
effectiveness of that practice. Unlike medicine, an alternative product or
practice does not originate from using scientific methods, but may
instead be based on hearsay, religion, tradition, superstition, belief in
supernatural energies, pseudoscience, errors in reasoning, propaganda, fraud,
or other unscientific sources.
Some other definitions seek
to specify alternative medicine in terms of its social and political
marginality to mainstream healthcare. This can refer to the lack of support
that alternative therapies receive from medical scientists regarding access to
research funding, sympathetic coverage in the medical press, or inclusion in the
standard medical curriculum. For example, a widely used definition
devised by the US NCCIH calls it "a group of diverse medical and health
care systems, practices, and products that are not generally considered part of
conventional medicine". However, these descriptive definitions are
inadequate in the present-day when some conventional doctors offer alternative
medical treatments and introductory courses or modules can be offered as part
of standard undergraduate medical training; alternative medicine is taught in
more than half of US medical schools and US health insurers are increasingly
willing to provide reimbursement for alternative therapies.
COMPLEMENTARY OR INTEGRATIVE MEDICINE
Complementary medicine (CM) or
integrative medicine (IM) is when alternative medicine is used together with
mainstream functional medical treatment in a belief that it improves the effect
of treatments. For example, acupuncture (piercing the body with needles to
influence the flow of a supernatural energy) might be believed to
increase the effectiveness or "complement" science-based medicine
when used at the same time. Instead, significant drug interactions caused
by alternative therapies may make treatments less effective, notably in cancer
therapy. Besides the usual issues with alternative medicine, integrative
medicine has been described as an attempt to bring pseudoscience into academic
science-based medicine, leading to the pejorative term "quackademic
medicine". Due to its many names, the field has been criticized for
intense rebranding of what are essentially the same practices.
CAM is an abbreviation of the
phrase complementary and alternative medicine. The 2019 World Health
Organization (WHO) Global Report on Traditional and Complementary Medicine
states that the terms complementary and alternative medicine "refer to a
broad set of health care practices that are not part of that country's own
traditional or conventional medicine and are not fully integrated into the
dominant health care system. They are used interchangeably with traditional medicine
in some countries."
The Integrative Medicine Exam by
the American Board of Physician Specialties includes the following subjects:
Manual Therapies, Biofield Therapies, Acupuncture, Movement Therapies,
Expressive Arts, Traditional Chinese Medicine, Ayurveda, Indigenous Medical
Systems, Homeopathic Medicine, Naturopathic Medicine, Osteopathic Medicine, Chiropractic,
and Functional Medicine.
OTHER TERMS
Traditional medicine refers to
the pre-scientific practices of a certain culture, in contrast to what is
typically practiced in cultures where medical science dominates. The 2019 WHO
report defines traditional medicine as "the sum total of the
knowledge, skill and practices based on the theories, beliefs and experiences
indigenous to different cultures, whether explicable or not, used in the
maintenance of health as well as in the prevention, diagnosis, improvement or
treatment of physical and mental illness."
Holistic medicine is another
rebranding of alternative medicine. In this case, the words balance and holism
are often used alongside complementary or integrative, claiming to take into
account a "whole" person, in contrast to the supposed reductionism of
medicine.
CHALLENGES IN DEfiNING ALTERNATIVE MEDICINE
Prominent members of the science
and biomedical science community say that it is not meaningful to define an
alternative medicine that is separate from a conventional medicine because the
expressions "conventional medicine", "alternative
medicine", "complementary medicine", "integrative medicine",
and "holistic medicine" do not refer to any medicine at all. Others say
that alternative medicine cannot be precisely defined because of the
diversity of theories and practices it includes, and because the boundaries
between alternative and conventional medicine overlap, are porous, and change.
Healthcare practices categorized as alternative may differ in their historical
origin, theoretical basis, diagnostic technique, therapeutic practice and in
their relationship to the medical mainstream. Under a definition of
alternative medicine as "non-mainstream", treatments considered
alternative in one location may be considered conventional in another.
Critics say the expression is
deceptive because it implies there is an effective alternative to science-based
medicine, and that complementary is deceptive because it implies that the
treatment increases the effectiveness of (complements) science-based medicine,
while alternative medicines that have been tested nearly always have no
measurable positive effect compared to a placebo. John Diamond wrote that
"there is really no such thing as alternative medicine, just medicine that
works and medicine that doesn't", a notion later echoed by Paul
Offit: "The truth is there's no such thing as conventional or
alternative or complementary or integrative or holistic medicine. There's only
medicine that works and medicine that doesn't. And the best way to sort it out
is by carefully evaluating scientific studies�not by visiting Internet
chat rooms, reading magazine articles, or talking to friends."
TYPES
Alternative medicine consists of
a wide range of health care practices, products, and therapies. The shared
feature is a claim to heal that is not based on the scientific method.
Alternative medicine practices are diverse in their foundations and
methodologies. Alternative medicine practices may be classified by their
cultural origins or by the types of beliefs upon which they are based. Methods
may incorporate or be based on traditional medicinal practices of a particular
culture, folk knowledge, superstition, spiritual beliefs, belief in
supernatural energies (antiscience), pseudoscience, errors in reasoning,
propaganda, fraud, new or different concepts of health and disease, and any
bases other than being proven by scientific methods. Different cultures
may have their own unique traditional or belief based practices developed
recently or over thousands of years, and specific practices or entire
systems of practices.
UNSCIENTIfiC BELIEF SYSTEMS
Alternative medicine, such as
using naturopathy or homeopathy in place of conventional medicine, is based on
belief systems not grounded in science.
|
|
Proposed
mechanism
|
Issues
|
|
Naturopathy
|
Naturopathic medicine is based on a belief that
the body heals itself
using a supernatural
vital energy
�that
guides bodily
processes.[54]
|
In conflict with
the paradigm of evidence-based medicine. Many naturopaths
have opposed
vaccination, and "scientific evidence
does not support claims that
naturopathic medicine
can cure
cancer or�any other disease".
|
|
Homeopathy
|
A belief that
a substance that causes the symptoms of a disease in healthy people cures similar symptoms in
sick people.[n 8]
|
Developed before knowledge of
atoms and
molecules, or of basic chemistry, which shows that repeated
dilution as practiced in homeopathy
produces only water,
and that homeopathy is not
scientifically valid.[59][60][61][62]
|
"They told me if I took 1000
pills at night I should be quite another thing in the morning", an early
19th-century satire on Morison's Vegetable Pills, an alternative medicine
supplement.
TRADITIONAL ETHNIC SYSTEMS
Ready-to-drink traditional Chinese medicine mixture
Alternative medical systems may
be based on traditional medicine practices, such as traditional Chinese
medicine (TCM), Ayurveda in India, or practices of other cultures around the
world.
Some useful applications of
traditional medicines have been researched and accepted within ordinary
medicine, however the underlying belief systems are seldom scientific and
are not accepted.
Traditional medicine is
considered alternative when it is used outside its home region; or when it is
used together with or instead of known functional treatment; or when it can be
reasonably expected that the patient or practitioner knows or should know that
it will not work � such as knowing that the practice is based on superstition.
|
|
Claims
|
Issues
|
|
Traditional Chinese medicine
|
Traditional practices and beliefs from
China, together with modifications made by the Communist party make
up TCM. Common practices include herbal medicine,
acupuncture (insertion of needles
in the body at specified points),
�massage (Tui na), exercise
(qigong),
and dietary therapy.
|
The practices
are based on belief
in a supernatural energy
�called
�qi, considerations of
Chinese astrology
and
Chinese numerology, traditional use �of herbs and other substances found in China, a
belief that the tongue
contains a map
�of the body that reflects changes
in the body, and an incorrect model
�of the anatomy
and physiology of internal
organs.[63][64][65][66][67][68]
|
|
Ayurveda
|
Traditional medicine of India.
Ayurveda believes in the existence of three
�elemental substances, the
doshas (called
�Vata, Pitta
and Kapha), and states
that a balance of the doshas results in health, while imbalance results in disease. Such disease-inducing imbalances can be adjusted and balanced using traditional herbs, minerals and heavy
metals. Ayurveda stresses
the use
�of
plant-based medicines and treatments,
with some animal products, and added minerals,
including
sulfur,
arsenic,
lead and
copper sulfate.
|
Safety
�concerns have been
�raised about Ayurveda, with
two U.S. studies
finding about 20 percent of Ayurvedic Indian-
manufactured
patent medicines contained toxic levels of heavy metals
such �as
lead,
mercury
�and
arsenic.
A 2015
study �of
users in the United
States also
�found elevated
blood lead levels in 40 percent of those
tested. Other concerns include the use of herbs containing toxic compounds and the lack of quality control
�in Ayurvedic facilities. Incidents of
heavy metal
�poisoning have been attributed to the use
�of these compounds in the United
States.[69][70][71][72][73][74][75][76]
|
�
SUPERNATURAL ENERGIES
Bases of belief may include
belief in existence of supernatural energies undetected by the science of
physics, as in biofields, or in belief in properties of the energies of
physics that are inconsistent with the laws of physics, as in energy medicine.
|
|
Claims
|
Issues
|
|
Biofield therapy
|
Intended to influence energy
�fields
that, it is purported,
surround and penetrate the body.
|
Advocates of
scientific skepticism such
�as
Carl Sagan have described the lack of empirical evidence to
support the existence of the putative
energy
�fields on which these
therapies
are predicated.[77]
|
|
Bioelectromagnetic therapy
|
Use verifiable electromagnetic fields, such
�as pulsed fields, alternating-current,
or direct- current fields in an unconventional
manner.
|
Asserts that magnets can be used to defy
the laws of
physics to influence
health �and
disease.
|
|
Chiropractic
|
Spinal manipulation aims
�to treat "vertebral subluxations" which are
claimed to put pressure on nerves.
|
Chiropractic
was developed in the belief that manipulating the spine
affects the flow of a supernatural vital energy
�and thereby
�affects health
�and disease. Vertebral
�subluxation is a
pseudoscientific concept and has
�not
been �proven to exist.
|
|
Reiki
|
Practitioners place
�their palms on the patient
near
Chakras that they
believe are centers
of supernatural energies in the belief
that these supernatural energies can transfer from the practitioner's palms
to heal the patient.
|
Lacks credible
scientific evidence.
|
|

|
Acupuncture involves insertion of needles in the body.
HERBAL REMEDIES AND OTHER SUBSTANCES
Substance based practices use
substances found in nature such as herbs, foods, non-vitamin supplements and
megavitamins, animal and fungal products, and minerals, including use of these
products in traditional medical practices that may also incorporate other methods.
Examples include healing claims for non-vitamin supplements, fish oil,
Omega-3 fatty acid, glucosamine, echinacea, flaxseed oil, and ginseng.
Herbal medicine, or phytotherapy, includes not just the use� of plant products, but may also� include�
the use� of animal and mineral� products. It is among the most commercially
successful branches of alternative medicine, and includes the tablets, powders
and elixirs that are sold as "nutritional supplements" Only a very
small percentage of these have been shown to have any efficacy, and there is
little regulation as to standards and safety of their contents.
A chiropractor "adjusting" the spine
|
|
Claims
|
Issues
|
|
Christian
faith healing
|
There is a
divine or spiritual intervention
in healing.
|
Lack of evidence for effectiveness. Unwanted outcomes, such as death and disability, "have occurred when faith
healing was elected instead of medical care for serious injuries or illnesses". A 2001 double-blind study
�of
799 discharged coronary surgery patients found that "intercessory prayer had no significant effect on medical outcomes after
�hospitalization in a coronary care
�unit."
|
NCCIH classification
A US agency, National Center on
Complementary and Integrative Health (NCCIH), has created a
classification system for branches of complementary and alternative
medicine that divides them into five major groups. These groups have some
overlap, and distinguish two types of energy medicine: veritable which involves
scientifically observable energy (including magnet therapy, colorpuncture
and light therapy) and putative, which invokes physically undetectable or
unverifiable energy. None of these energies have any evidence to support
that they affect the body in any positive or health promoting way.
1. Whole medical systems: Cut across more than one of the
other groups; examples include traditional Chinese medicine, naturopathy, homeopathy,
and ayurveda.
2. Mind-body interventions: Explore the interconnection
between the mind, body, and spirit, under the premise that they affect
"bodily functions and symptoms". A connection between mind and body
is conventional medical fact, and this classification does not include
therapies with proven function such as cognitive behavioral therapy.
3. "Biology"-based practices: Use substances found
in nature such as herbs, foods, vitamins, and other natural substances. (Note
that as used here, "biology" does not refer to the science of
biology, but is a usage newly coined by NCCIH in the primary source used for this
article.� "Biology-based" as
coined by NCCIH may refer to chemicals from a nonbiological source, such as use
of the poison lead in traditional Chinese medicine, and to other nonbiological
substances.)
4. Manipulative and body-based practices: feature
manipulation or movement of body parts, such as is done in bodywork,
chiropractic, and osteopathic manipulation.
5. Energy medicine: is a domain that deals with putative and
verifiable energy fields:
Biofield therapies are intended to influence
energy fields that are purported to surround and penetrate the body. The
existence of such energy fields have been disproven.
Bioelectromagnetic-based therapies use verifiable
electromagnetic fields, such as pulsed fields, alternating-current,
or direct-current fields in a non-scientific manner.
HISTORY
The history of alternative
medicine may refer to the history of a group of diverse medical practices that
were collectively promoted as "alternative medicine" beginning in the
1970s, to the collection of individual histories of members of that group, or
to the history of western medical practices that were labeled "irregular
practices" by the western medical establishment. It includes the histories
of complementary medicine and of integrative medicine. Before the 1970s,
western practitioners that were not part of the increasingly science-based
medical establishment were referred to "irregular practitioners", and
were dismissed by the medical establishment as unscientific and as
practicing quackery. Until the 1970s, irregular practice became increasingly
marginalized as quackery and fraud, as western medicine increasingly
incorporated scientific methods and discoveries, and had a corresponding
increase in success of its treatments. In the 1970s, irregular practices were
grouped with traditional practices of nonwestern cultures and with other
unproven or disproven practices that were not part of biomedicine, with the
entire group collectively marketed and promoted under the single expression
"alternative medicine".
Use of alternative medicine in
the west began to rise following the counterculture movement of the 1960s, as
part of the rising new age movement of the 1970s. This was due to misleading
mass marketing of "alternative medicine" being an effective
"alternative" to biomedicine, changing social attitudes about not
using chemicals and challenging the establishment and authority of any kind,
sensitivity to giving equal measure to beliefs and practices of other cultures
(cultural relativism), and growing frustration and desperation by patients
about limitations and side effects of science-based medicine. At the same time,
in 1975, the American Medical Association, which played the central role in
fighting quackery in the United States, abolished its quackery committee
and closed down its Department of Investigation.: xxi By the early to mid
1970s the expression "alternative medicine" came into widespread use,
and the expression became mass marketed as a collection of "natural"
and effective treatment "alternatives" to science-based biomedicine.
By 1983, mass marketing of "alternative medicine" was so pervasive
that the British Medical Journal (BMJ) pointed to "an apparently endless
stream of books, articles, and radio and television programmes urge on the
public the virtues of (alternative medicine) treatments ranging from meditation
to drilling a hole in the skull to let in more oxygen".
An analysis of trends in the
criticism of complementary and alternative medicine (CAM) in five
prestigious American medical journals during the period of reorganization
within medicine (1965�1999) was reported as showing that the medical profession
had responded to the growth of CAM in three phases, and that in each phase,
changes in the medical marketplace had influenced the type of response in
the journals. Changes included relaxed medical licensing, the development of
managed care, rising consumerism, and the establishment of the USA Office
of Alternative Medicine (later National Center for Complementary and
Alternative Medicine, currently National Center for Complementary and
Integrative Health).
MEDICAL EDUCATION
Mainly as a result of reforms
following the Flexner Report of 1910 medical education in established medical
schools in the US has generally not included alternative medicine as a teaching
topic. Typically, their teaching is based on current practice and
scientific knowledge about:�
anatomy, physiology, histology, embryology, neuroanatomy, pathology,
pharmacology, microbiology and immunology. Medical schools' teaching includes
such topics as doctor-patient communication, ethics, the art of medicine, and
engaging in complex clinical reasoning (medical decision-making). Writing in
2002, Snyderman and Weil remarked that by the early twentieth century the
Flexner model had helped to create the 20th- century academic health center, in
which education, research, and practice were inseparable.
While this had much improved
medical practice by defining with increasing certainty the
pathophysiological basis of disease, a single-minded focus on the pathophysiological
had diverted much of mainstream American medicine from clinical conditions that
were not well understood in mechanistic terms, and were not effectively treated
by conventional therapies.
By 2001 some form of CAM training
was being offered by at least 75 out of 125 medical schools in the US. Exceptionally,
the School of Medicine of the University of Maryland, Baltimore, includes a
research institute for integrative medicine (a member entity of the Cochrane
Collaboration). Medical schools are responsible for conferring medical degrees,
but a physician typically may not legally practice medicine until licensed by
the local government authority. Licensed physicians in the US who have attended
one of the established medical schools there have usually graduated Doctor of
Medicine (MD). All states require that applicants for MD licensure be graduates
of an approved medical school and complete the United States Medical Licensing
Exam (USMLE).
EFFICACY
There is a general
scientific consensus that alternative therapies lack the requisite
scientific validation, and their effectiveness is either unproved or
disproved. Many of the claims regarding the efficacy of alternative medicines
are controversial, since research on them is frequently of low quality and
methodologically flawed. Selective publication bias, marked differences
in product quality and standardisation, and some companies making
unsubstantiated claims call into question the claims of efficacy of isolated
examples where there is evidence for alternative therapies.
The Scientific� Review of Alternative Medicine points to
confusions in the general population � a person may attribute symptomatic
relief to an otherwise-ineffective therapy just because they are taking
something (the placebo effect);� the
natural recovery� from or the cyclical
nature of an illness� (the regression
fallacy) gets misattributed to an alternative medicine being taken; a person
not diagnosed with science-based medicine may never originally have had a true
illness diagnosed as an alternative disease category.
Edzard Ernst characterized the
evidence for many alternative techniques as weak, nonexistent, or negative and
in 2011 published his estimate that about 7.4% were based on "sound
evidence", although he believes that may be an overestimate. Ernst has concluded
that 95% of the alternative therapies he and his team studied, including
acupuncture, herbal medicine, homeopathy, and reflexology, are
"statistically indistinguishable from placebo treatments", but he
also believes there is something that conventional doctors can usefully learn
from the chiropractors and homeopath: this is the therapeutic value of the
placebo effect, one of the strangest phenomena in medicine.
In 2003, a project funded by the
CDC identified 208 condition-treatment pairs, of which 58% had been studied
by at least one randomized controlled trial (RCT), and 23% had been assessed
with a meta-analysis. According to a 2005 book by a US Institute of Medicine panel,
the number of RCTs focused on CAM has risen dramatically.
As of 2005, the Cochrane Library
had 145 CAM-related Cochrane systematic reviews and 340 non-Cochrane systematic
reviews.� An analysis of the conclusions
of only the 145 Cochrane reviews was done by two readers. In 83% of the cases,
the readers agreed. In the 17% in which they disagreed, a third reader agreed
with one of the initial readers to set a rating. These studies found that, for
CAM, 38.4% concluded positive effect or possibly positive (12.4%), 4.8%
concluded no effect, 0.7% concluded harmful effect, and 56.6% concluded
insufficient evidence. An assessment of conventional treatments found that
41.3% concluded positive or possibly positive effect, 20% concluded no effect,
8.1% concluded net harmful effects, and 21.3% concluded insufficient
evidence. However, the CAM review used the more developed 2004 Cochrane
database, while the conventional review used the initial 1998 Cochrane
database.
Alternative therapies do not
"complement" (improve the effect of, or mitigate the side effects of)
functional medical treatment. Significant drug interactions caused by
alternative therapies may instead negatively impact functional treatment by
making prescription drugs less effective, such as interference by herbal
preparations with warfarin.
In the same way as for
conventional therapies, drugs, and interventions, it can be difficult to
test the efficacy of alternative medicine in clinical trials. In instances
where an established, effective, treatment for a condition is already
available, the Helsinki Declaration states that withholding such treatment is
unethical in most circumstances. Use of standard-of-care treatment in addition
to an alternative technique being tested may produce confounded or
difficult-to-interpret results.
Cancer researcher Andrew J. Vickers has stated:
Contrary to much popular and
scientific writing, many alternative cancer treatments have been
investigated in good-quality clinical trials, and they have been shown to be
ineffective. The label "unproven" is inappropriate for such
therapies; it is time to assert that many alternative cancer therapies have
been "disproven".
PERCEIVED MECHANISM OF EFFECT
Anything classified as
alternative medicine by definition does not have a healing or medical
effect.� However, there are different
mechanisms through which it can be perceived to "work". The common
denominator of these mechanisms is that effects are mis-attributed to the alternative
treatment.
How alternative therapies "work":
|

|
a) Misinterpreted natural course � the individual gets better without
treatment.
b) Placebo effect or false treatment effect � an individual receives
"alternative therapy" and is convinced it will help. The conviction
makes them more likely to get better.
c) Nocebo effect � an individual is convinced that standard treatment
will not work, and that alternative therapies will work. This decreases the
likelihood standard treatment will work, while the placebo effect of the
"alternative" remains.
d) No adverse effects � Standard treatment is replaced with
"alternative" treatment, getting rid of adverse effects, but also
of improvement.
e) Interference � Standard treatment is "complemented" with
something that interferes with its effect. This can both cause worse effect,
but also decreased (or even increased) side effects, which may be interpreted
as "helping". Researchers, such as epidemiologists, clinical
statisticians and pharmacologists, use clinical trials to reveal such
effects, allowing physicians to offer a therapeutic solution best known to
work. "Alternative treatments" often refuse to use trials or make
it deliberately hard to do so.
|
Placebo effect
A placebo is a treatment with no
intended therapeutic value. An example of a placebo is an inert pill, but it
can include more dramatic interventions like sham surgery. The placebo effect
is the concept that patients will perceive an improvement after being treated
with an inert treatment. The opposite of the placebo effect is the nocebo
effect, when patients who expect a treatment to be harmful will perceive
harmful effects after taking it.
Placebos do not have a physical
effect on diseases or improve overall outcomes, but patients may report improvements
in subjective outcomes such as pain and nausea. A 1955 study suggested that a
substantial part of a medicine's impact was due to the placebo effect. However,
reassessments found the study to have flawed methodology. This and other
modern reviews suggest that other factors like natural recovery and reporting
bias should also be considered.
All of these are reasons why
alternative therapies may be credited for improving a patient's condition even
though the objective effect is non-existent, or even harmful. David Gorski
argues that alternative treatments should be treated as a placebo, rather than
as medicine. Almost none have performed significantly better than a placebo
in clinical trials. Furthermore, distrust of conventional medicine may lead to
patients experiencing the nocebo effect when taking effective medication.
REGRESSION TO THE MEAN
A patient who receives an inert
treatment may report improvements afterwards that it did not cause. Assuming it
was the cause without evidence is an example of the regression fallacy. This may
be due to a natural recovery from the illness, or a fluctuation in the
symptoms of a long-term condition. The concept of regression toward the mean
implies that an extreme result is more likely to be followed by a less extreme
result.
OTHER FACTORS
There are also reasons why a
placebo treatment group may outperform a "no-treatment" group in a
test which are not related to a patient's experience. These include patients
reporting more favourable results than they really felt due to politeness or
"experimental subordination", observer bias, and misleading wording
of questions. In their 2010 systematic review of studies into placebos, Asbj�rn
Hr�bjartsson and Peter C. G�tzsche write that "even if there were no true
effect of placebo, one would expect to record differences between placebo and
no- treatment groups due to bias associated with lack of blinding."
Alternative therapies may also be credited for perceived improvement through
decreased use or effect of medical treatment, and therefore either decreased
side effects or nocebo effects towards standard treatment.
USE AND REGULATION
APPEAL
Practitioners of complementary
medicine usually discuss and advise patients as to available alternative
therapies. Patients often express interest in mind-body complementary therapies
because they offer a non-drug approach to treating some health conditions.
In addition to the
social-cultural underpinnings of the popularity of alternative medicine, there are
several psychological issues that are critical to its growth, notably
psychological effects, such as the will to believe, cognitive biases that help
maintain self-esteem and promote harmonious social functioning, and the post
hoc, ergo propter hoc fallacy.
MARKETING
|
�
|
Edzard Ernst, an authority on
scientific study of alternative therapies and diagnoses, and the
first university professor of Complementary and Alternative Medicine. Here
in 2012, promoting his book Trick or Treatment co-written with Simon Singh.
Alternative medicine is a
profitable industry with large media advertising expenditures.
Accordingly, alternative practices are often portrayed positively and compared
favorably to "big pharma".
The popularity of complementary & alternative medicine
(CAM) may be related to other factors that Edzard Ernst mentioned in an
interview in The Independent:
Why is it so popular, then? Ernst
blames the providers, customers and the doctors whose neglect, he says, has
created the opening into which alternative therapists have stepped.
"People are told lies.� There are 40
million websites and 39.9 million tell lies, sometimes outrageous lies. They
mislead cancer patients, who are encouraged not only to pay their last penny
but to be treated with something that shortens their lives."
At the same time, people are gullible. It needs gullibility
for the industry to succeed. It doesn't make me popular with the public, but
it's the truth.
Paul Offit proposed that
"alternative medicine becomes quackery" in four ways: by recommending
against conventional therapies that are helpful, promoting potentially harmful
therapies without adequate warning, draining patients' bank accounts, or by promoting
"magical thinking." Promoting alternative medicine has been called dangerous
and unethical.
Friendly and colorful images of herbal
treatments may look less threatening or dangerous when compared to conventional
medicine. This is an intentional marketing strategy.
SOCIAL FACTORS
Authors have speculated on the
socio-cultural and psychological reasons for the appeal of alternative
medicines among the minority using them in lieu of conventional medicine. There
are several socio-cultural reasons for the interest in these treatments
centered on the low level of scientific literacy among the public at
large and a concomitant increase in antiscientific attitudes and new age
mysticism. Related to this are vigorous marketing of extravagant claims by the
alternative medical community combined with inadequate media scrutiny and
attacks on critics. Alternative medicine is criticized for taking advantage of
the least fortunate members of society.
There is also an increase in
conspiracy theories toward conventional medicine and pharmaceutical companies,
mistrust of traditional authority figures, such as the physician, and a
dislike of the current delivery methods of scientific biomedicine, all of
which have led patients to seek out alternative medicine to treat a variety of
ailments. Many patients lack access to contemporary medicine, due to a lack of
private or public health insurance, which leads them to seek out lower-cost
alternative medicine. Medical doctors are also aggressively marketing
alternative medicine to profit from this market.
Patients can be averse to the
painful, unpleasant, and sometimes-dangerous side effects of biomedical
treatments. Treatments for severe diseases such as cancer and HIV infection
have well-known, significant side-effects. Even low-risk medications such
as antibiotics can have potential to cause life-threatening anaphylactic
reactions in a very few individuals.�
Many medications may cause minor but bothersome symptoms such as cough or
upset stomach. In all of these cases, patients may be seeking out alternative
therapies to avoid the adverse effects of conventional treatments.
PREVALENCE OF USE
According to recent research, the
increasing popularity of the CAM needs to be explained by moral convictions or
lifestyle choices rather than by economic reasoning.
In developing nations, access to
essential medicines is severely restricted by lack of resources and poverty.
Traditional remedies, often closely resembling or forming the basis for
alternative remedies, may comprise primary healthcare or be integrated into the
healthcare system. In Africa, traditional medicine is used for 80% of primary
healthcare, and in developing nations as a whole over one-third of the
population lack access to essential medicines.
In Latin America, inequities
against BIPOC communities keep them tied to their traditional practices and
therefore, it is often these communities that constitute the majority of users
of alternative medicine. Racist attitudes towards certain communities disable
them from accessing more urbanized modes of care.� In a study that assessed access to care in
rural communities of Latin America, it was found that discrimination is a huge
barrier to the ability of citizens to access care; more specifically,
women of Indigenous and African descent, and lower- income families were
especially hurt.� Such exclusion
exacerbates the inequities that minorities in Latin America already face.� Consistently excluded from many systems of
westernized care for socioeconomic and other reasons, low-income communities of
color often turn to traditional medicine for care as it has proved reliable to
them across generations.
Some have proposed adopting a
prize system to reward medical research. However, public funding for research
exists. In the US increasing the funding for research on alternative medicine
is the purpose of the US National Center for Complementary and Alternative
Medicine (NCCAM). NCCAM has spent more than US$2.5 billion on such research
since 1992 and this research has not demonstrated the efficacy of alternative
therapies. The NCCAM's sister organization in the NIC Office of Cancer
Complementary and Alternative Medicine gives grants of around $105 million
every year.� Testing alternative medicine
that has no scientific basis has been called a waste of scarce research
resources.
That alternative medicine has
been on the rise "in countries where Western science and scientific
method generally are accepted as the major foundations for healthcare, and
'evidence- based' practice is the dominant paradigm" was described as an
"enigma" in the Medical Journal of Australia. A 15-year systematic
review published in 2022 on the global acceptance and use of CAM among medical
specialists found the overall acceptance of CAM at 52% and the overall use at
45%.
IN THE UNITED STATES
In the United States, the 1974
Child Abuse Prevention and Treatment Act (CAPTA) required that for states to
receive federal money, they had to grant religious exemptions to child neglect
and abuse laws regarding religion-based healing practices. Thirty-one states
have child-abuse religious exemptions.
The use of alternative medicine
in the US has increased, with a 50 percent increase in expenditures and a 25
percent increase in the use of alternative therapies between 1990 and 1997 in
America. According to a national survey conducted in 2002, "36 percent of
U.S. adults aged 18 years and over use some form of complementary and
alternative medicine." Americans spend many billions on the therapies
annually. Most Americans used CAM to treat and/or prevent musculoskeletal
conditions or other conditions associated with chronic or recurring pain.� In America, women were more likely than men
to use CAM, with the biggest difference in use of mind-body therapies including
prayer specifically for health reasons".� In 2008, more than 37% of American hospitals
offered alternative therapies, up from 27 percent in 2005, and 25% in 2004.
More than 70% of the hospitals offering CAM were in urban areas.
A survey of Americans found that
88 percent thought that "there are some good ways of treating sickness
that medical science does not recognize". Use of magnets was the most
common tool in energy medicine in America, and among users of it, 58 percent
described it as at least "sort of scientific", when it is not
at all scientific. In 2002, at least 60 percent of US medical schools
have at least some class time spent teaching alternative therapies.
"Therapeutic touch" was taught at more than 100 colleges and
universities in 75 countries before the practice was debunked by a
nine-year-old child for a school science project.
PREVALENCE OF USE OF SPECIfiC THERAPIES
The most common CAM therapies used in the US in 2002 were
prayer (45%), herbalism (19%), breathing meditation (12%), meditation (8%),
chiropractic medicine (8%), yoga (5�6%), body work (5%), diet-based therapy
(4%), progressive relaxation (3%), mega-vitamin therapy (3%) and Visualization
(2%)
In Britain, the most often used
alternative therapies were Alexander technique, aromatherapy, Bach and other
flower remedies, body work therapies including massage, Counseling stress
therapies, hypnotherapy, meditation, reflexology, Shiatsu, Ayurvedic
medicine, nutritional medicine, and Yoga. Ayurvedic medicine remedies are
mainly plant based with some use of animal materials. Safety concerns include
the use of herbs containing toxic compounds and the lack of quality control in
Ayurvedic facilities.
According to the National Health
Service (England), the most commonly used complementary and alternative
medicines (CAM) supported by the NHS in the UK are: acupuncture, aromatherapy,
chiropractic, homeopathy, massage, osteopathy and clinical hypnotherapy.
IN PALLIATIVE CARE
Complementary therapies are often
used in palliative care or by practitioners attempting to manage chronic pain
in patients. Integrative medicine is considered more acceptable in the interdisciplinary
approach used in palliative care than in other areas of medicine. "From
its early experiences of care for the dying, palliative care took for granted
the necessity of placing patient values and lifestyle habits at the core of any
design and delivery of quality care at the end of life. If the patient desired
complementary therapies, and as long as such treatments provided additional
support and did not endanger the patient, they were considered acceptable. The
non-pharmacologic interventions of complementary medicine can employ mind-body
interventions designed to "reduce pain and concomitant mood disturbance
and increase quality of life."
REGULATION
Health campaign flyers, as in this example from the
Food and Drug Administration, warn the public about unsafe products.
The alternative medicine lobby
has successfully pushed for alternative therapies to be subject to far less regulation
than conventional medicine. Some professions of complementary/traditional/alternative
medicine, such as chiropractic, have achieved full regulation in North America
and other parts of the world and are regulated in a manner similar to that
governing science-based medicine. In contrast, other approaches may be
partially recognized and others have no regulation at all. In some cases,
promotion of alternative therapies is allowed when there is demonstrably no
effect, only a tradition of use.� Despite
laws making it illegal to market or promote alternative therapies for use in
cancer treatment, many practitioners promote them.
Regulation and licensing of
alternative medicine ranges widely from country to country, and state to state.
In Austria and Germany complementary and alternative medicine is mainly in the
hands of doctors with MDs, and half or more of the American alternative practitioners
are licensed MDs. In Germany herbs are tightly regulated: half are prescribed
by doctors and covered by health insurance.
Government bodies in the US and
elsewhere have published information or guidance about alternative medicine.
The U.S. Food and Drug Administration (FDA), has issued online warnings for
consumers about medication health fraud. This includes a section on Alternative
Medicine Fraud, such as a warning that Ayurvedic products generally have not
been approved by the FDA before marketing.
RISKS AND PROBLEMS
NEGATIVE OUTCOMES
According to the Institute of Medicine, use of alternative
medical techniques may result in several types of harm:
"Economic harm, which results in monetary loss but
presents no health hazard;"
"Indirect harm, which
results in a delay of appropriate treatment, or in unreasonable expectations
that discourage patients and their families from accepting and dealing
effectively with their medical conditions;"
"Direct harm, which results in adverse patient
outcome."
INTERACTIONS WITH CONVENTIONAL PHARMACEUTICALS
Forms of alternative medicine
that are biologically active can be dangerous even when used in conjunction
with conventional medicine. Examples include immuno-augmentation therapy, shark
cartilage, bioresonance therapy, oxygen and ozone therapies, and insulin
potentiation therapy. Some herbal remedies can cause dangerous interactions
with chemotherapy drugs, radiation therapy, or anesthetics during surgery,
among other problems. An example of these dangers was reported by Associate
Professor Alastair MacLennan of Adelaide University, Australia regarding a
patient who almost bled to death on the operating table after neglecting to mention
that she had been taking "natural" potions to "build up her
strength" before the operation, including a powerful anticoagulant that
nearly caused her death.
To ABC Online, MacLennan also gives another possible mechanism:
And lastly there's the cynicism
and disappointment and depression that some patients get from going on from one
alternative medicine to the next, and they find after three months the
placebo effect wears off, and they're disappointed and they move on to the next
one, and they're disappointed and disillusioned, and that can create depression
and make the eventual treatment of the patient with anything effective
difficult, because you may not get compliance, because they've seen the failure
so often in the past.
SIDE-EFFECTS
Conventional treatments are
subjected to testing for undesired side-effects, whereas alternative therapies,
in general, are not subjected to such testing at all. Any treatment � whether
conventional or alternative � that has a biological or psychological effect on
a patient may also have potential to possess dangerous biological or
psychological side-effects. Attempts to refute this fact with regard to alternative
therapies sometimes use the appeal to nature fallacy, i.e., "That which is
natural cannot be harmful." Specific groups of patients such as
patients with impaired hepatic or renal function are more susceptible to side
effects of alternative remedies.
An exception to the normal thinking
regarding side-effects is Homeopathy. Since 1938, the U.S. Food and Drug
Administration (FDA) has regulated homeopathic products in "several
significantly different ways from other drugs." Homeopathic
preparations, termed "remedies", are extremely dilute, often far
beyond the point where a single molecule of the original active (and possibly
toxic) ingredient is likely to remain.�
They are, thus, considered safe on that count, but "their products
are exempt from good manufacturing practice requirements related to expiration
dating and from finished product testing for identity and strength",
and their alcohol concentration may be much higher than allowed in conventional
drugs.
TREATMENT DELAY
Alternative medicine may
discourage people from getting the best possible treatment. Those having
experienced or perceived success with one alternative therapy for a minor
ailment may be convinced of its efficacy and persuaded to extrapolate that
success to some other alternative therapy for a more serious, possibly
life-threatening illness. For this reason, critics argue that therapies that
rely on the placebo effect to define success are very dangerous.
According to mental health journalist Scott Lilienfeld in 2002,
"unvalidated or scientifically unsupported mental health practices can
lead individuals to forgo effective treatments" and refers to this as
opportunity cost. Individuals who spend large amounts of time and money on
ineffective treatments may be left with precious little of either, and may
forfeit the opportunity to obtain treatments that could be more helpful. In
short, even innocuous treatments can indirectly produce negative outcomes.
Between 2001 and 2003, four children died in Australia because their parents
chose ineffective naturopathic, homeopathic, or other alternative medicines and
diets rather than conventional therapies.
Unconventional cancer "cures"
There have always been "many
therapies offered outside of conventional cancer treatment centers and based on
theories not found in biomedicine. These alternative cancer cures have often
been described as 'unproven,' suggesting that appropriate clinical trials have
not been conducted and that the therapeutic value of the treatment is
unknown." However, "many alternative cancer treatments have been
investigated in good-quality clinical trials, and they have been shown to be
ineffective.... The label 'unproven' is inappropriate for such therapies; it is
time to assert that many alternative cancer therapies have been
'disproven'."
Edzard Ernst has stated:
any alternative cancer cure is bogus
by definition. There will never be an alternative cancer cure. Why?
Because if something looked halfway promising, then mainstream oncology would
scrutinize it, and if there is anything to it, it would become mainstream
almost automatically and very quickly. All curative "alternative cancer
cures" are based on false claims, are bogus, and, I would say, even
criminal.
REJECTION OF SCIENCE
There is no alternative medicine. There is only
scientifically proven, evidence-based medicine supported by solid data or
unproven medicine, for which scientific evidence is lacking.
� P.B. Fontanarosa, Journal of the American Medical
Association
(1998)
Complementary and alternative
medicine (CAM) is not as well researched as conventional medicine, which
undergoes intense research before release to the public.� Practitioners of science-based medicine also discard
practices and treatments when they are shown ineffective, while alternative
practitioners do not. Funding for research is also sparse making it
difficult to do further research for effectiveness of CAM. Most funding
for CAM is funded by government agencies. Proposed research for CAM are
rejected by most private funding agencies because the results of research are
not reliable. The research for CAM has to meet certain standards from research
ethics committees, which most CAM researchers find almost impossible to
meet. Even with the little research done on it, CAM has not been proven to be effective.
Studies that have been done will be cited by CAM practitioners in an attempt to
claim a basis in science. These studies tend to have a variety of problems,
such as small samples, various biases, poor research design, lack of controls,
negative results, etc. Even those with positive results can be better explained
as resulting in false positives due to bias and noisy data.
Alternative medicine may lead to
a false understanding of the body and of the process of science. Steven Novella,
a neurologist at Yale School of Medicine, wrote that government-funded studies
of integrating alternative medicine techniques into the mainstream are
"used to lend an appearance of legitimacy to treatments that are not
legitimate." Marcia Angell considered that critics felt that healthcare
practices should be classified based solely on scientific evidence,
and if a treatment had been rigorously tested and found safe and effective,
science-based medicine will adopt it regardless of whether it was considered
"alternative" to begin with. It is possible for a method to change
categories (proven vs. unproven), based on increased knowledge of its
effectiveness or lack thereof. Prominent supporters of this position are George
D. Lundberg, former editor of the Journal of the American Medical Association
(JAMA) and the journal's interim editor-in-chief Phil Fontanarosa.
Writing in 1999 in CA: A Cancer Journal for Clinicians
Barrie R. Cassileth mentioned a 1997 letter to the US Senate Subcommittee on
Public Health and Safety, which had deplored the lack of critical thinking and
scientific rigor in OAM-supported research, had been signed by four Nobel
Laureates and other prominent scientists. (This was supported by the National
Institutes of Health (NIH).)
In March 2009, a staff writer for
the Washington Post reported that the impending national discussion about
broadening access to health care, improving medical practice and saving money was
giving a group of scientists an opening to propose shutting down the National
Center for Complementary and Alternative Medicine.� They quoted one of these scientists, Steven Salzberg,
a genome researcher and computational biologist at the University of Maryland,
as saying "One of our concerns is that NIH is funding pseudoscience."
They noted that the vast majority of studies were based on undamental
misunderstandings of physiology and disease, and had shown little or no effect.
Writers such as Carl Sagan, a
noted astrophysicist, advocate of scientific skepticism and the author of
The Demon-Haunted World: Science as a Candle in the Dark (1996), have lambasted
the lack of empirical evidence to support the existence of the putative energy fields
on which these therapies are predicated.
Sampson has also pointed out that
CAM tolerated contradiction without thorough reason and experiment. Barrett has
pointed out that there is a policy at the NIH of never saying something does
not work, only that a different version or dose might give different results.
Barrett also expressed concern that, just because some "alternatives"
have merit, there is the impression that the rest deserve equal consideration
and respect even though most are worthless, since they are all classified
under the one heading of alternative medicine.
Some critics of alternative medicine
are focused upon health fraud, misinformation, and quackery as public health
problems, notably Wallace Sampson and Paul Kurtz founders of Scientific Review
of Alternative Medicine nd Stephen Barrett, co-founder of The National Council
Against Health Fraud and webmaster of Quackwatch. Grounds for opposing
alternative medicine include that:
It is usually based on religion,
tradition, superstition, belief in supernatural energies, pseudoscience, errorsin
reasoning, propaganda, or fraud.
Alternative therapies typically lack any scientific
validation, and their effectiveness is either unproved or disproved.
Treatments are not part of the conventional, science-based
healthcare system.
Research on alternative medicine is frequently of low
quality and methodologically flawed.
Where alternative therapies have
replaced conventional science-based medicine, even with the safest alternative
medicines, failure to use or delay in using conventional science-based medicine
has caused deaths.
Methods may incorporate or base
themselves on traditional medicine, folk knowledge, spiritual beliefs,
ignorance or misunderstanding of scientific principles, errors in
reasoning, or newly conceived approaches claiming to heal.
Many alternative medical treatments are not patentable,
which may lead to less research funding from the private sector. In addition,
in most countries, alternative therapies (in contrast to pharmaceuticals) can
be marketed without any proof of efficacy � also a disincentive for
manufacturers to fund scientific research.
English evolutionary biologist
Richard Dawkins, in his 2003 book A Devil's Chaplain, defined alternative
medicine as a "set of practices that cannot be tested, refuse to be
tested, or consistently fail tests." Dawkins argued that if a technique is
demonstrated effective in properly performed trials then it ceases to be
alternative and simply becomes medicine.
CAM is also often less regulated than
conventional medicine. There are ethical concerns about whether people who
perform CAM have the proper knowledge to treat patients. CAM is often done by
non-physicians who do not operate with the same medical licensing laws which
govern conventional medicine, and it is often described as an issue of
non-maleficence.
According to two writers, Wallace
Sampson and K. Butler, marketing is part of the training required in
alternative medicine, and propaganda methods in alternative medicine have been
traced back to those used by Hitler and Goebels in their promotion of pseudoscience
in medicine.
In November 2011 Edzard Ernst stated that the "level of
misinformation about alternative medicine has now reached the point where it
has become dangerous and unethical. So far, alternative medicine has remained
an ethics-free zone.� It is time to
change this."
CONflICTS OF INTEREST
Some commentators have said that
special consideration must be given to the issue of conflicts of interest
in alternative medicine. Edzard Ernst has said that most researchers into
alternative medicine are at risk of "unidirectional bias" because of
a generally uncritical belief in their chosen subject. Ernst cites as evidence
the phenomenon whereby 100% of a sample of acupuncture trials originating in
China had positive conclusions. David Gorski contrasts evidence-based medicine,
in which researchers try to disprove hyphotheses, with what he says is the
frequent practice in pseudoscience-based research, of striving to confirm
pre-existing notions. Harriet Hall writes that there is a contrast between the
circumstances of alternative medicine practitioners and disinterested
scientists: in the case of acupuncture, for example, an acupuncturist would
have "a great deal to lose" if acupuncture were rejected by research;
but the disinterested skeptic would not lose anything if its effects were
confirmed; rather their change of mind would enhance their skeptical
credentials.
USE OF HEALTH AND RESEARCH RESOURCES
Research into alternative
therapies has been criticized for "diverting research time, money, and
other resources from more fruitful lines of investigation in order to pursue a
theory that has no basis in biology." Research methods expert and author
of Snake Oil Science, R. Barker Bausell, has stated that "it's become
politically correct to investigate nonsense." A commonly cited statistic
is that the US National Institute of Health had spent $2.5 billion on
investigating alternative therapies prior to 2009, with none being found to be
effective.
GALLERY
|
�
|
Christian laying on of hands, prayer intervention, and faith
healing
|
�
|
Indian Ayurvedic medicine includes a belief that the
spiritual balance of mind influences disease.
�Medicinal herbs in a
traditional Spanish market
�Traditional medicines
in Madagascar
|
�
|
Assorted dried plant and animal parts used in traditional
Chinese medicine
�
Shaman healer in Sonora, Mexico.
�
Phytotherapy (herbal medicine): an engraving of magnolia
glauca in Jacob Bigelow's American Medical Botany
(back
to content)
3.1
Health in Nigeria w
In Nigeria, there has been a
major progress in the improvement of health since 1950. Although lower
respiratory infections, neonatal disorders and HIV/AIDS have ranked the topmost
causes of deaths in Nigeria, in the case of other diseases such as, PID, polio,
malaria and tuberculosis, progress has been achieved. Among other threats to
health are malnutrition, pollution and road traffic accidents. In 2020, Nigeria
had one of the highest cases of COVID-19 in Africa.
�A hospital in Abuja,
Nigeria's capital
The Human Rights Measurement
Initiative finds that Nigeria is fulfilling 48.2% of what it should
be fulfilling for the right to health based on its level of income. When
looking at the right to health with respect to children, Nigeria achieves 66.6%
of what is expected based on its current income. In regards to the right to
health amongst the adult population, the country achieves only 61.7% of what is
expected based on the nation's level of income. Nigeria falls into the
"very bad" category when evaluating the right to reproductive health
because the nation is fulfilling only 16.3% of what the nation is
expected to achieve based on the resources (income) it has available.
LIFE EXPECTANCY AND UNDER-5 MORTALITY RATE
Life expectancy at birth in
Nigeria increased from 49.4 in 2007 to approximately 54 in 2017.� In a decade (2007�2017), U5MR per 1000 live
births drastically reduced from 145.7 to 100.2.�
In comparison with some other reference countries (Ghana, Malawi,
Rwanda, Sudan, Norway, the United States, China and Australia), as shown in the
second Table below, Nigeria with a population of about 195 million has performed
poorly. The country has not done better when compared with the world average
and the World Bank regions namely: East Asia & Pacific Northwest,
Europe & Central Asia, Latin America & the Caribbean, Middle East &
North Africa, South Asia, and Sub-Saharan Africa.
Top 10 causes of most deaths in Nigeria
|
Cause of death
|
IHME rank
2007
|
IHME rank
2017
|
Percentage
change (2017�
2017)
|
|
Malaria
|
1
|
4
|
-35.8
|
|
Diahrrheal
�disease
|
2
|
5
|
-39.5
|
|
HIV/AIDS
|
3
|
3
|
-25.7
|
|
Lower respiratory
infection
|
4
|
1
|
-10.7
|
|
Neonatal disorders
|
5
|
2
|
-1.5
|
|
Tuberculosis
|
6
|
6
|
-15.2
|
|
Meningitis
|
7
|
7
|
-2.0
|
|
Cirrhosis
|
8
|
10
|
1.3
|
|
Ischemic heart
�disease
|
9
|
8
|
24.5
|
|
Stroke
|
10
|
9
|
15.0
|
Source: Institute for Health Metric and Evaluation (IHME)
�
Source: Under-5 Mortality Rate
(per 1,000 live births) and Life expectancy at birth (years). Estimates
developed by the UN Inter-agency Group for Child Mortality Estimation (UNICEF,
WHO, World Bank, UN DESA Population Division)
Comparison of health situations in Nigeria with some
reference countries, regions and the world
|
|
Countries/Regions
|
Life expectancy at birth
(2007)
|
Life expectancy at birth
(2017)
|
U5MR per
1000 �live
births (2017)
|
U5MR per
1000 �live
births (2007)
|
Estimated population (2018)
|
|
Nigeria
|
49
|
54
|
146
|
100
|
195 million+
|
|
Reference countries
|
Ghana (Western
Africa)
|
60
|
63
|
82
|
49
|
29 million+
|
|
Malawi (Southern
Africa)
|
53
|
64
|
103
|
55
|
18 million+
|
|
Rwanda (Eastern
Africa)
|
59
|
67
|
88
|
38
|
13 million+
|
|
Sudan (Northern
Africa)
|
61
|
67
|
84
|
63
|
41 million+
|
|
Norway
|
80
|
83
|
4
|
3
|
5 million+
|
|
United States
|
78
|
79
|
8
|
7
|
327 million+
|
|
China
|
75
|
76
|
20
|
9
|
1.393 billion
|
|
Australia
|
81
|
82
|
5
|
4
|
24 million
|
|
Reference regions
& world
|
East Asia & Pacific
|
74
|
76
|
26
|
16
|
2.328 billion
|
|
Europe & Central
Asia
|
75
|
78
|
15
|
9
|
918 million+
|
|
Latin America &
the Caribbean
|
73
|
76
|
24
|
18
|
641 million+
|
|
Middle East & North Africa
|
72
|
74
|
31
|
23
|
448 million+
|
|
South
�Asia
|
66
|
69
|
71
|
45
|
1.814 billion
|
|
|
|
|
|
|
|
Source: United Nations Population
Division. World Population Prospects: 2017 Revision. The World Bank Group
MATERNAL MORTALITY
�Successful emergency
Caesarean section done in Nigeria.
Maternal mortality rate in
Nigeria is above 800 per 100,000 live births. In 2013, the rate in Nigeria was
560 deaths per 100,000 live births; whereas in 1980, it was 516 deaths 100,000
per live births.� This may be as a result
of poor health facilities, lack of access to quality health care, malnutrition
due to poverty, herder-farmer conflicts, female genital mutilations,
abortions, and displacements due to Boko Haram terrorism in the North East of
Nigeria.� In Nigeria the lifetime risk of
death for pregnant women is 1 in 22. Nigeria's abortion laws make it one of the
most restrictive countries regarding abortion.
A study published in 2019
investigated the competency of emergency obstetric care among health providers
and found it lower than average. Another study shows decrease in maternal
mortality in the southern part of the country while it's still on the increase
in North due to low level of education.
Maternal mortality affects the
socioeconomic development of the country negatively. By 2030, if Nigeria is to
reduce maternal mortality ratio to less than 70 per 100,000 live births (SDG
goal 3 � target 1), all hands must be on deck to achieve it. People can start
by promoting and protecting their own health and the health of those around
them, by making well-informed choices, practising safe sex and attending
antenatal care in government approved health centres. There should be more
awareness in communities about the importance of good health, healthy
lifestyles as well as people's right to quality health care services, especially
for the most vulnerable such as women and children.� Government, local leaders and other decision
makers should be held accountable to their commitments to improve people's
access to health and health care.
WATER SUPPLY AND SANITATION
Access to an improved water source
stagnated at 47% of the population from 1990 to 2006, then increased to 54% in
2010. In urban areas access decreased from 80% to 65% in 2006, and then
recovered to 74% in 2010.
Adequate sanitation is typically
in the form of septic tanks, as there is no central sewage system, except for
in Abuja and some areas of Lagos. A 2006 study estimated that only 1% of Lagos households
were connected to general sewers. In 2016, mortality rate attributed to unsafe
water, unsafe sanitation and lack of hygiene is 68.6 deaths per 100,000
populations.
HIV/AIDS
The Nigeria HIV/AIDS indicator
and impact survey 2018 revealed that the national HIV prevalence rate among adults
ages 15�49 is 1.4 percent. The prevalence of HIV in Nigeria varies widely by
region and states. Akwa Ibom State has the highest prevalence rate of HIV with 5.6
percent and disease burden of 200,051 percentage of deaths and disability-adjusted
life years (DALYs), and followed by Benue State (4.9%, 188,482 DALYs) and
Rivers (3.8%, 196,225 DALYs). The States, Jigawa (12,804 DALYs) and Katsina (26,597
DALYs) both have the lowest prevalence of 0.3 percent. The epidemic is more
concentrated and driven by high-risk behaviors, including having multiple
sexual partners, low risk perceptions, inadequate access to quality health care
services, as well as street/road hawking of goods by itinerant workers
(hawkers) especially, around military and police checkpoints. Other risk
factors that contribute to the spread of HIV, including prostitution, high
prevalence of sexually transmitted infections, clandestine high-risk
homosexual/heterosexual practices, and women trafficking.
Youth and young adults in Nigeria
are particularly vulnerable to HIV, with young women at higher risk than young
men.
MALARIA
Malaria, a disease caused by
mosquitoes has resulted in untold morbidity and mortality in Nigeria. Although,
there has been slight decline in malarial transmission and deaths since 2007 it
ranked the number one cause of deaths in the country, the disease still remains
unflagging.
As of 2012, the malaria prevalence
rate was 11 percent. A part of this data is from the President's Malaria
Initiative which identifies Nigeria as a high-burden country. Nigeria's
branch dealing with this problem, the National Malaria Control Program
recognized the problem and embraced the World Malaria Day theme of "End
Malaria for Good".
In 2017, according to IHME
ranking, malaria ranked the fourth on the causes of most deaths in Nigeria with
U5MR and under-1 child mortality of 103.2 deaths and 62.6 deaths per 1,000 live
births respectively. With pockets of high-level transmission persisting in
states across Nigeria coupled with the never-ending struggle against drug and
insecticide resistance as well as the socio-economic costs associated with a
failure to eradicate the disease, malaria eradication by 2050 seems unachievable.
However, the step to eradicate the disease is a bold attainable goal if
concerted efforts are put in place. The challenge of ineffective management of
malaria prevention and control programs and inadequate use of data to inform
strategies should be addressed. The control of mosquitoes, high quality
diagnosis, and treatment are very necessary if the problem is to be successfully
eradicated. Strong and committed leadership at various levels of government in
Nigeria, reinforced through transparency and independent accountability
mechanisms are very important to ensure a complete eradication of malaria in
the country.
ENDEMIC DISEASES
In 1985, an incidence of yellow
fever devastated a town in Nigeria, leading to the death of 1000 people. In a
span of 5 years, the epidemic grew, with a resulting rise in mortality.� The yellow fever vaccine has been in
existence since the 1930s. There are other endemic diseases in the country
which include malaria, hepatitis A, hepatitis B, typhoid, meningitis and lassa
fever. Travelers are normally advised to get travel vaccines and medicines
because of the risk of these diseases in the country.
FOOD
Nutrition, especially in the north
of the country, is often poor. Since 2002, food staples are supposed to be
fortified with nutrients such as vitamin A, folic acid, zinc, iodine and
iron. Bill Gates, said there had been "pushback" by some in Nigerian
industries as this reduced profit margins. The Bill & Melinda Gates
Foundation is donating $5 million over four years to implement a rigorous
testing regime to make sure these standards are met. These nutrients would
reach poorer children who ate mainly a cereal and beans diet at very low cost
and reduce the risk of stunting. Vitamin A would reduce the risk of death from
measles or diarrhoea. In some districts 7% of children die before they reach
the age of five. Nearly half of these are attributable to malnutrition.
Aliko Dangote, whose companies supply salt, sugar and flour, said there
would need to be a crack down on the import of low-quality foodstuff, often
smuggled into local markets.
POLLUTION
Traffic congestion in Lagos,
environmental pollution: water pollution, and air pollution; and noise
pollution are major health issues.
WATER
The aquatic systems in Nigeria
are reservoirs for toxic chemicals. The activities of oil and gas industries as
well as widespread discharge of effluents into water ways is an eyesore.
Chemical substances such as polyaromatic hydrocarbons, per- and
polyfluoroalkyl substances as well as heavy metals find their way
into oceans, rivers and streams and contaminate them. In 2018, The Nation
newspaper reported improper waste disposal in the country, emphasizing that
there is no proper waste management system, hence the cause of the
indiscriminate dumping of refuse, used polythene bags, plastic bottles and
other liquid and solid wastes in the environment. The Huffingtonpost in
May 2017 raised an alarm on the incessant dumping of plastics in the ocean. It
posited that 'the oceans are drowning in plastics � and no one is paying
attention to the menace'; and by indication, it seems people are overwhelmed by
their own waste. Amidst this, Ellen MacArthur Foundation in Partnership with
the World Economic Forum predicted that by 2050, plastic in the oceans will
outweigh fish. With expected surge in consumption, negative externalities
related to plastics will multiply by that time. Most wastes materials contain
estrogenic chemicals - (estrogens) and androgenic chemicals - (androgens) and they
have potential to leach into the surrounding environment, impact on the
ecosystem and may alter hormonal functions. These contaminants and many other
chemicals are toxic to aquatic lives, most often affecting their life spans and
ability to reproduce; they make their way up the food chain as predator eats
prey and bioaccumulate in the adipose tissues of these organisms.
AIR
Nigeria's air quality is said to
be among the most unsafe globally (ranked 4th) and four of its major cities �
Onitsha, Aba, Kaduna, and Umuahia are among the worst polluted cities in the
world in term of particulate matter of size 10 micrometers and below (PM10).
The most recent report by WHO indicate that the country's annual mean
concentration PM2.5 is 72 μg/m3, far exceeding the recommended maximum of
10 μg/m3. Data from the institutes of Health Metrics and Evaluation on
Global disease burden (GBD) was used to ascertain the cause of death and DALYs
in Nigeria from 2007 � 2017 and published literature where reviewed. According
to World Health data report, most of the highest ranked causes of DALYs are
related to environmental risk factors including chronic respiratory diseases,
cardiovascular diseases, communicable diseases, maternal, neonatal and nutritional
disease, which has cause about 800 thousand deaths and 26 million DALYs per
year in Nigeria. Major environmental risks include indoor air pollution,
ambient air pollution, water, sanitation and hygiene, although there is prolong
and progressive decline in these except ambient PM and ground ozone pollution
which show a steady rise associated with death and DALYs in Nigeria indicating
a significant concern in environment health situation.
Table showing the proportion of
death for each disease attributed to air pollution in Nigeria at 2019 for both
sexes and all ages
|
Disease/disorder
|
Air pollution attributable share of total death in percentages
|
|
Ischemic heart
�disease
|
4.37
|
|
Stroke
|
3.98
|
|
Lung cancer
|
0.39
|
|
Chronic obstructive pulmonary disease
|
0.89
|
Table showing the proportion of DALYs for each disorder
attributed to air pollution in Nigeria at 2019 for both sexes and all ages
|
Disease/disorder
|
Air pollution attributable share of total DALYs in percentages
|
|
Ischemic heart
�disease
|
1,3
|
|
Stroke
|
1.47
|
|
Lung cancer
|
0.13
|
|
Chronic obstructive pulmonary disease
|
0.41
|
CAUSES
Nigeria is home to a lot of
automobiles including cars, motorbikes, heavy duty vehicles like buses, lorries
etc. that are old and has past their best days in term of energy efficiency.
They emit a lot of unhealthy fumes including nitrogen oxides, sulfur oxides,
carbon dioxides, carbon monoxides, particulate matter etc. A large amount of
waste across the country including household and industrial are disposed by
combustion which releases fumes from both organic items, synthetic material
like plastic, rubber as well as from dangerous items like batteries and e-waste
etc. Most households also contribute to emission of noxious smokes and
particulate matters like carbon soot etc. as they rely on inefficiency kerosene
stoves, fire wood and charcoal for cooking and most time this is done
indoor with poor ventilation. Many offices and residences contribute to
increased pollution level of the air with noxious fumes from generators which
are used as substitute to the public epileptic power supply and these fumes are
often released in largely unventilated areas. Other major sources including
emission from factories and industries which release similar fumes like
automobiles but uses mainly diesel in lieu of gasoline Road traffic accidents. Every
year 1.25 million people are killed in a road traffic crashes. Between 20 and
50 million more people suffer non-fatal injuries, with many incurring a
disability. Road traffic injuries cause considerable economic losses to
individuals, their families, and to nations as a whole. These losses arise from
the cost of treatment as well as lost productivity for those killed or disabled
by their injuries, and for family members who need to take time off work or
school to care for the injured. Road traffic crashes cost most countries 3% of
their gross domestic product. Road traffic injuries are the leading cause of
death among people aged between 15 and 29 years.
Over 3 400 people die on the
world's roads every day and tens of millions of people are injured or disabled
every year. Children, pedestrians, cyclists and older people are among the most
vulnerable of road users. WHO works with partners - governmental and
nongovernmental - around the world to raise the profile of the
preventability of road traffic injuries and promote good practice related to
addressing key behaviour risk factors � speed, drink-driving, the use of
motorcycle helmets, seat-belts and child restraints.
With the continued dangerous trend of road traffic collision
in Nigeria, which in 2013 placed it as one of the most road traffic
accident-prone countries worldwide (the most in Africa), the Nigerian
government saw the need to establish the present Federal Road Safety Corps in
1988 to address the carnage on the highways.
LEVEL AND TREND OF ROAD TRAFFIC ACCIDENTS
The Federal Road Safety Corps
(FRSC) says 456 people died and 3404 others were injured in 826 accidents
recorded nationwide in January (2018).
The FRSC stated this in its CCC report for January signed by
its Corps Marshal, Boboye Oyeyemi.
THE UN SUSTAINABLE DEVELOPMENT GOALS
In September 2015, the General Assembly
adopted the 2030 Agenda for Sustainable Development that includes 17
Sustainable Development Goals (SDGs). Building on the principle of
"leaving no one behind", the new Agenda emphasizes a holistic
approach to achieving sustainable development for all. Target 3.6 under
Sustainable Development Goal 3 is designed specifically to addresses the
issue of road traffic accident. It says "By 2020, halve (50% less) the
number of global deaths and injuries from road traffic accidents".
The Federal Government of Nigeria
has put some mechanisms in place to ensure implementation of the SDGs in the
country however, Nigeria is still far from achieving this goal.
TRADITIONAL/ALTERNATIVE MEDICINE
As recent reports have shown, in
addition to the many benefits there are also risks associated with the
different types of Traditional medicine / alternative medicine. Although
consumers today have widespread access to various traditional/alternative
medicine treatments and therapies, they often do not have enough information on
what to check when using them in order to avoid unnecessary harm. While
traditional medicine has a lot to contribute to the health and economy, much
harm has resulted from unregulated sale and misuse of traditional/alternative
medicine and herbs in the country and has significantly delayed patients'
seeking professional healthcare.
CLIMATE CHANGE
In recent times, more attention
has been drawn to the effects of climate change around the world. A lot of
unprecedented changes are being recorded in the weather conditions of different
regions and countries. These have manifested in form of wildfires,
torrential rains and other extreme weather outcomes. It has been pointed out
that the health effects of climate change will increase dramatically over the
next few years and pose a risk to human life and the well-being of billions of
people.
With around 200 million people,
Nigeria is the most populated country in Africa. As the continent's main
exporter of oil, Nigeria faces the challenge of balancing global energy demands
and domestic economic stability with the need to address climate and
environmental challenges. The impact of climate change in Nigeria could include
rising temperatures, more intense and frequent extreme weather events and sea
level rise.� For the population, this
could result in increased water and food insecurity, higher exposure to heat stress
and ultraviolet radiation; changes in infectious and vector-borne disease
transmission patterns; and an increased threat to coastal communities facing
sea level rise.� It is however important
to add that adequate adaptation and mitigation could help to protect the
population, presenting opportunities for actions towards better health outcomes
even in the face of numerous challenges posed by climate change.
The greatest health risk is for
illness to result in mortality.� Climate
change has the potential to exacerbate prevalent diseases as well as emerging
ones like High blood pressure, psychosis, neurosis and congenital
malformations. Climate change creates overwhelming problems for an already
impoverished populace.
�
Health effects of pollution
Flooding is a consequence of climate
change from rise in see level and poor infrastructure, especially with drainage
systems planning and design. For instance, southern Nigeria is highly susceptible
to flooding; particularly Lagos, the commercial hub of the country, which
is said to be one meter above the sea level, is threatened with possible
extinction. The direct health implications of flooding could be deduced
to include direct water borne diseases like typhoid, cholera, pneumonia,
diarrhea and malaria. These, as we will see in the table below are diseases
that already immensely burden the Nigerian populace.
Percentage of Total Deaths and
DALYs of common diseases that can be aggravated by flood
|
|
Percentage of total
deaths
|
Percentage of DALYs
|
|
Malaria
|
12%
|
11.16%
|
|
Typhoid fever
|
0.22%
|
0.24%
|
|
Diarreal diseases
|
11.36%
|
11.86%
|
|
Source:
�institute for Health Metric
and Evaluation
�(IHME 2019)
|
The WHO has identified
Schistosomiasis, African trypanosomiasis, malaria, lymphatic filariasis,
onchocerciasis, and leishmaniasis as "major tropical diseases". This
is in consideration of their public health significance and economic
consequences on afflicted individuals, families and societies. The
devastating effects of these diseases are summarized in the words of Hiroshi
Nakajima, former Director General, WHO: "beyond their toll of individual
illness and death, these tropical diseases have insidious effects on society.
They impede on national and individual development, make fertile land
inhospitable, impair intellectual and physical growth and exact a huge cost in
terms of treatment and control".
Meningitis, measles, chicken pox
and other health risks like high blood pressure and dehydration in pregnancy
are also believed to be amplified by high temperatures. The number of
people in emerging countries is expected to increase by 2.3 billion in 2005 to
4 billion in 2030. This means more carbon emotions due to human activities.
Growing urban sprawls, including poor housing also further compounds the
problem. These changes inevitably increase the peril heat waves in the cities
due to the effects of climate change.
Additionally, high temperature
affects diseases spread and rates of transmission of vector-borne and
rodent-borne diseases. Temperature affects pathogen maturation rate and
mosquito replication, the insect's density in a specific area, and increases
infection likelihood.� Malaria parasites
are recognized to remain sensitive to temperature, particularly throughout the
so-called extrinsic period of incubation for parasite lifecycle, which happens
once the parasite remains alive in the mosquitos. For example, warmer
temperatures promote faster reproductive cycles in mosquitoes that transit
malaria and in the parasite itself.
Although Nigeria has
identified with the rest of the world in acknowledging climate change and
its potential impacts for health and wellbeing, there are still gaps in the
planning and implementation of actions to mitigate these effects. The WHO-
Climate and Health Country Profile for Nigeria (2015), highlights the
successes and shortcomings that characterize the country's climate change response.
These include: identifying a national focal point for climate change in the
Ministry of Health and the development of a national health adaptation
strategy. However, no actions have been implemented towards building
institutional and technical capacities to work on climate change and
health.� Also, Nigeria has climate
information included in its Integrated Disease Surveillance and Response
system, including development of early warning and response systems for climate-sensitive
health risks. Albeit, no activities have been implanted to increase resilience
of health infrastructure. Finally, it is important to note that no
financial commitments (both domestic and international funds) have been made
to implements any action towards health resilience to climate change.
These gaps present opportunities
for actions, the implementation of which has potential to better prepare
Nigeria as a country to mitigate the health risks that climate change poses to
its people. The WHO suggests a comprehensive vulnerability and adaptation assessment
with a focus on health that includes relevant stakeholders from all sectors and
an estimate of the costs to implement health resilience to climate change,
covering infrastructure as well as institutional and technical capacities.
Furthermore, actions need to be taken, that will ensure greening of the health
sector, such as promoting the use of renewable energy, and finally,
conducting a valuation of the co-benefits to health of climate mitigation
policies. This will, among other benefits, help to monitor progress.
(back
to content)
3.2 Healthcare in Nigeria c
Healthcare in Nigeria is a
concurrent responsibility of the three tiers of government in the country. Private
providers of healthcare have a visible role to play in health care delivery.
The use of traditional medicine (TM) and complementary and alternative medicine
(CAM) has increased significantly over the past few years.
Healthcare delivery in Nigeria has
experienced progressive deterioration as a result of weakened political will on
the part of successive governments to effectively solve a number of problems
that have long existed in the sector over many years. This directly impacts the
productivity of citizens and Nigeria's economic growth by extension. Over half
of Nigeria's population live on less than $1.90 a day (�Poverty Head-count�),
making them one of the poorest populations in the world. As of February 2018,
the country was ranked 187 out of 191 countries in the world in assessing the
level of compliance with the Universal Health Coverage (UHC), as very little of
the populace are health insured, whereas even government provision for health is
insignificant. Out-of-pocket payments for health causes households to
incur huge expenditure. Private expenditure on health as a percentage of total
health expenditure is 74.85%.
The implication of this is that
government expenditure for health is only 25.15 percent of all the money spent
on health all across the nation. Of the percentage spent on health by the
citizens (74.85%), about 70% is spent as out-of-pocket expenditure to pay for
access to health services in both government and private facilities. Most of
the remaining money spent by citizens on their health is spent on procuring
�alternatives� which cost a lot. Nigeria has better health personnel than most
other African countries. However, considering its size and population, there
are fewer health workers per unit population than are required to provide
effective health services to the entire nation. Sadly, the most commonly
advertised reason is the brain drain of health professionals to other
countries, especially in Europe and America.
HEALTH INFRASTRUCTURE
The federal government's role is
mostly limited to coordinating the affairs of the university teaching
hospitals, Federal Medical Centres (tertiary healthcare) while the state government
manages the various general hospitals (secondary healthcare) and the local
government focus on dispensaries (primary healthcare), which are regulated by
the federal government through the NPHCDA.
The total expenditure on
healthcare as % of GDP is 4.6, while the percentage of federal government
expenditure on healthcare is about 1.5%. A long run indicator of the ability of
the country to provide food sustenance and avoid malnutrition is the rate of
growth of per capita food production; from 1970 to 1990, the rate for Nigeria
was 0.25%. Though small, the positive rate of per capita may be due to
Nigeria's importation of food products.
HEALTH INSURANCE
Historically, health insurance in
Nigeria could be applied to a few instances: free health care provided and
financed for all citizens, health care provided by government through a
special health insurance scheme for government employees and private
firms entering contracts with private health care providers. However,
there are few people who fall within the three instances; as at 2015 less than
5% of Nigerians have health insurance coverage.
In May 1999, the government
created the National Health Insurance Scheme, encompassing government
employees, the organized private sector and the informal sector. Legislative
wise, the scheme also covers children under five, permanently disabled
persons and prison inmates. In 2004, the administration of President Olusegun
Obasanjo gave more legislative powers to the scheme with positive amendments to
the original 1999 legislative act. 1.5 percent of Nigerians have been covered
by the National Health Insurance Scheme since its establishment. In 2017, the
House of Representatives Committee on Health Care Services in Abuja, organized
a two-day investigative hearing; where the Minister of Health Isaac Folorunsho
Adewole said that the sum of N351 billion had been expended on health
management organizations so far without commensurate result.
There is immense private sector
participation in the scheme with HMOs like Health Partners HMO, Total Health
Trust, Police HMO, Clearline HMO, Multi Shield Nigeria, Expatcare Health
International, Oceanic Health Management and Zuma Health Trust.
BONE MARROW SURGERIES
A new bone marrow donor program,
the second in Africa, opened in 2012. In cooperation with the University of
Nigeria, it collects DNA swabs from people who might want to help a person with
leukemia, lymphoma, or sickle cell disease to find a compatible donor for
a life-saving bone marrow transplant. It hopes to expand to include cord blood
donations in the future.
CANCER CARE
About 80,000 Nigerians die of cancer
annually and over 100,000 are diagnosed with cancer annually. More people are
dying of cancer in Nigeria because cancer and non- communicable diseases are
not given priority in the country's health budget. There are only seven cancer
radiotherapy centres in Nigeria.
Many of the cancer-related deaths
in Nigeria can be attributed to a lack of knowledge regarding this family of
diseases. Furthermore, a lack of education on both prevention and early detection
and a culture which endorses silence and places a negative social stigma on
such illnesses has led to more than one-third of preventable cancer deaths.
MENTAL HEALTH
The majority of mental health
services is provided by 8 regional psychiatric centers and psychiatric
departments and medical schools of 12 major universities. A few general
hospitals also provide mental health services. The formal centres often face competition
from native herbalists and faith healing centres.
The ratio of psychologists and social workers is 0.02 to
100,000.
ISSUES
REGULATION OF PHARMACEUTICALS
In 1989 legislation made
effective a list of essential drugs. The regulation was also meant to limit the
manufacture and import of fake or sub-standard drugs and to curtail false advertising.
However, the section on essential drugs was later amended. In 2005 it was
estimated that about 16.7% of pharmaceutical drugs in the country were
counterfeit. in 2012 a new study concluded that the proportion had fallen to
6.4%, of which 19.6% were Anti-Malaria medicines. In 2014 that had fallen to
3.6%. About N29 billion worth of counterfeit drugs were destroyed between 2015
� 2017.
Drug quality is primarily
controlled by the National Agency for Food and Drug Administration and Control.
The agency has established a Mobile Authentication Service. A team of girls
from the Regina Pacis Secondary School in Onitsha devised a better
technological solution, an app called the FD Detector which uses barcode
technology to verify drug authenticity and expiration dates.
This won them a place in the Technovation Challenge 2018.
Several major regulatory failures have produced
international scandals:
In 1993, adulterated paracetamol
syrup entered into the healthcare system in Oyo and Benue State, the result of was
the death of 100 children. A year after the disaster, batches containing
poisonous ethylene glycol, the major cause of the deaths, could still be
purchased.
In 1996, about 11 children died of contamination from an experimental
trial of the drug trovafloxacin.
In 2008�2009, at least 84 children died from a brand of
contaminated teething medication.
GEOGRAPHIC INEQUALITY
|
�
|
Malian Fulani immigrant selling herbal medicines in a
Nigerian market
Healthcare in Nigeria is influenced
by different local and regional factors that impact the quality or quantity present
in one location. Due to the aforementioned, the healthcare system in Nigeria
has shown spatial variation in terms of availability and quality of facilities
in relation to need. However, this is largely as a result of the level of state
and local government involvement and investment in health care programs and
education. Also, the Nigerian ministry of health usually spend about 70% of its
budget in urban areas where around 50% of the population resides.
EMIGRATION OF HEALTHCARE WORKERS
|
�
|
Retaining health care professionals is an important
objective
Survey shows looming brain drain in Nigeria's health sector in the
rising trend of emigration of healthcare personnel � physicians, pharmacists,
nurses, and laboratory scientists, physiotherapists and many others have
difficulty getting into paid employment. Many fresh doctors, out of
medical schools, and managed to get housemanship positions, the situation occurs
every year. The problem persists beyond the period of housemanship or
internship, when it comes to securing a well deserved employment. There are
generally not enough job positions to go round.�
The challenge of this is clear. The problem of skewed distribution, with
the few available personnel being mostly concentrated in the urban areas, where
almost all the large facilities like General Hospitals and Teaching Hospitals
are located. The underneath issues for this may include the political
dimension, with some states unwilling to recruit large numbers of workers from
other parts of the country as an act of deliberate policy, preferring to employ
their own indigenes, or, where there is a short-fall, employ foreigners mostly from
North Africa on short-term contracts. In 2007, a National Human Resources for
Health Policy was formulated by the Federal Ministry of Health and approved by
the National Council on Health. Subsequently, a Human Resource for Health
Strategic Plan 2008�2012 was drawn up to guide implementation of the policy at
all levels. The ultimate aim was to ensure that adequate numbers of skilled and
well-motivated health workers were available and equitably distributed through
the nation in order to ensure provision of quality health services. The situation
appears set to get worse. As the era of Sustainable Development Goals is
commenced and the target of 2030 begins to come into focus, the statistics are
far from providing reassurance.
There are 4000 Nigeria doctors
practicing in the United States and 8000 practicing in the United Kingdom.
Retaining these expensively trained professionals has been identified as
an urgent goal. The brain drain cut across all healthcare professionals;
thousands of Nigerian pharmacists and nurses are practicing in the UK and USA
as well and so on.
PRIVATIZATION AND COMMERCIALIZATION OF PUBLIC HEALTH SERVICE
The public health services in
Nigeria is of poor quality and it is not adequately available, accessible, and
affordable to many people who need these services. The search for solutions has
led to the idea of privatization and commercialisation of public health services.
This development is greatly favoured by the idea that it will increase
competition and result in the lowering of unit price of health services and
make such services more affordable to the poor. However, the argument against
it is that privatization and commercialization in Nigeria will be a mirage
unless institutional reforms take place.
TRADITIONAL AND ALTERNATIVE MEDICINE
As recent reports have shown, in
addition to the many benefits there are also risks associated with the
different types of traditional medicine /complementary or alternative medicine.
Although consumers today have widespread access to various TM/CAM treatments
and therapies, they often do not have enough information on what to check when
using TM/CAM in order to avoid unnecessary harm. While traditional medicine has
a lot to contribute to the health and economy, much harm has resulted from
unregulated sale and misuse of traditional/alternative medicine and herbs in
the country and has significantly delayed patients' seeking professional
healthcare.
(back to content)
4.0 TRADITIONAL AND MODERN MEDICINE:
HARMONIZING THE TWO APPROACHES i
2. PROCEEDINGS
2.1 Opening
ceremony
Dr. Shigeru Omi, WHO Regional
Director for the Western Pacific, opened the meeting with the emphasis on WHO�s
commitment to foster a better understanding of traditional medicine.
He reported on the high usage
rate of traditional medicine in the Region and the increasing interest in
traditional medicine from Member States during recent years. He indicated that
WHO supported the efforts to bring traditional medicine into mainstream general
health service. However, WHO could only endorse therapies supported by solid
scientific evidence. Dr. Omi reminded the participants that they were facing
many threats to human health and the outcomes of the meeting would lay the
foundation for traditional and modern medicine to work together to meet ever increasing
challenges of the new century.
Dr. Zhu Qing�shen, Vice�Minister
of Health and Director�General of State Administration of Traditional Chinese
Medicine (SATCM), of People�s Republic of China, welcomed the attendees and
described the important role traditional medicine plays in maintaining the
health of the people of China.
Dr. Margaret Chan, Director of Health of Hong Kong, China;
Dr. P.Y. Lam, Deputy Director of
Health and several staff from Department of Health, Hong Kong, China; a
delegate from Georgia;
Professor Zheng Shou�Zhan,
President of Beijing University of Traditional Medicine, and some senior staff
from the State Administration of Traditional Chinese Medicine also attended the
opening ceremony.
Dr. S. Omi�s speech is attached as Annex 2.
2.2 Purpose of the meeting, procedures and outcomes
Dr. Chen Ken, Medical Officer of
Traditional Medicine, WHO Regional Office for the Western Pacific and
responsible officer for the meeting, gave a brief introduction to the
objectives, process, and proposed methods of work of the workshop.
The purpose of this meeting was to:
� review previous scientific research on traditional medicine;
� discuss appropriate evidence for better acceptance of traditional
medicine; and
� identify research requirements, research priorities and appropriate
research methods which could be adopted for creating additional evidence on the
usefulness of traditional medicine.
It is expected that the
conclusions and recommendations of the consultation meeting will be followed up
by WHO and its Member States to ensure the proper use of traditional medicine
by harmonizing traditional and modern medicine.
2.3 Presentations
Papers on specific themes
relevant to the conference were prepared by the consultants, temporary advisers
and the secretariat and were distributed among all participants. The
consultation group agreed to receive verbal summaries of these papers during
the plenary session. Twenty verbal presentations were made by the authors of
the papers and the topics included:
� WHO�s involvement in traditional medicine;
� acupuncture � research on its mechanisms;
� acupuncture � clinical trials and clinical effectiveness;
� medicinal plants and herbal medicines � experimental
research;
� quality of medicinal plants;
� clinical trials in herbal medicine;
� evidence�based health care practice;
� issues of evidence in traditional medicine;
� Growth of traditional medicine; and
� Clinical research methodologies.
These papers and presentations
provided background material for subsequent discussions by sub�groups.
2.4 Group activities
The consultation group was
divided into five sub�groups with each group focusing on one of the following:
clinical research in acupuncture, clinical research in herbalism, basic science
research in acupuncture, basic science research in herbalism, and
socio�economic factors involved in harmonizing traditional and modern medicine.
Following two days of small group discussions, the two sub�groups discussing
herbal research were merged into one, and the two sub�groups discussing
acupuncture research were merged into one on the final day of group
discussions.
3. TRADITIONAL MEDICINE
3.1 Background and characteristics
Traditional medicine is the
ancient and culture�bound medical practice which existed before the application
of modern science to health. The practice of traditional medicine varies
widely, in keeping with the societal and cultural heritage of different
countries. Every human community has responded to the challenge of maintaining
health and treating diseases by developing a medical system. Thus, traditional
medicine has been practiced to some degree in all cultures.
A workshop on development of
national policy on traditional medicine organized by WHO Regional Office for
the Western Pacific in October 1999 defined traditional medicine as the sum
total of knowledge, skills and practices of holistic healthcare, which is
recognized and accepted by the community for its role in the maintenance of
health and the treatment of diseases. Traditional medicine, based on the
theory, beliefs and experiences indigenous to different cultures, was developed
and handed down from generation to generation.
In some countries, remedies used by traditional medicine
have re�emerged. Such techniques are usually known as �alternative� or
�complementary� medicine, which as a form of medicine has evolved recently as a
reaction to high technology medicine.
A traditional medicine
practitioner is a person who is recognized by the community where he or she
lives as someone competent to provide health care by using plant, animal and
mineral substances and other methods based on social, cultural and religious
practices.
Traditional medicine
practitioners are also recognized as experts on community attitudes and beliefs
related to physical, mental and social well�being and the causes of disease and
disability. Traditional medicine practitioners include traditional healers,
traditional birth attendants, herbalists and bone�setters.
There are many traditional
systems of medicine. However, many traditional systems of medicine have some
common characteristics.
� Traditional medicine is based
on a belief that health is a state of balance between several opposing aspects
in the human body. Illness occurs when an individual falls out of balance,
physically or mentally. The �causes� of imbalance could be change of weather,
intake of certain food; external factors, such as magical or supernatural
powers; mental stimulation and societal reasons.
Traditional medicine tries to restore the balance using
different therapies.
� Traditional medicine is based
on the needs of individuals. Different people may receive different treatments
even if they suffer from the same disease.
Traditional medicine is based on
a belief that each individual has his or her own constitution and social
circumstances which result in different reactions to �causes of disease� and
treatment.
� Traditional medicine applies a
holistic approach. It considers a person in his or her totality within an
ecological context and usually will not only look after the sick part of the
body. Besides giving treatment, traditional practitioners usually provide
advice on lifestyles and healthy behaviour.
� Traditional medicine precedes
modern medicine. Most traditional remedies have not been evaluated by sound
scientific methods. This means that, at this stage, traditional medicine is not
easily understood by modern medicine. However, traditional remedies have been �field�tested�
by tens of thousands of people for hundreds of years.
� Traditional medicine covers a wide scope and its practices
vary widely from country to country. In the Region, the main therapeutic
techniques are medicinal plants and acupuncture.
3.2 Changes in trends of usage
Traditional medicine exists in
most countries and areas in the Western Pacific Region and makes a significant
contribution to the health of the people of the Region. Interest in traditional
medicine has increased over the last decade and seems likely to continue.
People now are more prepared to look for alternative
approaches to maintain their health.
There are no solid data on the
extent of usage of traditional medicine in the Region. However, data from
several countries and areas in the Region show that around 40% to 60% of the
population of these countries and areas use traditional medicine. For example,
traditional medicine accounts for around 40% of all health care delivered in
China and in Hong Kong, approximately 60% of the population has consulted
traditional medicine practitioners at one time or another.
The use of
traditional/complementary medicine in industrialized countries has increased
significantly. Studies conducted in the US show that complementary therapy
usage increased from 34% in 1990 to 42% in 1997.4 In Australia, research has
indicated that 48.5% of the population used at least one non�medically
prescribed alternative medicine in 1993. The estimated national expenditure on
alternative medicines and alternative practitioners is close to A$1 000 million
per annum, of which A$621 million is spent on alternative medicines.
An Australian government report
in 1996 estimated that there were at least 2.8 million traditional Chinese
medicine consultations in 1996, representing an annual turnover of A$84 million
within the health economy. This growth was also reflected in a four�fold
increase in the importation of Chinese herbal medicines since 1992.
Clearly, traditional medicine is
widely used by the public, and in some countries its use has increased
dramatically. Increased demands from public lead to increased interest and
involvement of the academic and scientific community. Concurrently, more and
more governments from countries and areas within the Region have shown their
interest and willingness to promote the proper use of traditional medicine.
3.3 Consumers, government and other stakeholders
Based on the growing interest in
traditional medicine shown by consumers, scientists and regulators, three
important challenges present themselves.
� The public and the users of
traditional medicine request safe, quality�controlled and effective remedies.
� Medical scientists request more
scientifically sound evidence before comfortably accepting many traditional
medicine practices. Many health professionals have doubts about the usefulness
of traditional medicine. In many cases, they require more scientifically�based
evidence if they are to trust its safety and effectiveness.
Meanwhile, the involvement of the
academic and scientific community provides the opportunity to create more
evidence by means of modern science.
� Governments need to establish
and update mechanisms for the regulation of traditional medicine and its
practitioners and, in doing so, require more scientifically�based evidence to
support decision�making. As traditional systems of medicine become better
documented, and more scientifically credible, usage is only likely to increase
further.
Consumers, of course, have many
different reasons for using traditional medicine, and may not require the same
level of evidence of practice that is espoused by medical scientists. Consumers
may have confidence in, for example, oriental herbal medicine because of its
existence in public hospitals and medical infrastructure in China, Republic of
Korea, and Japan, instituted by centuries of use, scholarly writings and a
formal tertiary education system.
Consumers may also be prepared to
try an herbal formula that has been used and documented in classical medical
literature for many centuries and may be less convinced by a clinical trial of
a new drug � having been applied only to a well�defined sample group.
Consumers� awareness of these
factors may generate more confidence in terms of �evidence behind practice�
than any single methodologically rigorous clinical trial. However, to the
scientist it�s the latter, and not the former, that represents the stronger
evidence.
4. TRADITIONAL MEDICINE AND MODERN MEDICINE
Traditional and modern systems of
medicine were developed by different philosophies in different cultural
backgrounds. They look at health, diseases and causes of diseases in different
ways. These differences bring different approaches to health and diseases.
However, both systems deal with the same subject � human
being.
The old and modern arts of healing should exist together.
4.1 Integration of traditional medicine with modern medicine
The integration of traditional medicine with modern medicine
may have three different meanings.
First, it may mean incorporation
of traditional medicine into the general health service system. The government
recognizes the practice of traditional medicine and the use of traditional
medicine is incorporated into the mainstream of health service system. In the
Region, traditional medicine has been an integral part of formal health service
system in several countries, albeit in different forms.
Second, it may mean integration
of the practice of traditional medicine with that of modern medicine. In fact,
many medical doctors who have adequate knowledge of traditional medicine have
tried to incorporate remedies used by traditional medicine into their daily
work. In some places, traditional and modern medicines are practiced side by
side. Studies have also shown that many patients use both traditional and
modern medicine.
Third, it may mean the
integration of traditional and modern medicine as two branches of medical
science. Although traditional and modern medicines have developed in different
cultural contexts and are at different stages of scientific development, they
have many similarities. Efforts have been made to synthesize the two branches,
in order to form a new branch of medical science, incorporating elements of
both. However, at this stage this would appear to be a difficult task.
4.2 The need for harmonization of traditional and modern
medicine.
Increased cross�cultural
communication has resulted in the exposure of many indigenous forms of
traditional medicine to new, more modern, medical environments. Various
responses may and have occurred to the presence of differing approaches to
health care.
These range from complete
rejection of TM by modern medical practitioners and of modern medicine by TM
practitioners, to a parallel existence with little communication over patient
care, or to ultimately forced understanding, subsuming and integration of one
model by the other. None of these approaches is ideal precisely because none
confers adequate respect on the practices of the other.
This results in a weak
utilization and exploration of the benefits presented by each model.
Harmonization of traditional and modern medicine emphasizes the importance of
respectful co�existence. Within the model of harmonization, there is the
requirement to develop and hold a good understanding of the other approaches to
health care. Modern medicine practitioners and researchers are required to
achieve adequate education and awareness of the practice, principles and
context of traditional medicine. Similarly, TM practitioners need to be
significantly more aware of the nature of practice and strengths of modern
medical approaches. The purpose of this broader education base is not simply to
yield a better understanding of differing practices, but primarily to promote
the best care for patients by intelligently selecting the most facilitating
route to health and wellness.
Surveys and other sources of
evidence indicate that traditional medical practices are frequently utilized in
the management of chronic diseases. It is particularly for this category of
illness that TM has developed a reputation. It is also in this area of
treatment that modern medicine is considered the weaker. An approach to
harmonizing activities between modern and traditional medicine will promote a
clearer understanding of the strengths and weaknesses of each, and encourage
the provision of the best therapeutic option for patients.
The alternative to this is poor
health care practice and bad medicine, most especially as the quantifiable
scientific evidence of effective TM practices mounts.
Collecting evidence based on
research is, therefore, regarded an essential step, although, of course, much
more is involved in harmonization.
5. EVIDENCE AND TRADITIONAL MEDICINE
5.1 Acquisition of traditional medical knowledge
�In order to evaluate the
efficacy of ginseng, find two people and let one eat ginseng and run, and the
other run without eating ginseng. The one that did not eat ginseng will develop
shortness of breath sooner.� Bencao Tujing, Atlas of Materia Medica, 1061AD.
Traditional medicine
practitioners have developed unique methods of diagnosis and treatment that are
specific to their particular cultures. Some of these approaches based on
complex theoretical frameworks can be traced back as far as 3 500 years.
Although there is evidence from
the Song dynasty in China that comparative trials were used to illustrate
treatment effects, they were not applied in a rigorous systematic manner to
advance the state of knowledge. For the most part, it was assumed that
knowledge of traditional medicine was reinforced through clinical experience
and transferred either verbally or by cataloguing accumulated experience in
reference texts.
Clinical experience is an excellent way to learn about
medicine.
However, development of new
medical knowledge relies on treatment safety, costs, and systematic research.
Given today�s interest in traditional and complementary medicine, information
on safety, efficacy and costs is being requested by patients, governments,
traditional practitioners and practitioners of modern medicine.
5.2. Evidence�based health care practice
The practice of evidence�based medicine
(EBM) involves �the conscientious, explicit, and judicious use of current best
evidence in making decisions about the care of individual patients.� When it
was originally proposed in 1992, EBM was defined as a new paradigm for medical
practice: �Evidence�based medicine de-emphasizes intuition, unsystematic
clinical experience and pathophysiologic rationale as sufficient grounds for
clinical decision making and stresses the examination of evidence from clinical
research.�
Although evidence�based medicine
emphasizes the use of the randomized controlled trial (RCT) for the evaluation
of therapeutic effectiveness whenever possible, the practice of EBM does not
rely exclusively on the randomized controlled trial. Evidence to support
clinical practice can come from any number of systematic research designs;
however, these different types of research designs do not all lead to the same
level of evidence. The rules of EBM privilege certain kinds of evidence as
having more weight. The latest levels of evidence provided by the Cochrane
collaboration include:
Level I: Strong evidence from at least one systematic review
of well�designed RCTs.
Level II: Strong evidence from at least one RCT.
Level III: Well�designed trials without randomization.
Level IV: Non�experimental evidence.
Level V: Expert opinion.
Level VI: Someone told me.
There are several other ways to level the evidence proposed
by different institutions.
EBM is the use of best evidence
integrated with individual clinical expertise in making a medical decision. One
cannot stand without the other. Without the clinical expertise, external
evidence might not be applied appropriately to individual patients. Without the
use of evidence, clinical expertise alone might be biased and out�of�date. In
clinical guideline development process, actual recommendations come from
different levels of evidence. Strong recommendations come from strong evidence
(i.e. from well-designed randomized controlled trials). However, in most
situations when there is a lack of good evidence, the panel usually considers
other factors such as cost, availability of health personnel, laboratory and
medical interventions, practical considerations, target population, etc. to
decide on the best recommendations. Therefore, the role of traditional medicine
in areas where western medicine is not readily available or affordable has to
be emphasized. Even if there might be a lack of good evidence (and this is also
true of western medicine), use of traditional medicine interventions might
still be part of most clinical practice guideline recommendations.
The following methodology is
proposed for creating evidence based recommendations (EBRs). This framework
provides a series of validated steps to ensure the development and acceptance
of objective, users�friendly, evidence�based recommendations for clinical
practice.
The six�steps to EBR development are described below.
Step 1: Project definition and team formation:
� specification of questions to be addressed and selection
of team,
� focused questions on the management of a specific disease
or condition;
Step 2: Perform a formal literature search:
� electronic search, where possible,
� retrieval of local publications, including translation of
primary sources by persons trained in traditional medicine and clinical
epidemiology;
Step 3: Create systematic overviews:
� evaluation of literature discovered, based on objective
criteria;
Step 4: Estimate expected benefits, harms and costs:
� evaluation of important sources of information from
observational and historical databases which may reveal important information
with respect to toxicity, costs and culturally�based patient preferences;
Step 5: Judge relative value of expected benefits, harms and
costs:
� relative importance of benefits and harms to the patient
and payer; and Step 6: Develop EBRs based on levels of evidence.
Evidence�based medicine is not a
methodological research framework; it is a research transfer framework.
Although evidence-based medicine de�emphasizes the sharing of unsystematic
clinical experience, it does not invalidate clinical experience as a method of
gaining knowledge. Using the EBM framework, however, a clinician can transfer
his or her knowledge to other practitioners; the knowledge must be presented in
a transparent fashion so that the recipient can appraise the knowledge to
determine the level of evidence it represents.
6. EVIDENCE OF PRACTICE IN TRADITIONAL MEDICINE
These notes reflect consensus
views developed in groups in response to papers submitted to the meeting. The
groups consisted of representatives from various Member States with backgrounds
in both traditional medicine and modern medicine.
6.1 Basic science research in acupuncture
The group recognized that
although acupuncture research initially concentrated on analgesia and
neurological models, recently it had broadened to other areas of physiological
systems including endocrine, immunological and metabolic.
Two perspectives could be discerned in the research:
� traditional theory and clinical
evidence is used to provide the basis for modern experiments in
neurophysiology, and
� basic scientists are attempting
to describe traditional ideas of meridians, point location, etc. in scientific
terms.
The principal areas of this
research were described in papers by Professors Cao Xiaoding, Kyuya Kogure and
Liu Jungling. The group recognized, however, that much of the important
original scientific work on acupuncture was not yet available in English.
Most of the research work on
mechanisms of action was carried out on acute pain management, and it was not
clear whether this was relevant to effects of acupuncture on chronic pain,
which may have different underlying mechanisms, nor whether similar mechanisms could
be applied to other therapeutic applications of acupuncture. The issue
underscored the importance of integrating clinical science and basic research
in future acupuncture studies.
6.2 Clinical research on acupuncture
The starting point of the group�s
discussion centred on the awareness of the enormous historical and cultural
significance of traditional acupuncture, as well as the importance of clinical
experience and observation in this area. However, the focus of discussion was
on the modern methods of treatment evaluation.
A number of English language
reports of clinical trials are available.11,12 In the last few years,
activities of the Cochrane Centre for Systematic Reviews have been extended to
include reviews of complementary/traditional medicine. Reviews of the clinical
trial literature on acupuncture for low back pain, asthma, nausea and vomiting
and smoking cessation are also available. Reviews are in progress for the
acupuncture treatment of chronic headache.
The findings from all these
reviews are similar, in that clinical trials have been too few, too small, and
inadequately controlled.
There have been doubts about the
adequacy of treatment, problems with the definition of placebos and a variety
of other methodological problems. Overall, methodological details have been
lacking in many study reports. While progress has been made in defining an
appropriate methodology for acupuncture evaluation, this has not yet translated
into trials of a high standard that can provide definitive results. Hence, the
results from most reviews are fundamentally inconclusive. Clearly, if research
is to be continued, much larger trials of considerably better quality need to
be conducted. Most of research literature remains in Chinese, and, therefore,
not easily accessible to those carrying out the systematic reviews. Conversely,
the English language studies and reviews are not easily accessed within China.
The conclusions reached from the
clinical trial perspective contrast strongly with those reached by clinicians and
researchers working from within a traditional medicine framework. From within
traditional medicine, the result of literally hundreds of years of clinical
experience, and thousands of case series suggest that acupuncture can be
effective for a wide range of clinical conditions.
The modern clinical trial and the
traditional medicine perspectives can be usefully encompassed with the
evidence-based medicine framework described above. There is a need to
acknowledge the evidence base within traditional medicine, while also
recognizing the importance of clarifying the extent and limitations of
traditional practice through methodologically sound research. However, the
design of studies needs to incorporate traditional medicine perspectives,
including differences in diagnostic approaches that guide treatment.
6.3. Basic science research in herbal medicine
A wealth of information exists in
the literature regarding plants and plant formulas used in traditional
medicine. The Western Pacific Region is a particularly rich source of such
information. Historical data has also been the starting point for basic science
research that has led to the discovery of active components. Using highly
advanced research techniques a number of compounds have been discovered over
the years and successfully brought into clinical use.
The collection of data on herbal
use is an ongoing process. In China, over 100 000 herbal preparations have been
recorded that are still in clinical use. Researchers in Fiji, Malaysia, Samoa
and Tonga have recently published monographs on medicinal plants with
information on taxonomy, traditional use, chemical constituents, etc.
Also, an extensive Korean
database exists of over 12,000 prescription titles with respective formulas,
12,000 natural constituents with drawings of chemical structure and analytical
data, photo images of standard herbal materials and original medicinal whole
plants with taxonomical verification and a dictionary of disease classification
in terms of TCM and modern medicine. All participants voiced the need for a
comprehensive regional database that would allow easy access and exchange of
information.
Quality control of herbal
products will have a significant impact on the overall effectiveness of herbal
medicines. To this end, China has introduced new legislation requiring approval
for new raw materials and traditional herbal formulas to be classified as
drugs.
New drug approvals require
documentation of identification, cultivation, physical and chemical
characteristics, pharmacology, standards of clinical use, stability, and
preparation methods along with three reference samples. To date over 1,000 new
drug applications have been approved. Recent legislation in Malaysia requiring
the registration of herbal products has lead to the licensing of 4,778 (28.9%)
out of 16,518 products. Many (71.1%) failed to satisfy strict regulatory
requirements as to their quality, safety and efficacy. 13 Research activities
currently include evaluation of active herbal constituents for efficacy,
bioavailability and toxicity. In Japan, 80% of practising physicians have
experience using herbal formulas.
Japan now produces 210 Kampo
herbal formulas according to strict quality controls, 147 of which are covered
by health insurance. It was the consensus of the group that quality control
measures should continue to be promoted.
Phytochemical and pre�clinical
research are the areas of research in which the active components of herbal
remedies are isolated, their structures identified and biological activities
analyzed for mechanisms of action, toxicity, etc. Recently in the Republic of
Korea, acubin was isolated from Plantago asiatica, a traditional medicinal
plant that has been used for hepatitis B. Derivatives synthesized from the lead
compound, higenamine, isolated from Aconitum tuber, have shown activity as an
anti�platelet aggregating agent. Extensive research has been performed in Japan
on about 30 Kampo formulas on a pre�clinical or basic science level. One
example of this research is the work on the immunostimulating activity of
Juzen�Taiho�To (JTT). JTT consists of ten different component herbs. It has
been shown to influence the immune system by enhancing the T�cell dependent
antibody response, phagocytosis, anti�complementary activity and mitogenic
activity against spleen B cells in mice. The biological activity was identified
to originate from three different types of polysaccharides having different
activities. These three different types of polysaccharides were separated into
22 unique active pectic polysaccharides. Although JTT consists of ten component
herbs, the corresponding carbohydrate�lignan complex fractions from each
component herb did not demonstrate immunity enhancing activity. However, when
at least five certain herbs were combined, the activity was observed.
The series of experiments
strongly suggests the presence of a synergistic effect in this Kampo
preparation. Examples of other areas of Kampo medicine that are currently being
investigated include the anti�dementia actions on the nervous system, treatment
of liver diseases, allergic reactions, anti�influenza, anti�atherosclerosis
activity, suppression of chronic inflammatory airway disease and anti�pyretic
activity.
6.4 Clinical research in herbal medicine
The range and number of human
clinical trials of traditional herbal medicines performed in China, Republic of
Korea, Japan and other countries are extensive. For the purposes of this
summary a sub�group of participants reviewed and graded a limited number of
studies submitted to the group by participants to provide a snapshot of
research activity in this area. The focus of activity of this group was on
oriental herbal medicine.
The following six major aspects of clinical trial design
were utilized to objectively evaluate the studies at hand:
� the use of explicit, objective entry criteria;
� appropriate use of a control group;
� random allocation of patients to control and intervention
groups;
� appropriate levels of blinding;
� complete follow�up and reporting on all patients recruited
into the trial; and
� the selection of unambiguous and clinically meaningful,
patient�based end points.
Two additional criteria were
considered important by the group if traditional medicine were to be assessed
appropriately:
� the use of a traditional diagnostic framework in guiding
treatment; and
� tailoring the treatment to trial subjects where possible.
These clinical trial criteria
were used to grade clinical trials according to the strength of evidence they
represent. The trials reviewed are summarized below and presented in Table 1.
The quality of evidence represented by each trial was rated according to the
guidelines in section.
Summary of studies
Gastroenterology
One well�performed randomized
controlled trial has been recently published in English on irritable bowel
syndrome. This trial was considered to represent level II evidence.
Hepatology
A randomized, prospective
unblinded Japanese study of a traditional herbal formula demonstrated reduced
cumulative incidence of hepatocellular carcinoma and increased survival of
patients with cirrhosis. This trial was considered to represent level II
evidence.
A retrospective study also
demonstrated that long�term administration of a licorice root derivative was
effective in reducing the cumulative incidence of liver cancer in chronic
hepatitis C patients. This trial was considered to represent level IV evidence.
Reproductive endocrinology
An unblinded, randomized
controlled comparison of herbal medicine with conventional medicine in
polycystic ovary disease demonstrated positive outcomes along a number of
parameters although there were concerns about methodological standards. This
trial was considered to represent level II evidence.
A small randomized controlled
trial on intrauterine growth retardation demonstrated a positive outcome on
birth weight and placental villi but exhibited similar methodological problems.
This trial was considered to represent level II evidence.
Dermatology
Two studies of traditional herbal
medicine demonstrated effectiveness over placebo in both children and adults
with refractory atopic eczema. Both studies were deemed level II evidence.
Psychiatry
A randomized, placebo�controlled
blinded trial demonstrated the benefit of a traditional herbal formula in the
treatment of vascular dementia. Although there were some limitations in design
this study was credible overall. The trial was considered to represent level II
evidence (always with Table).
Reviews
In addition, one systematic review and one meta�analysis
were available for discussion.
Acute ischaemic or hemorrhagic stroke
A review and meta�analysis
performed on 15 clinical trials of a State approved traditional Chinese herbal
medicine, conducted between 1992�1996, revealed variable methodological quality
(unpublished). Only one of the clinical trials reported single blind procedure,
none double blind. All claimed a positive outcome.
However, the review identified significant problems with the
trial methodology.
Acute respiratory infections
A systematic review of clinical
trials of Chinese herbal medicines in acute respiratory infections concluded
that the inadequate methods of most studies made it difficult to interpret the
results with confidence.
Conclusions
Overall, the herbal trial reports
represent some good preliminary evidence of the efficacy of herbal medicine in
a number of clinical disorders including, but not limited to, those reported
above. There is further evidence in numerous other clinical areas. The process
of acquiring quantifiable clinical trial evidence on traditional oriental
herbal medicine is clearly underway.
However, whilst some good quality
research has been reported, there is a relative paucity of good clinical trials
and systematic reviews of the practice of traditional (oriental) herbal
medicine, and most remain published in non�English journals. Whilst the
outcomes of the trials largely support the efficacy of herbal medicine, many
are compromised by methodological flaws. The clinical trials published in
English are few. There is a significant volume of clinical trials in the
Chinese herbal literature, although methodological problems have been a major
concern which weaken the credibility of the outcomes.
7. HARMONIZING TRADITIONAL AND MODERN MEDICINE: CONCLUSIONS
AND RECOMMENDATIONS
The meeting participants
recognized that a large proportion of the population in the Region use
traditional medicine as a primary means of care. Traditional medicine will
continue to exist as a separated medical system for some time. It was noted
that many users of traditional remedies also use modern medicine at the same
time. Many medical doctors apply both traditional and modern medicine.
Harmonization of traditional and modern medicine will, therefore, ensure that
the two approaches work effectively side by side properly.
7.1 Towards harmonization of traditional and modern medicine
By the end of the conference, the
consultation group identified a number of issues that were important in the
harmonization of traditional and modern medicine. The group recommended several
steps which would contribute to the goal of harmonizing the two systems of
medicine.
7.1.1 Promoting an evidence�based approach
An evidence�based approach is
important in harmonizing traditional and modern medicine and minimizing bias.
There is a need to acknowledge the evidence base within traditional medicine;
traditional medicine should recognize the importance to clarify the extent and
limitations of traditional practice through methodologically sound research.
Importantly, the consultation group did not see any major problems with
applying the principles of evidence�based medicine (including the randomized
controlled trial) to TM research and practice. This is a process that will only
assist in increasing the credibility of TM practices. To this end, researchers
should endeavor to utilize rigorous features in clinical trial design as
described in sections 5 and 6. All suitable and appropriate study designs
should be encouraged for the purpose of acquiring useful information on the
efficacy and safety of traditional practices and medicines. This would include
drawing on study designs such as case series, retrospective studies, cohort and
case-control studies, and involvement of traditional healers in documentation
of treatment outcomes.
Research should establish the
value of traditional medicine in not only treating disease, but also in
promoting health and wellness.
This could include research on
the use of combinations of therapy (for example, acupuncture with dietary
changes and/or herbal medicine).
The concept of an holistic
approach to treating patients is important and paramount in traditional
medicine. Hence, outcome measures in clinical trials need to be relevant to the
whole health of patients. A strong emphasis was placed on the need to develop
and validate the reliable, clinically meaningful, multi�dimensional outcome
measures that related to quality of life.
Whenever possible, researchers
should endeavor to utilize rigorous features in clinical trial design,
including;
� the use of explicit, objective entry criteria;
� appropriate use of a control group;
� random allocation of patients to control and intervention
groups;
� appropriate levels of blinding;
� complete follow�up and reporting on all patients recruited
into the trial; and
� the selection of unambiguous and clinically meaningful,
patient�based end points.
A more conducive environment for
research on traditional medicine needs to be set up. This includes looking into
the legal status and training practitioners, education of researchers, funding
and utilization of research findings.
In undertaking clinical research,
the Declaration of Helsinki and other guidelines relevant to ethical issues in
health research should be followed.
7.1.2 Encouraging a mutual respect
Lack of adequate education by
modern medical practitioners in the TM approaches to diagnosis and treatment,
and the lack of adequate education in designing methodologically sound research
by traditional medicine practitioners represent significant barriers to the harmonization
of traditional and modern medicine. In the past, non�TM trained researchers
conducted poor quality clinical research due to the inappropriate application
of TM techniques.
Similarly, poor quality research
resulted from TM practitioners failing to recognize the well�established
importance of rigorous approaches to performing clinical trials. Improved
relevant education is required on both sides.
While performing rigorous
research on TM, it must be emphasized that TM principles of practice should be
strictly adhered to. It is important that traditional medical theory is not
ignored in the context of a good trial design. In some cases, whilst a modern
medical diagnosis may be required for the purposes of screening and including
patients for a clinical trial, the trial should be designed to permit a
traditional diagnostic and therapeutic approach to practice. Practice is
particularly individualized in TM and a research design that moves too far from
TM practice would no longer achieve its purpose in evaluating TM. The
importance of collaboration between TM practitioners and clinical researchers
is apparent.
Trialists and researchers need to
develop expertise in both traditional medicine and research methodology, and
they need to ensure that research methodologies are appropriate to the practice
of traditional medicine. Furthermore, developing interpretations of traditional
medicine in terms of modern medical theory is also important. This can provide
credibility to the traditional medical diagnostic and theoretical concepts
without undermining its practice base.
Harmonization through mutual
respect of practices will occur if a wide range of well�performed clinical
trials proceed. Barriers to the performance of worthy clinical trials should be
minimized.
For example, it has been proposed
that since herbal medicines are available in the public arena and the
government has not sought to restrict their usage, a clinical evaluation of the
products should be encouraged. For the purpose of a clinical trial, safety
evaluation beyond the recorded history of use of the medicinal agents should
not generally be required. In fact, the clinical trial itself provides safety
information. Regulation and restriction, if required, should occur as a matter
of public risk minimization measure, not to obstruct evaluation of publicly
available products. This will provide an evaluation of effectiveness and assist
the government not only to define a regulatory position, but also to clarify
the potential role of the therapeutic agents concerned. This issue is of
relevance to clinical researchers, government regulators and institutional
ethics committees.
7.1.3 Disseminating information
Poor dissemination of research
literature related to the practice of TM presents a major barrier to
researchers worldwide. Some high quality basic science and clinical research on
many forms of traditional medicine exist only in Japanese, Korean or Chinese
language journals and are relatively inaccessible. Hence, there remains a need
to translate, collate and disseminate the relevant research findings of the
last two decades. In addition, TM researchers need to reach a broad readership
and raise the level of awareness.
WHO, researchers, professional
associations, research institutes and other agencies should consider mechanisms
to improve communication and information sharing. These include further
networking, newsletters, expert meetings, conferences and other mechanisms.
Due to the vast array of TM
practices, geographical separation and cultural diversity, communication, even
in the same tongue, presents a barrier to harmonization. The development of a
�modern� language for TM may lead to better understanding of its theory and
practice by the public, policy�makers and the medical society. A common language
will contribute to further cooperation amongst researchers.
The general public will also
benefit from information on the safety and effectiveness of traditional
medicine and the outcome of scientific research explained in simple language
easily understood.
7.1.4 Research on herbal medicine
The basic science areas of herbal
medicine provides a means of assuring the quality and safety of herbal
remedies. It may also lead to the discovery of clinically important drugs.
There is a need to change the
order in which basic science research is performed in the discovery of new
drugs in the practice of traditional herbal medicine. Historically, basic
science research in herbal medicine begins with the selection of plants based
on widespread use and folklore. This is followed by intensive laboratory work
leading to the development of bioassays, isolation techniques and
characterization of active constituents, determination of the mechanism of
action and a battery of toxicology testing. Promising agents are then moved
into clinical trials. Although many extremely useful drugs have been discovered
using this method, the vast majority of plants that undergo this method of
evaluation do not yield clinically useful drugs. Applying two new strategies
that embrace the principles of evidence�based medicine may dramatically
increase this success rate.
The first strategy is to
categorize plants and traditional medicine formulas according to an Evidence
Rated Research Scale. By utilizing this style of categorizing plants and herbal
formulas, researchers will have a common language in which to assess the body
of knowledge available for each plant or formula.
Evidence Rated Research Scale consists of the following:
1. Single plant or herbal formula that has extensive
positive clinical efficacy, proven safety, known mechanism of action,
structurally identified active compounds and strict quality control which fully
supports its use in the general population
2. Single plant or herbal formula that has extensive
pre-clinical in vitro and/or in vivo positive research results along with basic
science research on safety, mechanism of action, structurally identified active
compounds and strict quality control which supports its use in the general
population but has not been clinically verified.
3. Single plant or herbal formula used and broadly accepted
as efficacious based on a long history of use that has been tested for quality
control and safety.
Clinical efficacy has not been verified by randomized
controlled trials.
4. Single plant or herbal formula used and broadly accepted
as efficacious based on a widespread and long history of use. Clinical efficacy
has not been verified by randomized controlled trials.
5. Single plant or herbal formula used locally or only
rarely found in the literature.
The second strategy involves shifting the initial focus of
TM herbal research from that of basic science to clinical outcomes.
According to this approach, high
quality clinical trials would initially be performed using plants or herbal
formula believed to be efficacious. Those TM herbal remedies confirmed to be
effective would then undergo rigorous scientific investigation. By applying a
Post�clinical Basic Science Research Approach, the basic research scientists
will conduct their investigations starting with clinically proven effective
material which may enhance and expedite the discovery new clinically effective
agents and research tools. The format of the Post�clinical Basic Science
Research Approach is as follows:
(1) Each interested regional country identifies and
prioritizes diseases that warrant research.
(2) Single plants or herbal formulas used to treat those
diseases might then be chosen for a variety of reasons (most notably, clinical
experience) although preference might also be given to plants appearing high on
the
Evidence Rated Research Scale.
(3) Safety and toxicity studies should be carried out
(unless already documented). A long history of human use is acceptable evidence
of basic safety under this scheme.
(4) High quality, evidence�based clinical trials should then
be designed and performed.
(5) Plants or formulas that are shown to be positive in
clinical trials will then undergo rigorous basic science research including:
� isolation and structure elucidation of the active
compound(s);
� dosage, bioavailability and advanced safety studies;
� pharmacokinetics and mechanism of action identification;
� activity enhancing chemical modification studies;
� other types biological activity studies; and
� quality control studies to standardize
phytopharmacological equivalents.
Thus, by combining the knowledge
and use of traditional medicine to obtain clinically useful evidence in which
to focus the resources of modern medicine�s basic science research, the health
of the people utilizing both systems may be improved.
During the process of evaluating
traditional herbal remedies, the responsibility of TM practitioners will be to
facilitate the appropriate evaluation of effectiveness, while other medical
research techniques provide the capacity and approaches to determine how the
therapeutic agents work. This order of activity differs from conventional
synthetic or semi�synthetic pharmaceutical research for new therapeutic
chemical constituents, where the latter has had no marketplace exposure or
history of human usage in therapy. This is an important distinction: TM
therapeutics have a long history of human usage and previously accepted
marketplace exposure. This distinction should motivate traditional medicine
practitioners and relevant industry sectors to collaborate to raise adequate
funding and to develop and fulfill meaningful research plans.
An awareness of the principles of
TM practice is important in basic science research. The synergism of activity
of the herbs demonstrated by the Japanese studies reported in section 6.3,
where individual herbs failed to show activity demonstrated by the whole
formula, highlights the importance of adopting traditional approaches to the
utilization of traditional medicines. Attention in research should be paid to
the synergistic behaviour of whole formulations in contrast to actions and
safety of single bioactive agents.
In accordance with the UN
Convention on Biologic Diversity held in Rio de Janeiro in 1992, researchers in
the development of herbal remedies must recognize the importance of the
conservation of diverse plant species.
7.1.5 Research on acupuncture
There is a need to standardize
animal models in basic acupuncture research by considering standardized models
from other fields. The animal models used in acupuncture research need to be
understandable, reproducible, and exchangeable. Animal research must correlate
as closely as possible to clinical reality.
Acupuncture researchers need to
document the morphological and physiological connection to internal organs
through the use of technologically advanced modalities such as functional
magnetic resonance imagine (MRI) and positron emission tomography (PET) scans.
This could lead to better understanding of the importance of acupoints and
meridians, including the awareness of micro�anatomy, connective tissue and
metabolic aspects. In view of the costs associated with these technologies, it
was suggested that ways to co�ordinate and facilitate the use of these
resources must be promoted by governmental bodies.
Acupuncture research presents
some unique methodological challenges that can cause problems with respect to
the maintenance of blinding and thus may open trials of acupuncture to bias.
The acupuncture researcher must consider the appropriate selection of sham
procedures in order to address these issues. Some points to consider include:
� Sham needling presents difficulties related to choice of
position, stimulation, duration and technique. Patient expectations and
experience with acupuncture can result in failures in blinding.
� Mock TENS is difficult to undertake because the patient
can perceive the active stimulation.
� Minimal acupuncture may have a mild effect and can be
distinguished from true acupuncture by the subject.
� Placebo acupuncture, with a retractable blunt needle,
demonstrates promise but has not yet been adequately evaluated in clinical
trials.
� Alternative treatment, such as physiotherapy, may give
indication of effectiveness over �standard care�.
Researchers need to be very
explicit when describing experimental trials so that all the steps of design
and procedures are fully explained in order to allow other researchers to
repeat the same experiment and grade the level of evidence.
7.1.6 Other perspectives on acceptance
Traditional medicine is rooted in
respective cultures and traditions, so there are many issues and perspectives
that need to be examined aside from the basic science and clinical aspects.
Like all other systems of health care, the development of traditional medicine
is not solely driven by science but equally by policy, and economic and
socio�behavioral factors. These factors can act as a bridge between research
and action.
Research on traditional medicine
beyond the basic science and clinical perspective should be conducted. Other
scientists such as social scientists, health economists and epidemiologists
need to be part of multi�disciplinary teams conducting research in traditional
medicine.
There is a need to understand the health and health care
seeking behaviour of the users and non�users in the following areas:
� pathways to seeking care � issues such as delay of seeking
care, concomitant use, doctor shopping and switching from one medical system to
another;
� patterns of use � issues such as user characteristics,
medical conditions for which traditional medicine are sought, extent and
frequency of use, payments, factors associated with use and non�use and effects
of education and policy on use and non�use;
� provider behaviour � issues such as provider
characteristics, prescribing behaviour and referrals; and
� policy studies � cost analysis and issues such as effects
of education and policy on patterns of use.
Research in the context of the
above will provide useful evidence to policy�makers in dealing with traditional
medicine.
Business involvement in TM is a
global concern. It is possible that profit motivation could override safety,
efficacy and health concerns. Issues of professionalism, ethics and marketing
are important areas for future research. Some examples include:
� impact of TM on health care expenditures (e.g. insurance
coverage);
� investment in product development by business/ commercial
sector (their concerns, marketing behaviour, and interest in private investment
in TM)
Governments should actively
promote the rational use of traditional medicine that have been scientifically
validated. To do so, they need a national policy for approving those drugs and
techniques that are safe and effective for specified clinical indications.
The adoption of such policy will
help to overcome some of the legal barriers against the use of traditional
medicine.
7.2 Operational recommendations
There are clear challenges to the
harmonization of traditional and modern medicine. Better access to information,
facilitating appropriate clinical trials, improving rigour in clinical trials,
improving education and collaboration of practitioners and researchers, and
respecting traditional practices in research are all important steps towards
achieving harmonization.
It is recognized that the idea
for harmonizing traditional and modern medicine will not occur immediately. To
accumulate evidence based on research can be regarded as the first step.
However, much more is involved in harmonization of traditional and modern
medicine. The group also believes that a number of simple actions can be taken
to initiate the efforts for harmonization. In addition to the suggestions and
recommendations mentioned above, the group made the following operational
recommendations to establish a framework to begin the process.
(1) WHO should continue to encourage governments to adopt
policies to promote the rational and safe use of traditional medicine.
(2) WHO and its Member States should support the
harmonization and appropriate integration of traditional medicine with modern
medicine.
(3) WHO should collaborate with
research institutes and researchers engaged in research on traditional medicine
to disseminate their findings as widely as possible, including publication of
their results in broadly circulated English language journals. Furthermore, professional
associations, journals, research institutes and other agencies should endeavour
to make available in English the reports of research studies presently
available only in Chinese, Japanese and Korean literatures. This should include
the preparation and dissemination in English and native languages such as
Chinese, reviews of research conducted in other countries. The successful
dissemination of the outcomes of well�designed and well�performed research will
assist traditional and modern medicine practitioners to make informed decisions
about the most effective therapy for patients.
(4) Appropriate mechanisms to improve dissemination of and
access to information resulting from research activities should be developed:
� WHO should assist in updating available databases on
traditional medicines and utilization of those databases by researchers and
other interested users;
� WHO should consider commissioning the preparation of a
document which could be available in English and native languages, to
illustrate the use of the evidence�based approach to research in traditional
medicine; and
� WHO should undertake activities (forming networks,
organizing meetings and conferences, and using electronic media) for
information dissemination.
(5) WHO should continue to
co�ordinate data analysis on important traditional remedies. Researchers who
have expertise in trial evaluation and traditional medicine should be mobilized
to evaluate research papers published in the last five to ten years according
to the levels of EBM. This could then form the framework for a
scientifically�evaluated traditional medicine.
(6) As part of acquiring clinical
evidence, relevant governments or professional agencies should ensure that
appropriate adverse event reporting and recording mechanisms are in place.
Regular summary findings should be disseminated by the relevant government or
professional agency to interested parties.
(7) WHO should support the training of people with knowledge
of traditional medicine to acquire skills in research methodologies including
clinical epidemiology.
Furthermore, WHO should encourage
and support the training of clinical trialists to acquire training in the
theory and fundamentals of traditional medicine.
(8) WHO and its Member States
should advocate, support and encourage the conducting of high quality research
in traditional medicine, including clinical research, basic sciences, policy
issues (legal and educational), and social, behavioural and economic issues.
Research Guidelines for Evaluating the Safety and Efficacy of Herbal Medicine
and Guidelines for Clinical Research on Acupuncture, prepared and published by
WHO Regional Office for the Western Pacific, provide valuable guidance on
principle and methodology for designing, conducting and evaluating basic
scientific and clinical research in traditional medicine.
(9) WHO should encourage research to establish the value of
traditional medicine in promoting health and wellness beyond treating diseases.
(10) WHO and its Member States
should advocate that, provided adequate evidence of safety (such as history of
human use) is available, clinical trials of widely used and established
traditional remedies may be undertaken prior to obtaining the results of
extensive �pre�clinical� basic sciences research.
WHO has had a traditional
medicine programme for the last 20 years. It was developed in conjunction with
the goal of health for all and the adoption of the primary health care
approach. WHO recognizes that a large percentage of the population of the
Western Pacific Region still uses traditional medicine to treat disease and
maintain health. Figures show that around 50% of the population in some
countries in the Region is using traditional medicine for different reasons.
This is also the case elsewhere in the world. For example, studies show that
use of traditional or complementary medicine in the U.S.A. has increased from
33.8% of the population in 1990 to 42.1% in 1997. It seems probable that
interest in traditional medicine will continue to increase in the future.
We support Member States in their
efforts to bring the proper use of traditional medicine into the mainstream of
general health service systems. WHO�s involvement in traditional medicine is
focused on our joint efforts with Member States for national policy
development, regulation of traditional medicine, use of traditional medicine in
supporting primary health care, research and information exchange. WHO supports
only a few specific remedies and techniques used by traditional medicine, such
as use of artemisinin and acupuncture. For example, use of artemisinin in some
countries as a first line anti-malaria drug is supported by WHO.
In the case of acupuncture, in
June 1997, a provisional list of 43 diseases and disorders that lend themselves
to acupuncture treatment was drawn up by a WHO Interregional Seminar on
Acupuncture, Moxibustion and Acupuncture Anaesthesia held in Beijing, China.
However, the selection of those diseases and disorders was based on clinical
experience and not necessarily on controlled clinical research. A number of
resolutions adopted by the World Health Assembly and the Regional Committee for
the Western Pacific have urged Member States to undertake research on
traditional medicine and to improve cooperation between traditional and modern
medicine, especially as regards the use of scientifically proven, safe and
effective traditional remedies. However, lack of scientifically-based evidence
limits our involvement in supporting the use of specific traditional remedies.
We believe that we need to keep an open mind on traditional medicine. However,
we would like to endorse a therapy with solid scientific evidence.
Long historical use of many forms
of traditional medicine and experiences passed from generation to generation
have demonstrated the effectiveness of traditional remedies. However,
scientific research is needed to provide additional evidence of its safety and
effectiveness.� Scientific research will
serve as the basis of our endorsement of the use of traditional remedies and
techniques. The major tasks of this consultation meeting are, first, to review
the outcome of previous research on traditional medicine and, second, to
identify research priorities and sound research methods. By identifying a
research strategy, we will be able to focus on the
Looking back over this century,
it is clear that modern medicine developed very quickly in the last 100 years.
However, if we look back over the whole millennium, traditional medicine
represented main stream of health care to deal with the health problems of
human beings. Although modern medicine has enabled us to make great advances,
particularly in disease control, many threats to human health remain. Some of
these are new threats, such as lifestyle-related diseases including drug abuse and
depression.
(back
to content)
4.1 A History of Metaphysics w
The Presocratics
Although metaphysics properly
begins with Aristotle�s search for the underlying principles of reality, he
looked to the claims of the pre-Socratics as possible answers to deep questions
such as �what is there?� and what are the causes behind everything.
Most of their pre-Socratic claims
were speculations about the physical nature of the cosmos and its origins. In
some ways, the pre-Socratics might be viewed as the earliest natural
scientists, with their strong interest in physics, chemistry, astronomy,
geology, meteorology, and even psychology. By contrast, Socrates would change
the subject to ethical issues. It took Aristotle to return to cosmological,
theological, and metaphysical issues first raised by the pre-Socratic
philosophers and great authors like Homer and Hesiod.
The two great antagonist views
were from Parmenides and Heraclitus. For Parmenides, �All is One,� there is no
such thing as nothing (the void of the atomists), and change is an illusion
(all of Zeno�s paradoxes of motion supported his master�s claims).
For Heraclitus, by contrast, �All
is Flux.� There is nothing but change. �You can�t step in the same river
twice.� The one great positive insight of Heraclitus was that behind all
changes there are laws � the �Logos.� He clearly anticipates the modern notion
of the laws of nature that control all change.
Aristotle gives great credit to
several pre-Socratic philosophers, starting with Thales of Miletus, for
attempting �natural� explanations for phenomena where earlier thinkers had
given only poetic, mythological, or theological stories. Although the
explanations were very simple, they were as basic as could be. Thales said �All
is Water.� This means everything material now is somehow made from water. This
is the sort of basic principle and discovery of basic elements of nature that
Aristotle was after.
For Anaximander of Miletus, the
first principle is a sort of indefinite and unbounded moving element. For
Anaximenes, another Milesian, the primal element from which all is made is air.
For his primal element, Heraclitus chose Fire, because unlike Thales�s Water
and Anaximenes� Air (and of course Earth), Fire is always rapidly changing.
Pythagoras gave Plato the idea
that mathematics could supply the most fundamental explanations of reality,
namely the Forms, the organization and arrangement of things in the universe.
Most other pre-Socratics were
focused on material explanations, especially the atomists, Democritus and
Leucippus, who were physical determinists, and Epicurus, who agreed about the
atoms and void, but made the atoms swerve to add an element of indeterminism to
events.
Socrates and Plato Considered as
a metaphysicist, Plato�s greatest contribution was to promote the Forms or
�Ideas.� Plato coined the Greek word for idea (ιδέα) from
the past tense of the verb �to see.� For Plato, ideas are something we have
seen when souls made their great circuit of the heavens before coming to Earth.
Plato was inspired by Pythagoras. Other than Pythagoras,
whose fundamental understanding of reality was based on mathematics, the other
pre-Socratics were all materialists.
Socrates had no interest in the
materialists and their physical theories. He wanted to understand the human
being and ethical values. He famously insisted that �virtue is knowledge.�
Anyone doing an evil thing must be doing it out of ignorance of the Good.
Ironically, Socrates spent his life showing that very few,
if any, people understand what it is to know anything.
ARISTOTLE
Metaphysics has signified many
things in the history of philosophy, but it has not strayed far from a literal
reading of �beyond the physical.� The term was invented by the 1st-century BCE
head of Aristotle�s Peripatetic school, Andronicus of Rhodes. Androni cus
edited and arranged Aristotle�s works, giving the name Metaphysics
(τα μετα τα
φυσικα βιβλια), literally
�the books beyond the physics,� perhaps the books to be read after reading
Aristotle�s books on nature, which he called the Physics. The Greek for nature
is physis, so metaphysical is also �beyond the natural.�
Proponents of modern naturalism deny the existence of
anything metaphysical, which some regard as �supernatural.�.
Aristotle never used the term
metaphysics. For Plato, Aristotle�s master, the realm of abstract ideas was
more �real� than that of physical. i.e., material or concrete, objects, because
ideas can be more permanent (the Being of Parmenides), whereas material objects
are constantly changing (the Becoming of Heraclitus).
Where Plato made his realm of
ideas the �real world,� Aristotle made the material world the source of ideas
as mere abstractions from common properties found in many concrete objects.
Neoplatonists like Porphyry worried about the existential status of the
Platonic ideas. Does Being exist? What does it mean to say �Being Is�?
In recent centuries then, metaphysical has become �beyond
the material.� Metaphysics has become the study of immaterial things, like the
mind, which is said to �supervene� on the material brain.
Metaphysics is a kind of
idealism, in stark contrast to �eliminative� materialism. And metaphysics has
failed in proportion to the phenomenal success of naturalism, the idea that the
laws of nature alone can completely explain the contents of the universe.
The books of Aristotle that
Andronicus considered �beyond nature� included Aristotle�s �First Philosophy� �
ontology (the science of being), cosmology (the fundamental processes and
original causes of physical things), and theology (is a god required as �first
cause?�).
Aristotle�s Physics describes the
four �causes� or �explanations� (aitia) of change and movement of objects
already existing in the universe (the ideal formal and final causes, vs. the
efficient and material causes). Aristotle�s metaphysics can then be seen as
explanations for existence itself. What exists? What is it to be? What
processes can bring things into (or out of) existence? Is there a cause or
explanation for the universe as a whole?
In critical philosophical
discourse, metaphysics has perhaps been tarnished by its Latinate translation
as �supernatural,� with its strong theological implications. But from the
beginning, Aristotle�s books on �First Philosophy� considered God among the
possible causes of the fundamental things in the universe. Tracing the regress
of causes back in time as an infinite chain, Aristotle postulated a first cause
or �uncaused cause.� Where every motion needs a prior mover to explain it, he
postulated an �unmoved first mover.� These postulates became a major element of
theology down to modern times.
Modern metaphysics is described
as the study of the fundamental structure of reality, and as such foundational
not only for philosophy but for logic, mathematics, and all the sciences. Some
see a need for a foundation for metaphysics itself, called metametaphysics, but
this invites an infinite regress of �meta all the way down (or up).�
Aristotle�s First Philosophy
included theology, since first causes, new beginnings or genesis, might depend
on the existence of God.
And there remain strong connections between many modern
metaphysicians and theologians.
THE STOICS
The Stoics divided their philosophy into three parts, logic,
ethics, and physics.
Stoic logic included rhetoric,
dialectic, grammar, epistemology and a philosophy of language. They developed
theories of concepts, propositions, perception, and thought. Their logic was
propositional, rather than the Aristotelian logic of syllogisms and predicates.
They defined five fundamental logical tools:
if p then q; p; therefore q (modus ponens);
if p then q; not q; therefore not-p (modus tollens);
either p or q; p; therefore not-q;
either p or q; not p; therefore q;
not both p and q; p; therefore not-q;
They had a strict interpretation
of the principle of bivalence (Aristotle�s non-contradiction) and the law of
the excluded middle. Every statement is either true or false, even statements
about the future, as Diodorus Cronus maintained. But Aristotle denied the present
truth or falsity of future statements with his analysis of future contingency
(e.g., the Sea Battle).
The Stoic philosophy of language
had a theory of signs long before Charles Sanders Peirce�s semiotics or
Ferdinand de Sausurre�s semiology. A signifier is an utterance of a name, a
proper noun (onoma). The name-bearer is the object or concept that gets
signified. The signification consists of the immaterial qualities that they
called lekta, or �sayables,� predicates that are true or false of the signified.
The sayables are that which subsists (grows and decays), the �peculiar
qualifications� of an individual.
Stoic physics included a wide
range of topics including ontology, cosmology, theology, psychology, and
metaphysics. The basic principles of the universe (Aristotle�s archai) are two
- matter and pneuma, a breath or psyche. Pneuma combined two of the four
fundamental elements, fire and air, representing hot and cold, as the active
principle.
A passive principle combined
earth and water as the basis for material objects. The Stoics regarded matter
as �unqualified� and inert. Changes in the material in an object they described
as generation and destruction (following Aristotle).
Pneuma is the cause (aition) of
change in the peculiar qualities of an individual that constitute growth and
decay, corresponding to the Platonic and Aristotelian forms and ideas that
shape a material object. Pneuma endows the bodies with different qualities as a
result.
The pneuma of inanimate object is called a �tenor� (hexis,
�having�).
What it �has� are qualities. Pneuma in plants has a (phusis,
�nature�).
Pneuma in animals the Stoics
called soul (psych�) and in rational animals pneuma includes the commanding
faculty (h�gemonikon)
The Stoics saw the identity of an
individual as its immaterial bundle of properties or qualities that they called
the �peculiarly qualified individual� or ἰδίος
ποιὸν.
Zeno of Cytium had formulated a
psychological theory of how we acquire beliefs that are justified empirically
and not by reasoning.
To form a belief is to give one�s
assent to an �impression� (a phenomenal appearance: phantasia) about the
material substrate of an object. Some perceptions are �cognitive� or
self-warranting. Assenting to them is a cognition or grasp (katal�psis) of
their objects. Assent should be restricted to these cognitive or kataleptic
impressions.
Cognitive impressions give us
infallible knowledge or wisdom. Our beliefs will then be constituted entirely
by self-warranting perceptual cognitions. Zeno argued that a cognitive
impression �stamps� the form of the object (its peculiar qualities) on our mind
or soul (pneuma), just as we now see immaterial information embodied in the
material brain, experiences recorded in our ERR.
Following Aristotle, the Stoics
called the material substance or substrate ὑποκείμενον
(or �the underlying�). This material substrate is transformed when matter is
lost or gained, but they said it is wrong to call such material changes �growth
(αὐξήσεις) and decay
(φθίσεις).� The Stoics suggested they should
be called �generation (γενέσεις) and
destruction (φθορὰς).� These terms were already
present in Aristotle, who said that the form, the essence, is not generated.
He said that generation and
destruction are material changes that do not persist (as does the Stoic
peculiarly qualified individual).
�It is therefore obvious that the
form (or whatever we should call the shape in the sensible thing) is not
generated�generation does not apply to it�nor is the essence generated; for
this is that which is induced in something else either by art or by nature or
by potency. But we do cause a bronze sphere to be, for we produce it from
bronze and a sphere; we induce the form into this particular matter, and the
result is a bronze sphere... For if we consider the matter carefully, we should
not even say without qualification that a statue is generated from wood, or a
house from bricks; because that from which a thing is generated should not
persist, but be changed. This, then, is why we speak in this way.� 1
It is important to see that the
Aristotelian view is very similar to the Stoic - that individuals are
combinations of matter and form.
At times Aristotle made the
matter the principle of individuation, at other times he stressed the
immaterial qualities or �affections,� as did the Stoics, with their peculiarly
qualified individual (ἰδίος ποιὸν).
1 Aristotle, Metaphysics, Book VII, � vii & viii
Is Aristotle here the source of the four Stoic genera or
categories?
The term �substance� (οὐσία)
is used, if not in more, at least in four principal cases; for both the essence
and the universal and the genus are held to be the substance of the particular
(ἑκάστου), and fourthly the substrate (ὑποκείμενον).
The substrate is that of which the rest are predicated, while it is not itself
predicated of anything else. Hence we must first determine its nature, for the
primary substrate (ὑποκείμενον)
is considered to be in the truest sense substance.
Aristotle clearly sees a statue
as an integral combination of its form/shape and its matter/clay, not two
distinct things, as Skeptics would claim. Now in one sense we call the matter (ὕλη)
the substrate; in another, the shape (μορφή); and in a
third, the combination.
Both matter and form and their
combination are said to be substrate. of the two. By matter I mean, for
instance, bronze; by shape, the arrangement of the form (τὸ
σχῆμα τῆς ἰδέας);
and by the combination of the two, the concrete thing: the statue (ἀνδριάς).
Thus if the form is prior to the matter and more truly
existent, by the same argument it will also be prior to the combination.2
The Academic Skeptics attacked
the Stoics, saying Stoics were making single things into dual beings, two
objects in the same place at the same time, but indistinguishable.
�. . . since the duality which
they say belongs to each body is differentiated in a way unrecognizable by
sense-perception. For if a peculiarly qualified thing like Plato is a body, and
Plato�s substance is a body, and there is no apparent difference between these
in shape, colour, size and appearance, but both have equal weight and the same
outline, by what definition and mark shall we distinguish them and say that now
we are apprehending Plato himself, now the substance of Plato? For if there is
some difference, let it be stated and demonstrated.� 3
Many of the classic metaphysical
puzzles are arguments over this dual nature of something as matter and form,
especially Dion and Theon, Tibbles, the Cat, The Growing Argument, The Ship of
Theseus, and The Statue and the Clay.
2 Aristotle, Metaphysics, Book VII, � iii, 1-2
3 Anonymous Academic treatise, Oxyrhynchus Papyrus 3008 in
Stoic Ontology,
The Hellenistic Philosophers, A. Long and D. Sedley, p.167
Modern metaphysicians mistakenly think that matter alone
constitutes an entity.
ACADEMIC SKEPTICS
Fundamentally, the Skeptics attempted to deny knowledge,
including epistemology and metaphysics.
Arcesilaus, the sixth head or scholarch of the Platonic
Academy.
Under him, the Academy returned
to the Socratic method and engaged in negative dialectics that denied the
possibility of knowledge (akatal�psia). Arcesilaus realized that he could not
say that he knows nothing without making a knowledge claim. This mitigated
absolute skepticism.
The Academic Skeptics refused to
accept any philosophical arguments that claimed to justify knowledge. Whatever
reasons are used to justify something must themselves be justified, leading to
an infinite regress. The Skeptics recommended that their followers therefore
suspend (epoch�) all judgments.
Most of Arcesilaus�s best known
arguments were dialectical attacks on the Stoics. His major Stoic opponent was
Chrysippus, whose philosophy of �assent� was more or less the opposite of
Arcesilaus� epoch�. Stoic epistemology was more empirical than the logical and
rational approach of the Skeptics, which allowed them to generate several
dialectical puzzles and paradoxes from the Stoic premises or first principles.
THE SCHOLASTICS
For medieval philosophers,
metaphysics was understood as the science of the supersensible. Albertus Magnus
called it science beyond the physical. Thomas Aquinas narrowed it to the
rational cognition of God. John Duns Scotus disagreed, arguing that only study
of the world can yield knowledge of God. Aquinas and Scotus can be seen as the
founders of the great division in philosophy between continental rationalism
and British empiricism.
It began as a theological dispute
over the freedom of God. Does God have freedom of the will or is God
constrained by Reason? If God must be rational, then one can deduce everything
about the world by reasoning in an ivory tower. If God was free to create
anything, knowledge requires an empirical investigation of the world.
Scholastic philosophers mostly
returned metaphysics to the study of being in itself, that is, ontology, which
again today is the core area of metaphysical arguments. In renaissance Germany,
Christian Wolff broadened metaphysics to include psychology, along with
ontology, cosmology, and natural or rational theology. In renaissance England,
Francis Bacon narrowed metaphysics to the Aristotelian study of formal and
final causes, separating it from natural philosophy which he saw as the study
of efficient and material causes.
DESCARTES
Ren� Descartes made a turn from
what exists to knowledge of what exists. He changed the emphasis from a study
of being to a study of the conditions of knowledge or epistemology.
Descartes was the origin of the
mind-body problem. 4 He famously divided the world into mind (the ideal realm
of thoughts) and body (the material world). For him, the physical world was a
deterministic machine, but our ideas and thoughts could be free (undetermined)
and could change things in the material world (through the pineal gland in the
brain, he thought).
Information philosophy restores
an immaterial mind to the impoverished and deflated metaphysics that we have
had since empiricism and naturalism rejected the dualist philosophy of Ren�
Descartes and its troublesome mind-body problem.
LEIBNIZ
Gottfried Leibniz had a vision of
a universal ambiguity-free language based on a new symbol set, a characterica
universalis, and a machine-like calculus ratiocinator that would automatically
prove all necessary truths, true in �all possible worlds.� Gottlob Frege called
Leibniz�s idea �a system of notation directly appropriate to objects.� In the
three hundred years since Leibniz had this vision, logical philosophers and
linguistic analysts have sought those truths in the form of �truth-functional�
propositions and statements formulated in words, but they have failed to find
any necessarily �true� connection between words and objects.
Information philosophy uses such
system of notation, not in words, but in bits of digital information. And the
interconnected computers of the Internet are not only Leibniz�s calculus
ratiocinator, but humanity�s storehouse of shared experiences and accumulated
knowledge. Like the individual experience recorder and reproducer (ERR) in each
human mind, the World Wide Web is our shared Knowledge Recorder and Reproducer.
Computer simulations of physical and biological processes are the best
representations of human knowledge about the external world of objects.
Leibniz�s Principle of Sufficient
Reason says that every event has a reason or cause in the prior state of the
world. This appears to commit him to a necessary determinism, but like the
ancient compatibilist Chrysippus, Leibniz argued that some empirical things are
contingent.
Leibniz formulated many logical principles that play a major
role in current metaphysical debates.
One is his Principle of
Contradiction (Aristotle�s Principle of Non- Contradiction). A proposition
cannot be true and false at the same time, and that therefore A is A and cannot
be not A. That A is A follows from what Leibniz called the Identity of
Indiscernibles, the idea that no differences are perceivable between identical
things. This came to be known as Leibniz�s Law.
The Metaphysics of Identity Leibniz calls identity of any
object with itself as a primary truth.
�Primary truths are those which
either state a term of itself or deny an opposite of its opposite. For example,
�A is A�, or �A is not not-A�; If it is true that A is B, it is false that A is
not B, or that A is not-B�; again, �Each thing is what it is�, �Each thing is like
itself, or is equal to itself, �Nothing is greater or less than itself�and
others of this sort which, though they may have their own grades of priority,
can all be included under the one name of �identities�.
All other truths are reduced to
primary truths by the aid of definitions�i.e. by the analysis of notions; and
this constitutes a priori proof, independent of experience. I will give an
example.
A proposition accepted as an
axiom by mathematicians and all others alike is �The whole is greater than its
part�, or �A part is less than the whole�. But this is very easily demonstrated
from the definition of �less� or �greater�, together with the primitive axiom,
that of identity. The �less� is that which is equal to a part of another
(�greater�) thing. (This definition is very easily understood, and agrees with
the practice of the human race when men compare things with one another, and
find the excess by taking away something equal to the smaller from the larger.)
So we get the following reasoning: a part is equal to a part of the whole
(namely to itself: for everything, by the axiom of identity, is equal to
itself). But that which is equal to a part of the whole is less than the whole
(by the definition of �less�); therefore a part is less than the whole.5
4. There are no two individuals indiscernible from one
another...
Two drops of water or milk looked
at under the microscope will be found to be discernible. This is an argument
against atoms, which, like the void, are opposed to the principles of a true metaphysic.
5. These great principles of a
Sufficient Reason and of the Identity of Indiscernibles change the state of
metaphysics, which by their means becomes real and demonstrative; whereas
formerly it practically consisted of nothing but empty terms.
6. To suppose two things
indiscernible is to suppose the same thing under two names.� 6 Information
philosophy restores the metaphysical existence of a Cartesian realm that is
�beyond the natural� in the sense since at least David Hume and Immanuel Kant
that the �laws of Nature� completely determine everything that exists,
everything that happens, everything that exists in the phenomenal and material
world.
5 Leibniz.. �Primary Truths,� in Philosophical Writings, ed.
G. H. R. Parkinson, p.87
6 Leibniz. ��Correspondence with Clarke,� in Philosophical
Writings, p.216
While information philosophy is a
form of Descartes� idealism/ materialism dualism, it is not a substance
dualism. Information is a physical, though immaterial, property of matter.
Information philosophy is a property dualism.
Abstract information is neither
matter nor energy, although it needs matter for its embodiment and energy for
its communication.
Information is immaterial. It is
the modern spirit, the ghost in the machine. It is the mind in the body. It is
the soul. And when we die, our personal information and its communication
perish. The matter remains.
The Empiricists
For empiricists in England like
John Locke and David Hume, metaphysics included the �primary� things beyond
psychology and the �secondary� sensory experiences. They denied that any
knowledge was possible apart from experimental and mathematical reasoning. Hume
thought the metaphysics of the Scholastics is sophistry and illusion.
If we take in our hand any
volume; of divinity or school metaphysics, for instance; let us ask, Does it
contain any abstract reasoning concerning quantity or number? No. Does it
contain any experimental reasoning concerning matter of fact and existence?
No. Commit it then to the flames: for it can contain nothing
but sophistry and illusion.7
Hume criticized the Theory of
Ideas of his fellow British empiricists John Locke and George Berkeley. If, as
they claim, knowledge is limited to perceptions of sense data, we cannot �know�
anything about external objects, even our own bodies. But Hume said that we do
have a �natural belief� in the external world and causal laws.
Hume�s idea of the mind having a
�feeling� (not a reason) that leads to natural beliefs became Kant�s �second
Copernican revolution� that the mind projects �concepts of the understanding�
and �forms of perception� on the external world.
7 Hume (1748) Enquiry Concerning Human Understanding,
section XII
KANT
In Germany, Immanuel Kant�s
Critiques of Reason claimed a transcendental, non-empirical realm he called
noumenal, for pure, or a priori, reason beyond or behind the phenomena. Kant�s
phenomenal realm is deterministic, matter governed by Newton�s laws of motion.
Kant�s immaterial noumena are in the metaphysical nonempirical realm of the
�things themselves� along with freedom, God, and immortality. Kant identified
ontology not with the things themselves but, influenced by Descartes, what we
can think � and reason - about the things themselves. In either case, Kant
thought metaphysical knowledge might be impossible for finite minds.
Kant reacted to the
Enlightenment, to the Age of Reason, and to Newtonian mechanics (which he
probably understood better than any other philosopher), by accepting
determinism as a fact in the physical world, which he called the phenomenal
world. Kant�s goal was to rescue the physical sciences from the devastating and
unanswerable skepticism of David Hume, especially Hume�s assertion that no
number of �constant conjunctions� of cause and effect could logically prove
causality.
Kant called Hume�s assertion the
�crux metaphysicorum.� If Hume is right, he said, metaphysics is impossible.
Kant�s Critiques of Reason were to prove that Hume was wrong.
Neither Hume�s Idea of �natural
belief� nor Kant�s �concepts of the understanding� are the apodeictic and
necessary truths sought by metaphysicians. They are abstract theories about the
world, whose information content is validated by experiments. Hume�s idea of
the mind having a �feeling� (not a reason) that leads to natural beliefs became
Kant�s �second Copernican revolution� that the mind projects �concepts of the
understanding� and �forms of perception� on the external world.
Kant�s main change in the second
edition of the Critique of Pure Reason was an attempted refutation of this
British idealism (B 274).
He thought he had a proof of the existence of the external
world.
Kant thought it a scandal in
philosophy that we must accept the existence of material things outside
ourselves merely as a belief, with no proof.
�The only thing which might be
called an addition, though in the method of proof only, is the new refutation
of psychological idealism, and the strict (and as I believe the only possible)
proof of the objective reality of outer intuition. However innocent idealism
may be considered with respect to the essential purposes of metaphysics
(without being so in reality), it remains a scandal to philosophy, and to human
reason in general, that we should have to accept the existence of things
outside us (from which after all we derive the whole material for our
knowledge, even for that of our inner sense) merely on trust, and have no
satisfactory proof with which to counter any opponent who chooses to doubt it.�
8
Kant�s noumenal world outside of
space and time is a variation on Plato�s concept of Soul, Descartes� mental
world, and the Scholastic idea of a world in which all times are present to the
eye of God. His idea of free will is a most esoteric form of compatibilism.
Kant�s decisions are made in our souls outside of time and only appear
determined to our senses, which are governed by our built-in a priori forms of
sensible perception, like space and time, and built-in categories or concepts
of intelligible understanding.
POSITIVISMS
The motto of the information
philosopher is �beyond logic and language.� Specifically, we must show that
logical positivism and logical empiricism, whose attack on metaphysics began as
early as Auguste Compte in the early nineteenth century, have done nothing to
solve any of the deep problems about the fundamental nature of reality.
Positivism is the claim that the
only valid source of knowledge is sensory experience, reinforced by logic and
mathematics. Together these provide the empirical evidence for science. Some
see this as the �naturalizing� of epistemology.
Ernst Mach�s positivism claimed
that science consists entirely of �economic summaries� of the facts (the
results of experiments).
He rejected theories about
unobservable things like Ludwig 8 Kant (1787) Preface to Second Edition,
Critique of Pure Reason, B XL
Boltzmann�s atoms, just a few
years before Albert Einstein used Boltzmann�s own work to prove that atoms
exist.
This �linguistic turn� and
naturalizing of epistemology can be traced back to Kant and perhaps even to
Descartes. The logical positivism of Bertrand Russell and Ludwig Wittgenstein
claimed that all valid knowledge must be scientific knowledge, though science
is often criticized for �reducing� all phenomena to physical or chemical
events. The logical positivists may have identified ontology not with the
things themselves but what we can say - using concepts and language - about the
things themselves.
The idea that all knowledge can
be described by true statements began with Leibniz�s vision of a universal
ambiguity-free language based on a new symbol set, a characterica universalis,
and a machinelike calculus ratiocinator that would automatically prove all
necessary truths, true in �all possible worlds.�
In the three hundred years since
Leibniz had this vision, logical philosophers and linguistic analysts following
Gottlob Frege have sought those truths in the form of �truth-functional�
propositions and statements formulated in words, but they have failed to find
any necessarily �true� connection between words and objects.
Frege had an enormous influence
on Russell, who shared Frege�s dream of reducing mathematics, or at least
arithmetic, to logic. The great Principia Mathematica of Russell and Alfred
North Whitehead was the epitome of that attempt. It failed with the discovery of
Russell�s Paradox and later G�del�s incompleteness proof.
Russell hoped to work with the
young Ludwig Wittgenstein to develop the �logical atoms,� the simplest
propositions, like �red, here, now,� upon which more complex statements could
be built. He saw the major problems of philosophy as problems of language and
logic, that complete understanding of the natural world could be obtained
through a complete set of logical propositions.
Wittgenstein�s Tractatus
Logico-Philosophicus was the height of logical positivism - the idea that all
knowledge, including all science, can be represented in logically true
statements or propositions. The Tractatus includes the first hint of its own
failure, with its dark comments about how little can be said.
��The totality of true
propositions is the total natural science (or the totality of the natural
sciences).� 9
�We feel that even if all
possible scientific questions be answered, the problems of life have still not
been touched at all.� 10
Logical positivists and the logical
empiricists of the Vienna Circle not only asserted that all knowledge is
scientific knowledge derived from experience, i.e., from verifiable
observations, they also added the logical analysis of language as the principal
tool for solving philosophical problems. They divided statements into those
that are reducible to simpler statements about experience and those with no
empirical basis. These latter they called �metaphysics� and �meaningless.�
While language is too slippery
and ambiguous to serve as a reliable tool for philosophical analysis,
quantitative information, which underlies all language use, is such a tool.
Logical positivists and
empiricists mistakenly claim that physical theories can be logically deduced
(or derived) from the results of experiments. A second flaw in all empiricist
thinking since Locke et al. is the mistaken idea that all knowledge is derived
from experience, written on the blank slate of our minds, etc. In science, this
is the flawed idea that all knowledge is ultimately experimental. To paraphrase
Kant and Charles Sanders Peirce, theories without experiments may be empty, but
experiments without theories are blind.
By contrast, the modern
hypothetical-deductive method of science maintains that theories are not the
logical (or inductive) consequences of experiments. As Einstein put it, after
shaking off his early enthusiasm for Mach�s positivistic ideas, theories are �free
inventions of the human mind.� Theories begin with hypotheses, mere guesses,
�fictions� whose value is shown only when they can be confirmed by the results
of experiments. Again and again, theories have predicted behaviors in as yet
untested physical conditions that have surprised scientists, often suggesting
new experiments that have extended the confirmation of theories, which again
surprise us. As pure information, scientific knowledge is far beyond the
results of experiments alone.
9 Wittgenstein (1922) Tractatus Logico-Philosophicus, 4.11
10 Ibid, 6.52
LINGUISTIC ANALYSIS
The central figure in the transition
from logical empiricism to linguistic analysis was Ludwig Wittgenstein.
Modern anglo-american
metaphysicians think problems in metaphysics can still be treated as problems
in language, potentially solved by conceptual analysis. They are today still analytical
language philosophers, despite a general failure of words to describe objects
in any deeply meaningful way. Language is too flexible, too ambiguous and full
of metaphor, to be a diagnostic tool for metaphysics.
We must go beyond logical puzzles
and language games to the underlying information contained in a concept, and in
the material things that embody the concept. And it is now transparently
obvious that the description of objects, aside from the scientific discovery of
the natural laws governing their behavior, is best done with information, with
computer simulations and dynamic animations of material objects, both inanimate
and living.
Although many metaphysicians
claim to be exploring the fundamental structure of reality, the overwhelming fraction
of their writings is about problems in analytic linguistic philosophy, that is
to say problems with words. Many questions appear to be verbal quibbles. Others
lack meaning or have no obvious truth value, dissolving into paradoxes.
Based on current practice, we can
sharpen the definition of a metaphysician to be an analytic language
philosopher who discusses metaphysical problems.
By contrast, a metaphysicist is
an information philosopher who is familiar with modern physics, chemistry, and
biology, as well as the interpretation of quantum physics. The fundamental
structure of reality today must be built on an understanding of quantum
reality.
For example, the wave function of
a quantum particle is pure information. Interpretations of quantum mechanics are
fundamentally metaphysical, problems for a metaphysicist. What are we to say
about a field of human inquiry whose problems have hardly changed over two
millennia? Metaphysicians today still analyze logic and language in the puzzles
and paradoxes that have been used for millennia to wrestle with metaphysical
problems.
Debates between metaphysicians
have changed relatively little in recent centuries, despite great advances in
human knowledge.
Most of these problems are the
result of assuming that the contents of the universe are pure material. They
depend on the idea that material alone constitutes complete knowledge - the
identity � of any physical thing.
Analytic language philosophers
are largely materialist, even eliminative materialists, many denying the
existence of mind, for example. They are also mostly determinist, denying the
existence of alternative possibilities in our actual universe, while investing
a great deal of their energy in the study of inaccessible possible worlds (in
each of which there are also no possibilities, only actuality).
The new light thrown by
information philosophy on many metaphysical problems, puzzles, and paradoxes
comes from establishing an immaterial, yet physical, realm of ideas alongside
the material realm. No physical object is completely known without
understanding its form in terms of quantifiable information. Information
philosophy goes beyond logical puzzles and language games.
MODAL LOGIC
Although the modes of necessity,
possibility, and impossibility had been part of Aristotelian logic (indeed,
even future contingency was analyzed), Gottlob Frege�s logic of propositional
functions included only one mode - simple affirmation and denial of statements
and the universal and existential quantifiers. Bertrand Russell�s Principia
Mathematica followed Frege and ignored other modalities.
Although the Scholastics
considered some questions of modality, it was the Harvard logician C.I. Lewis
who advanced beyond Aristotle and developed the first modern version of modal
logic. He wrote two textbooks, A Survey of Symbolic Logic in 1918 and Symbolic
Logic, written with C. H. Langford, in 1927.
Lewis was critical of the
Principia for its non-intuitive concept of �material implication,� which allows
irrelevant, even false premises p to imply any true consequences. Lewis
proposed that implication must include �intensional� and meaningful, even
causal, connections between antecedents and consequences, a revision he called
�strict implication.�
Lewis�s inclusion of intension
(meaning) was criticized by Willard Van Orman Quine, who thought symbolic logic
should be limited to �extensional� arguments, based on the members of classes
in a set theory basis for logic. In Quine�s 1943 article, �Notes on Existence
and Necessity,� (revised to appear ten years later as part of the chapter
�Reference and Modality� in his landmark book From a Logical Point of View,
Quine saw no need for �intensional� statements in mathematics. Truth values are
all that are needed, he says �These latter are intensional compounds, in the
sense that the truth-value of the compound is not determined merely by the
truth-value of the components...any intensional mode of statement
composition...must be carefully examined in relation to its susceptibility to
quantification...It is known, in particular, that no intensional mode of
statement composition is needed in mathematics.� 11
Quine saw the need for serious
restrictions on the significant use of modal operators.12 Just three years
later, Ruth Barcan Marcus, publishing under her maiden name Ruth C. Barcan,
added a modal axiom for possibility to the logical systems S2 and S4 of C.I.
Lewis.
Lewis was pleasedwith her work, although by that time, he
had given up his own work on logic.
Quine, however, reacted
negatively to Marcus�s suggestion in 1946 that modal operators (Lewis�s diamond
�◊� for possibly, and a box �☐ for �necessarily� suggested
by Barcan�s thesis adviser, F. B. Fitch) could be
transposed or interchanged with universal and existential quantification
operators (an inverted A �∀�
for �for all�
and a reversed E �∃�
for �for some�),
while preserving the truth values of the statements or propositions.
Marcus asserted the commuting of
quantification and modal operators in what A.N. Prior called the �Barcan
formulas.�
∀x ☐Fx ⊃
☐ ∀x Fx. ∀x
◊Fx ⊃ ◊
∀x
Fx.
∃x ☐Fx ⊃
☐∃x Fx. ∃x ◊Fx⊃
◊∃x Fx.
11 Quine (1943) �Notes on Existence and Necessity,� in
Journal of Philosophy, 40
p.123-125
12 Ibid., p,127
In his 1943 article, Quine had
generated a number of apparently paradoxical cases where truth value is not
preserved when �quantifying into a modal context.� But these can all be
understood as a failure of substitutivity for putatively identical entities.
Information philosophy has shown
that two distinct expressions that are claimed to be identical are never
identical in all respects. So a substitution of one expression for the other
may not be identical in the relevant respect. Such a substitution can change
the meaning, the intension of the expression. Quine called this �referential
opacity.� This is a problem that can be solved with unambiguous references.
Frege had insisted that we must
look past the reference or designator (his �Bedeutung) to the sense (�Sinn�) of
the reference, which is just what Lewis was attempting to do with his attempted
addition of intension and �strict� implication...
Perhaps Quine�s most famous
paradox of referential opacity is this argument about the number of planets:
�(1) 9 is necessarily greater than 7 for example, is
equivalent to
�9 > 7� is analytic and is therefore true (if we
recognize the reducibility of mathematics to logic)...� 13
Given, say that
(2) The number of planets is 9, we can substitute �the
number of planets� from the non-modal statement (2) for �9� in the modal
statement (1) which gives us the false modal statement
(3) The number of planets is necessarily greater than 7.
But this is false, says Quine, since the statement
(2) The number of planets is 9 is true only because of
circumstances outside of logic.
Marcus analyzed this problem in 1961, which she called the
�familiar example,�
13 Quine (1943) �Notes on Existence and Necessity,� p.121
��(27) 9 eq the number
of planets is said to be a true identity for which substitution fails in
(28) ☐(9 > 7) for it leads
to the falsehood
(29) ☐(the number of planets
> 7).
Since the argument holds (27) to
be contingent (~☐(9 eq the number of
planets)), �eq� of
(27) is the appropriate analogue of material equivalence and consequently the
step from (28) to (29) is not valid for the reason that the substitution would
have to be made in the scope of the square.� 14
The failure of substitutivity can
be understood by unpacking the use of �the number of planets� as a purely designative
reference, as Quine calls it.
In (27), �the number of planets�
is the empirical answer to the question �how many planets are there in the
solar system?� It is not what Ruth Barcan Marcus would call a �tag� of the
number 9. The intension of this expression, its reference, is the
�extra-linguistic� fact about the current quantity of planets.
The expression �9� is an
unambiguous mathematical (logical) reference to the number 9. It refers to the
number 9, which is its meaning (intension).
We can conclude that (27) is not
a true identity, unless before �the number of planets� is quantified, it is
qualified as �the number of planets qua its numerosity, as a pure number.�
Otherwise, the reference is �opaque,� as Quine describes it. But this is a
problem of his own making.
As Marcus says, when we recognize
(27) as contingent, ~☐ (9 eq the number of
planets), it is not necessary that 9 is equal to the number of planets, its
reference to the number 9 becomes opaque.
The substitution of a possible or
contingent empirical fact that is not �true in all possible worlds� for a
logical-mathematical concept that is necessarily true is what causes the
substitution failure.
When all three statements are �in
the scope of the square� (☐), when all have the same
modality, we can �quantify into modal con- 14 Marcu
(1961) Modalities and Intensional Languages,� p.
313 texts,� as Quine puts it. Both
expressions, �9� and �the number of planets, qua its numerosity,� will be
references to the same thing, They will be identical in one respect, qua
number. They will be �referentially transparent.�
The Necessity of Identity In her
third article back in 1947, �The Identity of Individuals,� Barcan had first
proved the necessity of identity. This result became a foundational principle
in the modern incarnation of Leibniz�s �possible worlds� by Saul Kripke and
David Lewis.
Her proof combined a simple substitution of equals for
equals and Leibniz�s Law.
Quine described this in his 1953 �Reference and Modality�
(p.153) as in the form
(x)(y) (x = y) ⊃ ☐
(x = y), reading �for all x and for all y, if �x = y,� then necessarily �x = y.�
Quine found this relationship in
the 1952 textbook, Symbolic Logic, by F. B. Fitch, who was Ruth Barcan�s thesis
adviser. Although Fitch mentions her work in his foreword, he does not
attribute this specific result to her where he presents it. His proof is based
on the assumption of substitutability, which he calls �identity elimination.�
23.4 (1) a = b, (2) ☐[a = a], then (3) ☐[a
= b], by identity elimination.15
Then in 1961, Marcus published a very brief proof of her
claim, using Leibniz�s Law relating identicals to indiscernibles.
�In a formalized language, those
symbols which name things will be those for which it is meaningful to assert
that I holds between them, where �I � names the identity relation... If �x� and
�y� are individual names then (1) x I y
Where identity is defined rather than taken as primitive, it
is customary to define it in terms of indiscernibility, one form of which is
(2) x Ind y =df (φ)(φx eq φy)� 16
15 Fitch (1952) Symbolic Logic, p.164
16 Marcus (1961) Modalities and Intensional Languages,� p.
305
Statement (2) says that the indiscernibility of x from y, by
definition means that for every property φ, both x and y have that same
property, φx eq φy.
A few years after Marcus� 1961 presentation, David Wiggins
developed a five-step proof of the necessity of identity, using Leibniz�
Law, as had Marcus. He did not mention her.
DAVID WIGGINS ON IDENTITY
David Wiggins and Peter Geach debated back and forth about
the idea of �relative identity� for many years after Geach suggested it in
1962.
Ruth Barcan Marcus published her original proof of the
necessity of identity in 1947 and repeated her argument at a 1961 Boston
University colloquium.
Whether Wiggins knew of Marcus�s 1961 presentation is not
clear.
He should have known of her 1947
paper, and his work is similar to her 1961 derivation (which uses Leibniz�s
Law). Wiggins gives no credit to Marcus, a pattern in the literature for the
next few decades and still seen today ignoring the work of female philosophers.
Saul Kripke clearly modeled much of his four-step derivation
after Wiggins, especially his criticism of the derivation as �paradoxical�.
Kripke gives no credit to either
Marcus or Wiggins for the steps in the argument, but his quote from Wiggins,
that such a claim makes contingent identity statements impossible, when they
clearly are possible, at least tells us he has read Wiggins. And we know Kripke
heard Marcus�s presentation at the 1961 B. U. colloquium.
Here is Wiggins in 1965,
�I WANT to try to show (i) that
there are insuperable difficulties any term + relation + term or subject +
predicate analysis of statements of identity, (ii) that, however important and
helpful the sense-reference distinction is,1 this distinction does not make it
possible to retain the relational or predicative analysis of identity
statements, and (iii) that a realistic and radically new account is needed both
of � = � and of the manner in which nounphrases occur in identity-statements.
Till we have such an account many questions about identity and
individuation will be partly unclear, and modal logics will continue without
the single compelling interpretation one might wish.
The connexion of what I am going to
say with modal calculi can be indicated in the following way. It would seem to
be a necessary truth that if a = b then whatever is truly ascribable to a is
truly ascribable to b and vice versa (Leibniz�s Law). This amounts to the
principle (1) (x)(y)((x = y) ⊃ (φ)(φx ⊃ φy))
Suppose that identity-statements are ascriptions or
predications.!
Then the predicate variable in (1) will apparently range
over properties like that expressed by �( = a)�2 and we shall get as
consequence of (1)
(2) (x) (y) ((x = y) ⊃ (x = x . ⊃
. y = x))
There is nothing puzzling about this. But if (as many modal
logicians believe), there exist de re modalities of the form
☐ (φa) (i.e.,
necessarily (φa)), then something less innocent follows. If �( = a ) �
expresses property, then �☐ (a=a)�, if this too is about the object a, also ascribes something
to a, namely the property ☐ ( = a). For on a naive
and pre-theoretical view of properties, you will reach an expression for a
property whenever you subtract a noun-expression with material occurrence
(something like � a � in
this case) from a simple declarative sentence. The property ☐
( = a) then falls within the range of the predicate variable in Leibniz�s Law (understood in this intuitive way) and we get (3) (x)
(y) (x = y ⊃ (☐ (x = x). ⊃.
☐(y = x)))
Hence, reversing the antecedents, (4) (x) (y) (☐
(x = x). ⊃. (x = y) ⊃ ☐(x
= y))
But (x) ( ☐ (x=x)) � is a necessary truth, so we can drop this antecedent and
reach
(5) (x)(y)((x = y). ⊃ . ☐(x
= y))
Now there undoubtedly exist contingent identity-statements.
Let �a = b� be one of them. From its simple truth and (5) we
can derive �☐(a = b)�.
But how then can there be any contingent identity-statements?...
1 G. Frege, �On Sense and
Reference �, Translations from the Philosophic Writings of Gottlob Frege, ed.
P. T . Geach and M. Black (Oxford, 1952), pp. 56-4]
2 Quotation marks are used under
the convention that they serve to form a designation of whatever expression
would result in a particular case from rewriting the expression within the
quotation-marks with genuine constants in the place of free variables and
dummy-expressions.� 17
Saul Kripke on Identity Kripke
does not cite Wiggins directly as the source of the argument, but just after
his exposition above, Kripke quotes David Wiggins as saying in his 1965
�Identity-Statements�
Now there undoubtedly exist
contingent identity-statements. Let a = b be one of them. From its simple truth
and (5) [= (4) above] we can derive �☐( a = b)�. But how then can there be any contingent identity
statements?18
Kripke goes on to describe the
argument about b sharing the property � = a� of being identical to a, which we
read as merely selfidentity, and so may Kripke.
�If x and y are the same things
and we can talk about modal properties of an object at all, that is, in the
usual parlance, we can speak of modality de re and an object necessarily having
certain properties as such, then formula (1), I think, has to hold. Where x is
any property at all, including a property involving modal operators, and if x
and y are the same object and x had a certain property F, then y has to have
the same property F. And this is so even if the property F is itself of the
form of necessarily having some other property G, in particular that of
necessarily being identical to a certain object. [viz., = x]
Well, I will not discuss the
formula (4) itself because by itself it does not assert, of any particular true
statement of identity, that it is necessary. It does not say anything about
statements at all. It says for every object x and object y, if x and y are the
same object, then it is necessary that x and y are the same object.
And this, I think, if we think
about it (anyway, if someone does not think so, I will not argue for it here),
really amounts to something very little different from the statement (2). Since
17 Wiggins (1965) Identity Statements,� in Analytical Philosophy pp.40-41
18 Kripke (1971) �Identity and Necessity,� p. 136
x, by definition of identity, is
the only object identical with x, �(y)(y = x ⊃ Fy)�
seems to me to be little more than a garrulous way of saying �Fx� and thus (x) (y)(y = x ⊃
Fx) says the same as (x)Fx no matter what �F� is � in particular, even if �F� stands for the property of
necessary identity with x. So if x has this property (of necessary identity
with x), trivially everything identical with x has it, as (4) asserts. But,
from statement (4) one may apparently be able to deduce various particular
statements of identity must be necessary and this is then supposed to be a very
paradoxical consequence.� 19
The indiscernibility of
identicals claims that if x = y, then x and y must share all their properties,
otherwise there would be a discernible difference. Now Kripke argues that one
of the properties of x is that x = x, so if y shares the property of �= x,� we
can say that y = x.
Then, necessarily, x = y.
However, two distinct things, x
and y, cannot be identical, because there is some difference in extrinsic
external information between them. Instead of claiming that y has x�s property
of being identical to x (�= x�) , we can say only that y has x�s property of
being selfidentical, thus y = y. Then x and y remain distinct in at least this
intrinsic property as well as in extrinsic properties like their distinct
positions in space.
DAVID LEWIS ON IDENTITY
David Lewis, the modern metaphysician who built on Leibniz�
possible worlds to give us his theory of �modal realism,� is just as clear as
Leibniz on the problem of identity.
�[W]e should not suppose that we have here any problem about
identity. We never have. Identity is utterly simple and unproblematic.
Everything is identical to
itself; nothing is ever identical to anything else except itself. There is
never any problem about what makes something identical to itself, nothing can
ever fail to be. And there is never any problem about what makes two things
identical; two things never can be identical.� 20
Except, says an information philosopher, �in some respects.�
19 Kripke (1971) �Identity and Necessity,� p. 137-138
20 Lewis (1988) �Counterparts or Double Lives,� On the
Plurality of Worlds, p.192
MODAL LOGIC AND POSSIBLE WORLDS
In the �semantics of possible
worlds,� necessity and possibility in modal logic are variations of the
universal and existential quantifiers of non-modal logic. Necessary truth is
defined as �truth in all possible worlds.� Possible truth is defined as �truth
in some possible worlds.� These abstract notions about �worlds� � sets of
propositions in universes of discourse � have nothing to do with physical
possibility, which depends on the existence of real contingency.
Propositions in modal logic are required to be true or
false. Contingent statements that are neither true or false are not allowed. So
much for real possibilities, which cannot be based on truths in some possible worlds.
Historically, the opposition to
metaphysical possibility has come from those who claim that the only possible
things that can happen are the actual things that do happen. To say that things
could have been otherwise is a mistake, say eliminative materialists and
determinists.
Those other possibilities simply never existed in the past.
The only possible past is the past we have actually had.
Similarly, there is only one
possible future. Whatever will happen, will happen. The idea that many different
things can happen, the reality of modality and words like �may� or �might� are
used in everyday conversation, but they have no place in metaphysical reality.
The only �actual� events or things are what exists. For �presentists,� even the
past does not exist. Everything we remember about past events is just a set of
�Ideas.� And philosophers have always been troubled about the ontological
status of Plato�s abstract �Forms,� entities like the numbers, geometric
figures, mythical beasts, and other fictions.
Traditionally, those who deny possibilities in this way have
been called �Actualists.�
In the last half-century, one might think that metaphysical
possibilities have been restored with the development of modal logic.
So-called modal operators like
�necessarily� and �possibly� have been added to the structurally similar
quantification operators �for all� and �for some.� The metaphysical literature
is full of talk about �possible worlds.�
�The most popular theory of �possible worlds�
is David Lewis�s �modal realism,� an infinite number of worlds, each of which
is just as actual (eliminative materialist and determinist) for its inhabitants
as our world.
It comes as a shock to learn that every �possible world� is
just as actual, for its inhabitants, as our world is for us. There are no
alternative possibilities, no contingency, that things might have been
otherwise, in any of these possible worlds. Every world is as physically
deterministic as our own.
Modal logicians now speak of a
�rule of necessitation� at work in possible world semantics. The necessarily
operator � ☐ � and the
possibly operator � ◊
� are said to be �duals� - either one can be defined in terms of the other (☐
= ~◊~, and ◊
= ~☐~), so either can be primitive. But most
axiomatic systems of modal logic appear to privilege necessity and de-emphasize
possibility. They rarely mention contingency, except to say that the necessity
of identity appears to rule out contingent identity statements.
The rule of necessitation is that �if p, then necessarily
p,� or p ⊃ ☐p.
It gives rise to the idea that if anything exists, it exists
necessarily.
This is called �necessitism.� The
idea that if two things are identical, they are necessarily identical, was
�proved� by Ruth Barcan Marcus in 1947, by her thesis adviser F.B. Fitch in
1952, and by Willard Van Orman Quine in 1953. David Wiggins in 1965 and Saul
Kripke in 1971 repeated the arguments, with little or no reference to the
earlier work.
This emphasis on necessitation in
possible-world semantics leads to a flawed definition of possibility that has
no connection with the ordinary and technical meanings of possibility.
Modal logicians know little if
anything about real possibilities and nothing at all about possible physical
worlds. Their possible worlds are abstract universes of discourses, sets of
propositions that are true or false. Contingent statements, that may be true or
false, like statements about the future, are simply not allowed.
They define necessary
propositions as those that are �true in all possible worlds.� Possible
propositions are those that are only �true in some possible worlds.� This is
the result of forcing the modal operators ☐ and ◊ to correspond to the universal and existential
quantification operators for all ∀ and for some ∃.
But the essential nature of possibility is the conjunction of contingency and
necessity.
Contingency is not impossible and not necessary (~~◊
˰ ~☐).
We propose the existence of a metaphysical possibilism
alongside the notion necessitism.
�Actual possibilities� exist in
minds and in quantum-mechanical �possibility functions� It is what call �actual
possibilism,� the existence in our actual world of possibilities that may never
become actualized, but that have a presence as abstract entities that have been
embodied as ideas in minds. In addition, we include the many possibilities that
occur at the microscopic level when the quantummechanical probability-amplitude
wave function collapses, making one of its many possibilities actual.
Actual possibles can act as causes when an agent chooses one
as a course of action.
Why Modal Logic Is Not
Metaphysics Modal logicians from Ruth Barcan Marcus to Saul Kripke, David
Lewis, and the necessicist Timothy Williamson are right to claim metaphysical
necessity as the case in the purely abstract informational world of logic and
mathematics. But when information is embodied in concrete matter, which is
subject to the laws of quantum physics and ontological chance, the fundamental
nature of material reality is contingent and possibilist.
There are two reasons for the
failure of modal logic to represent metaphysical reality. The first is that
information is vastly superior to language as a representation of reality. The
second is that truths and necessity cannot be the basis for metaphysical
possibility.
Possible world semantics is a way of talking about universes
of discourse - sets of true propositions - that considers them �worlds.�
It may be the last gasp of the
attempt by logical positivism and analytic language philosophy to represent all
knowledge of objects in terms of words.
Ludwig Wittgenstein�s core idea
from the Tractatus had the same goal as Gottfried Leibniz�s ambiguity-free
universal language, The totality of true propositions is the total natural
science (or the totality of the natural sciences).21
Information philosophy has shown
that the meaning of words depends on the experiences recalled in minds by the
Experience Recorder and Reproducer. Since every human being has a different set
of experiences, there will always be variations in meaning about words between
different persons, as Gottlob Frege pointed out.
The goal of intersubjective
agreement in an open community of inquirers hopes to eliminate those
differences, but representation of knowledge in words will always remain a
barrier and source of philosophical confusion. The physical sciences use
analytic differential equations to describe the deterministic and continuous
time evolution of simple material objects, which is a great advance over
ambiguous words. But these equations fail at the quantum level and where
discrete digital messages are being exchanged between biological interactors.
Moreover, while mathematical methods are precise, their significance is not
easily grasped.
The very best representation of
knowledge is with a dynamic and interactive model of an information structure,
what Wittgenstein imagined as a �picture of reality.� Today that is a
three-dimensional model implemented in a digital computer with a
high-resolution display, even a virtual reality display. While computer models
are only �simulations� of reality, they can incorporate the best �laws� of
physics, chemistry, and biology. And since computer models are pure
information, abstract ideas, they seem �beyond physical� and reaching the
metaphysical.
Sadly, modal logicians have never
proposed more than a handful of specific propositions for their possible
worlds, and many of these generated controversies, even paradoxes, about
substitutivity of presumed identicals in modal contexts. Word and object have
degenerated to words and objections. By comparison, molecular models of the
biological machines that have evolved to keep us alive and let us think can be
�shown,� not said, as Wittgenstein imagined.
21 Wittgenstein (1922) Tractatus Logico-Philosophicus, 4.11
His later work can be summed up
as the failure of language to be a picture of reality. Information philosophy
gives us that picture, not just a two-dimensional snapshot, but a lifelike
animation and visualization of the fundamental nature of metaphysical reality.
Our information model
incorporates the irreducible ontological chance and future contingency of
quantum physics. The claimed �necessity of identity,� and the �necessary a posteriori�
of natural and artificial digital �kinds� with identical intrinsic information
content are just more �ways of talking.� There is no necessity in the physical
world.
Truths and necessity are ideal concepts �true in all
possible worlds,� because they are independent of the physical world. They have
great appeal as eternal ideas and �outside space and time.�
Possible worlds semantics defines
necessity as �propositions true in all possible worlds� and possibility as
�propositions true in some possible worlds.� There is no contingency here, as
the only allowed propositions are either true or false. Modal logicians have
little knowledge of our actual physical world and zero factual knowledge, by
definition, of other possible worlds. The possible worlds of �modal realism�
are all actual worlds, deterministic and eliminatively materialist. There are
no possibilities in possible worlds, even in the �many worlds� of physics.
A necessicist metaphysics is only
a half-truth. Without metaphysical possibility, we cannot account for the
information in the universe today, nor can we explain the cosmic, biological,
and human creation of new information in our free and open future.
Necessitism and possibilism are perhaps another congruence
with the great duals of idealism and materialism.
THE RETURN OF METAPHYSICS AND ITS PARADOXES
In the last few decades,
metaphysicians have celebrated the failures of logical positivists and logical
empiricists, especially their loud claims that metaphysics is nonsense or
meaningless.
The sad failure of analytic language philosophy to solve any
meaningful problems in philosophy has also encouraged a number of philosophers
to return to metaphysical questions.
But can they make any progress on
the fundamental nature of reality if their tools are still only logic and
language analysis? The information philosopher thinks not. We must go beyond
logical puzzles and language games to underlying information structures.
Now academic philosophers have
never failed to teach all the classic problems, paradoxes, and puzzles, mostly
presenting them as insoluble, which gives them a form of job security, but this
must be discouraging for would-be future philosophers.
The well-known lack of progress
in philosophy compared to the advances in knowledge made in the sciences is
more than an embarrassment, it is in some cases a scandal, as the information
philosopher has tried to show.
Even in the sciences, the deference shown to philosophers by
the special sciences, when it comes to the fundamental nature of reality, has
held back those sciences.
Notably, the deep belief in
natural laws that are deterministic has held back the essential role of chance
in physics and biology. The claims of eliminative materialism have held back
progress on the mind-body problem and the free will problem in psychology.
Indirectly caused by philosophical
views, these are scandals in the special sciences themselves. The philosophical
notion that many genuine problems about reality must be taught as mysteries,
not only paradoxes and puzzles, is a disservice to generations of students, who
come away not only confused, but ill-informed.
Consider these negative comments from a recent important
study of metametaphysics, the foundations of metaphysics itself.
�When one is first introduced to
a dispute that falls within the purview of metaphysics � or perhaps even after
years of thinking hard about it � one can experience two sorts of deflationary
intuitions. First one may sense that nothing is really at issue between the
disputants. The phenomenology here resembles that of countering merely �verbal�
or �terminological� disputes in ordinary conversation...
We come now to the second type of
intuition that is elicited by metaphysical disputes. Even when we sense that
something might really be at issue when it comes to a question of metaphysics,
we may still get the impression that the answer is more or less trivial �it can
be known by drawing out consequences of truisms that we all accept or by
reflecting on a conceptual framework that we all share.
These two deflationary intuitions
threaten the robustly realist approach that is dominant today � at least among
analytic philosophers who specialize in metaphysics, Most contemporary
metaphysicians think of themselves as concerned, not primarily with the
representations of language and thoughts, but with the reality that is
represented.� 22
Information philosophy hopes to
reinflate metaphysics by adding back the immaterial ideas that have been
eliminated by naturalists and materialists, with their claims that the world is
causally closed.
Information physics shows that the universe is open,
continually expanding and generating creative new possibilities for the future.
Careful analysis of the
information content (the abstract form that shapes a concrete object, arranging
its parts) has given us plausible solutions for several classic paradoxes and
puzzles in metaphysics.
Information is neither matter nor energy, although it needs
matter for its embodiment and energy for its communication. It is immaterial.
It is the modern spirit, the ghost in the machine.
Living things use information to control the flows of matter
and energy through their bodies. Information is the mind in the body.
It is the soul. And when we die, our personal information
and its communications perish. The matter remains.
(back
to content)
4.1.1 Spiritual Medicine w
Constructing and deconstructing the terminology of spirit: a
journey back to the Greek roots
ABSTRACT
Over the past few decades,
literature related to spirituality presents rising interest within researchers.
Many tried to encode the term but there is not a widely agreed definition of
spirituality. My interest in investigating the terminology led me to some
hypothesis. Τhe antiquity of the word must be important in order to understand
how the word was originally used. The purpose of this short communication is
giving flesh to the notion of spirituality as it goes into the heart of Ancient
Greek philosophy in order to encode the term. A large body of literature
acknowledges the connectedness between spirituality and the Greek word
πνεύμα (pneuma) which means spirit, mind, soul,
and breathing. The semantic root of the English term spirituality is the Latin
word spirare which meant to breathe, to blow and to live. Spirituality does
elicit an experiential sense by force of the words� own signification and
etymology. Based on the definitions of spirit outlined in this manuscript; the
spirit animates not only human beings but all beings. This analysis shows that
since �air� is an extension of breath, spirituality must possibly be as vital
as the air we breathe. It must be our �Breath of Life�. Air has also been
ascribed divine attributes, so spirituality could also be the �Breath of God�.
This �Breath� could help people understand answers to ultimate questions about
life, about meaning and about the relationship to the sacred, the transcendent,
and the Divine.
INTRODUCTION
Over the past few decades,
literature related to spirituality presents rising interest within researchers.
The role and meaning of spirituality has been discussed in various worldwide
publications. Many tried to encode the term but there is not a widely agreed
definition of spirituality. When discussing about this debate Dreyer and
Bennett (2006) very aptly say �� there is also the issue of definition. There
are hundreds from which to choose�. The word of spirituality is on countless
lips today. A religious language usually refers to the notion of spirituality
as to what is not material; several metaphors are also used in order to define
the term; the dualistic view of matter and spirit seems to have influenced
several other researchers; philosophical paradigms are still trying to capture
the definition; while a universal approach of the term that touches upon us all
also attempts to lead a path. No borders exist and so this debate can proceed
incessantly.
Due to this large number of
definitions and approaches an unresolved question still remains to be answered.
What is spirituality? For someone unfamiliar with the term things get even more
confusing. People might have heard about spirituality but are not really sure
what it is. Many researchers have the desire to attribute a universal essence
to the meaning of spirituality. Sometimes this desire ignores the historical
and cultural traces and differences in the uses of the term. Spirituality is
not an invention of these last few decades. Kielkiewicz and Dalzell (2014)
stated that spirituality was known and practiced by generations of people down
through the ages. According to Miner-Williams (2006) spirituality has been
discussed since the earliest of times, and many hundreds of philosophies have
explored this phenomenon. The phenomenon is used and understood very
differently in today�s context in comparison to its original root. �Currently,
there is no �gold standard� for the definition of spirituality that can be
established independent of the historical use of the term in the English
language or the Greek or Latin roots from which the word �spirituality� is
derived�.
Two recent researches on Greek
Chronic Obstructive Pulmonary Disease (COPD) patients and COPD caregivers
showed that the antiquity of the word (Greek:
πνεύμα) could be important in order to understand
how it was originally used. My interest in investigating this kind of cognition
led me to some hypothesis. I am not aware if there is �some kind of ancient
�authentic� or �true� spirituality� but I believe that in order to encode the
term we must go back to Ancient Greeks ways of thinking. There were we can
actually identify the root of the word spirituality.
AIM
The purpose of this short
communication is giving flesh and historical grounding to the notion of
spirituality. It mainly goes into the heart of Ancient Greek philosophy in
order to encode the term. It is based on a detailed search of work published in
the database of Pubmed and Google Scholar using terms that included
spirituality, spirit, Ancient Greek and Roman philosophy, religiosity, air, and
breath. Maybe this analysis could help readers come closer to the original
meaning of the word while trying to explain the phenomenon of spirituality.
CONSTRUCTING AND DECONSTRUCTING SPIRITUALITY
Many researchers try to use
shortened or narrower definitions in order to decode spirituality. Spirituality
has been described as a variable of holism as it involves a sense of
connectedness to other people, nature, and life as a whole. Moving away from
this holistic perspective one �may cut of spirituality from the half of its
body�. Waaijman also wonders ��whether this intense interest is not a
Procrustes bed�.
Holistic spirituality is a
necessity for our postmodern world. Holism comes from the word �whole� which is
perceived in multiple meanings such as the entire, total, undivided, undamaged,
or a complete entity. The word �whole� comes from the Greek word
�όλος�. This totality of the terminology was probably
captured from Anaximenes. Anaximenes
(Άναξιμένης: in Greek) of
Miletus (c. 585�528 B.C.E.) was a pre- Socratic Greek philosopher. Anaximenes
is best known for his doctrine that air is the source of all things. He
proposed air as the First Cause from which all else comes and conceived �air�
as an extension of breath.
Joshua Mark states that �to the
Greeks of the time, air was comparable to soul and, just as one�s breath gave
an individual life, so air, Anaximenes claimed, gave life to all observable
phenomena�. While describing the same phenomenon it is stated that �by �air,�
Anaximenes meant some original element that can give life (breath or soul) to
human beings.
Some may wonder about how all
these are related to spirituality. Hence, why not start unfolding Ariadne�s
mite. Carrette and King identify that although the term �spirituality�
developed from earlier Greek and Latin roots, there are significant dimensions
to these earlier uses that are lost once one defines the spiritual in narrowly
privatized terms.
I believe that spirituality leads
on to its own ancient path; it is not a trend that changes yearly. Did this
�genuine� or �ancient� spirituality come from the transfiguration of a
previously existed spirituality? Probably not, it proved its existence
incessantly and it still is.
A large body of literature
acknowledges the connectedness between spirituality and the Greek word
πνεύμα (pneuma). The Greek term
πνεύμα (pneuma) reveal the linguistic root of the
word.
The Greek word for spirituality
is �pneumatikotita�
(=πνευματικότητα).
Πνευματικότητα
comes from the Greek word πνεύμα (pneuma) which
means spirit, mind, soul and breathing. The root πνευ-
talked about the dynamic movement of air describing a person�s breath, which
meant they were alive (breath equals life). Pneuma, �air in motion, breath,
wind,� is equivalent to aer (ἀήρ, �air�) as the element from
which all else originated. Anaximenes concept of �air,� seems to explain both
spiritual and physical phenomena. �Οἷον ἡ
ψυχὴ ἡ ἡμετέρα ἀὴρ
οὖσα συγκρατεῖ
ἡμᾶς, καὶ ὅλον
τὸν κόσμον πνεῦμα
καὶ ἀὴρ περιέχει�
[(Αέτ. I 3, 4 (D. 278)]. (= Just as our soul (psyche), being air
(aer), holds us together, so do breath (pneuma) and air (aer) encompass the
whole world.
Based on the definitions of spirit outlined above; it seems
that for the Greeks, spirit animates not only human beings but all beings.
In the classical societies of
Greece and Rome, spirituality also maintained a central place. Breath was also
associated with �soul,� the source of life, in many ancient cultures, including
the Romans. The modern English term �spirituality� refers to spirit and comes
from the Latin spiritualitas. Spiritualitas springs from the noun spiritus
which means �the breath of life�. The semantic root of spiritus is the word
spirare which meant to breathe, to blow and to live.
It seems that spirituality does
elicit an experiential sense by force of the words� own etymology and
signification.
If we suppose that spirituality
is all around us, as air, is it then, possible to see the affect this
�phenomenon�? First and foremost, someone will argue that we cannot see
spirituality. Maybe this statement is not quite true because I personally
believe that we must conceive spirituality both outside and inside the
boundaries of our senses.
Spirituality was strongly associated with air. �Air can be
thought of as a kind of neutral stuff that is found everywhere, and is
available to participate in physical processes�.
In Hermes Trismegistus we can
read the following dialogue between Hermes and Asclepius talking about air.
-Hermes. Is not the air a body?
-Asclepius. A body it is�. The air is body, and this is the
body which permeates through all the entities, and permeating fills all
tilings.
Spirituality was strongly
associated with breath and breathing. Our daily reality is both spiritual and
material. Breathing for example is the most basic of the voluntary behaviors of
living beings and it requires no volition at all. Fontana progresses to discuss
breathe as a force that unifies the unseen and the seen dimensions. Kourie and
Ruthenberg stated that �the earth, the body and materiality breathes with an
organic life and mystery�.
Some may wonder; are we able come
to an awareness of the mystery of God, or the Divine or find answers to
ultimate questions about life based on air and breathing? Is this approach to
simplistic to be taken under consideration?
Anaximenes ascribed to air divine
attributes. He wrote the Gods and the Divine derived from air. With the spread
of Christianity and its concept of the Holy Spirit, spirit and spirituality became
associated with a religion. It seems that most religions endeavour to inculcate
a sense of the spirituality in their believers. Christians for instance have
thought of the Holy Spirit as �the breath of God�. The Book of Genesis depicts
the Spirit of God at the beginning of creation as a wind. The words wind and
breath are linked together as God breathes life into Adam. �... And the Lord God
formed a man�s body from the dust of the ground and breathed into it the breath
of life. And the man became a living person.� (Genesis 2, 2).
Nowadays, there are many ways that people describe
spirituality. Assembling my thoughts on this topic I asked myself, �Is it may
be time to tighten the definition?�
I may take a risk but I would
like to give a brief reference of some characteristics which I believe could be
possibly accounted to spirituality. I will also try to convey some ideas on the
effect of spirituality on people�s lives.
1. Spirituality takes its place in the world of every-day
experience.
2. Spirituality is not static; it changes forms and shapes,
it �flaws� around us, affecting and changing our daily lives.
3. Spirituality is an inexhaustible source.
4. Spirituality has no center, edges, boundaries, or limits.
5. Spirituality is continuous. It has infinite moments and
signs since the dawn of time.
6. Spirituality requires no volition but gives us back
everything.
7. Spirituality is our �inner guardian� because is as vital
as breath and breathing.
This �Breath� probably helps people understand answers to
ultimate questions about life, about meaning and about the relationship to the
sacred, the transcendent, and the Divine.
Since �air� is an extension of breath; spirituality must
possibly be as vital as the air we breathe.
It must be our Breath of Life.
Since air has been ascribed divine attributes; spirituality
could also be the Breath of God. So is this �Breath of God� equal (=) with the
�Breath of Life�?
Although there are numerous
modern scholars that are addressing this relationship between spirituality and
breath many may argue with this approach. Some may also wonder if this is the
only definitive meaning of spirituality and if it has to be so strict?
Questions and answers about
spirituality are not absent in other cultures, and philosophies. Spirituality
is not separated from the spheres of human and other forms of life.
Unfortunately, some key issues in Greek philosophy tend to be forgotten. I
believe that this ancient knowledge on the specific terminology could be our
leading path. There is no need to change a deeply rooted ancient belief about
spirit and spirituality by simply treating it as being too simplistic. Going
back to Ancient Greeks� ways of thinking about spiritual ideas in order to
decode the definition of spirituality is to everyone�s great benefit.
CONCLUSION
Maybe the terminology of
spirituality is confusing for many people. Different people from different
backgrounds describe spirituality differently. Diving into Greek philosophy and
exploring the antiquity of the word helps us to understand how the word was
originally used. Some of these things may not speak to you at all but there are
many reasons for exploring spirituality. Fuller understanding of the phenomenon
requires further exploration. The Greek path of spirituality could take people
on an interior journey in order to meet and connect with the Breath of their
Lives.
(back
to content)
4.1.2 CRYSTAL HEALING is a Metaphysics Diploma course w
HISTORY
The therapeutic use of crystals
is not a new or alternative healing method. The art of healing with gems is
thousands of years old. Evidence that gemstones were used to heal disease can
be found from the most ancient civilisations. They were also considered to have
protective and talismanic properties, and to keep evil spirits away.
Crystal amulets, talismans and
charms have often been found in prehistoric burial grounds. Such items were
considered essential for the wellbeing of the dead. The legendary land of
Atlantis (50 000 BC) also features prominently in crystal history. Crystals in
Atlantis were used for communication, to store energy and to provide light and
heat. The Atlanteans also kept secret records on or in quartz crystals. This,
they believed, would ensure that such records would remain intact forever, with
no risk of destruction through age or local catastrophe.
Use of crystals for healing can
be found in Sumerian writings and Indian vedic texts (4 000 BC). Vedic
naturopathic medicine is known as Ayurveda. Ayurveda also makes use of crystal
healing in the form of elixirs, pastes and powders made from gemstones. In the
first Chinese medical book, written 5 000 years ago by Shen Nung, the Red
Emperor, detailed descriptions of gemstones and their influence on the human
body can be found.
In the Bible, crystals are mentioned at least 200 times.
There are strict instructions about the crystals to be used in the breastplate
that God had instructed Moses to produce for Aaron, the priest.
In Egypt, the tomb of Tutankhamun
shows the reverence with which the ancient Egyptians regarded jewels. They
believed that, in addition to indicating the wealth and majesty of the pharaoh,
the stones possessed mystical charms to protect him in the after-life.
Tutankhamun�s sarcophagus was made of quartzite. Within the linen bandages that
swathed his body were 143 bejewelled amulets.
In the 12th Century, Hildegard
van Blingen (1098 � 1179) composed the Physika, which dealt with gemstones in a
comprehensive fashion. This lady developed entirely new ways of healing with
gems. Paracelsus (1493 � 1541) published a book called On Minerals in which he
distinguished between chemical formulae and the elemental powers that reside
within stones. Famous Greek, Roman an Arabic doctors and scholars wrote of the
power of gems, which played an important role in their methods of healing. In
the middle ages a book was published, called Liber Lapidu seu de Gemmis, which
provided an overview of sixty gems and their therapeutic properties. This book
was a bestseller and was translated into four languages. It went through
fourteen editions and was published from 1511 to 1799.
In America, both the Mayans and
Indians used crystals as a means to diagnose illness as well as to cure it.
Indians of the Cherokee tribe also used crystals for divination. Medicine men
in American Indian tribes claimed to be able to foresee the future by gazing
into the depths of large faceted crystals, just as today�s fortune tellers gaze
into crystal balls. The Mayans also used obsidian slabs to foretell the future.
(back
to content)
�
4.2 The History of Naturopathic Medicine ф
Dr. Robert F. Stern DC, CFE, ABQAURP and Mitchell Bebel
Stargrove, ND, LAc
DC, CFE, ABQAURP
Medical Director/ Allied Health, CGI
HISTORY AND ORIGINS OF NATUROPATHIC MEDICINE
Naturopathic medicine is both an
ancient and a modern tradition of medicine within the United States and Europe.
It was formed officially at the beginning of the 20th century by physicians
wishing to bring various traditions of classical and folk medicine into a
modern scientific framework. Using the foundation of core principles that
continue to define naturopathic medicine these doctors combined the best of
European and American folk herbalism, Eclectic herbal medicine, homeopathy,
hydrotherapy and hygiene, healing diets and nutrients, fasting and nature cure,
exercise and spinal manipulation. At the time of naturopathy�s birth into a
formal profession, Dr. Benedict Lust, one of its founders, declared that all
types of doctors were welcome to call themselves naturopaths as long as their
practice was consistent with these shared underlying principles.
CURRENT DEFINITION OF NATUROPATHIC MEDICINE
Today the American Association of Naturopathic
Physicians defines naturopathic medicine as a blend of centuries-old natural
non-toxic therapies with current advances in the study of health and human
systems, covering all aspects of family health from prenatal to geriatric care.
Naturopathic medicine concentrates on whole patient wellness � the medicine is
tailored to the patient and emphasizes prevention and self-care.
Naturopathic medicine attempts to
find the underlying cause of the patients� condition rather than focusing
solely on symptomatic relief. Thus, the core principles of naturopathic
medicine have generally been agreed upon as:
1. The Healing Power of Nature,
or in Latin: Vis Medicatrix Naturae, which is the fundamental observations that
our human bodies are part of nature and that the force of life itself is
healing. The ancient Greek word �physis� refers to this vital force of nature
within all living organisms and is the root for such words as physician,
physics and physique. Before the 20th century this approach to medicine was
called Vitalistic; in the language of modern science it parallels the emerging
knowledge of self-organizing processes, ecology and systems theory. Thus,
naturopathy has always focused on health as much as disease, stimulating,
enhancing and supporting your body�s inherent ability to heal as much as the
virus, bacteria, injury or illness. We know what it feels like to be vital and
vigorous. Naturopathy focuses on tapping into these deep resources and using
them to heal our illnesses and keep us well.
2. Treat the Cause, or in Latin:
Tolle Causum. Many symptoms are expressions of the body�s attempt to heal
itself and their suppression will not address the root causes of dysfunction,
illness and disease. Quite simply, treating symptoms is always important in
medicine but deep and lasting healing, the medical outcomes that we all really
seek are based on discovering the causes of dysfunction and disease and
changing them in a fundamental and lasting way. This also inherently means that
each individual needs to be treated in a unique and evolving therapeutic
process that reflects their history and physical characteristics, addresses
their weaknesses, stresses and strengths, and creates opportunities for their own
personal growth, self-discovery and transformation. Thus, a digestive problem
such as heartburn needs to be treated but opens the doorway to looking at
stress patterns, movement, tension and exercise, healing and stressful foods,
and new tools for feeling what is good for us. Treating the cause removes
blockages that have been preventing the natural healing processes from
occurring and thus unleashes our inner healing momentum and empowers us to
learn from our illnesses and difficulties to live better, stronger, healthier,
more creative lives. Preventive medicine isn�t just about reducing risks and
avoiding disease, it is really about learning to hear your body�s feedback and
discovering ways to not just feel �OK,� but to feel better.
3. Do No Harm, or in Latin:
Primum no nocere. Hippocrates declared: �First, Do no harm� as the most
important principle of medicine back in ancient Greece. Naturopathic medicine
embraces a wide range of non-toxic therapies including lifestyle counseling and
exercise programs, diet and nutrition, herbs and homeopathy, spinal
manipulation to minor surgery. In fact, almost anything form of medical care
can be consistent with naturopathic principles as long as it does not harm the
patient or interfere with their body�s inherent healing processes. Minimizing
side effects can come not from using weak medicines but should result from
personalized care specifically directed toward your individual needs and
possibilities within an attentive and skillful doctor-patient relationship
using modern scientific tools but also taking the time to listen and provide a
healing touch.
4. Treat the Whole Person. Health
and wellness, dysfunction or disease all result from a complex and
ever-changing interaction of physical, emotional, dietary, genetic, environmental,
lifestyle and other factors. Naturopathic physicians treat the whole person,
taking all of these factors into account to craft an individualized, evolving
and dynamic therapeutic process that doesn�t just treat your �problem� but
focuses on you, the person who happens to have that �problem�.
5. Doctor as Teacher. The literal
meaning of �Doctor� is �teacher�. Thus, while a naturopathic physician
recognizes the need to �fix� problems at a mechanical or symptomatic level, the
greater opportunity for true and lasting healing arises when we, as patients,
learn from our health problems and change how we live so that we avoid the
situations that contributed to our distress and live our lives in more aware,
healthy and nurturing ways. Thus, a naturopathic physician aspires to engender
a safe and healing environment for a supportive and challenging therapeutic
relationship.
THE EDUCATION, TRAINING AND LICENSING OF NATUROPATHIC PHYSICIANS
Naturopathic physicians (N.D.) are general
practitioners trained as specialists in natural medicine. They are most highly
trained practitioners in the broadest scope of naturopathic medical modalities.
A naturopathic physician has a Doctorate of Naturopathic Medicine degree from a
four-year graduate level naturopathic medical college with admission
requirements comparable to those of conventional medical schools. In addition
to the standard medical curriculum of basic medical sciences and conventional
diagnostics, naturopathic students must do extensive coursework and clinical
study in natural therapeutics such as therapeutic nutrition, botanical
medicine, homeopathy, hydrotherapy, naturopathic manipulative therapy,
pharmacology, counseling and minor surgery. Many NDs have additional training
and certification in acupuncture and home birthing. Naturopathic Colleges are
certified and regulated by The Council on Naturopathic Medical Education,
accredited by that body and/or state or regional accrediting bodies, and
recognized by the US Department of Education. Naturopathic physicians practice
throughout the United States and Canada, as well as The United Kingdom,
Australia, India and other countries, In the U.S., NDs are licensed in thirteen
states, as well as the District of Columbia, Puerto Rico and Virgin Islands,
each of which has a set of statutes and regulations, as well as a state medical
board, which govern and oversee the practices of naturopathic physicians in
that state. In many states, NDs are licensed as primary care providers with the
authority to order lab tests, prescribe a broad range of prescription
medications, and sign birth and death certificates.
Naturopathic Physicians practice a wide range of natural
therapeutics, including:
CLINICAL NUTRITION.
Nutrition and therapeutic use of food have always
been a fundamental aspect of naturopathic medicine. A growing body of
scientific knowledge on diet and nutrition validates this approach to promoting
health, preventing illness and treating disease. Many medical conditions can be
treated effectively, with fewer complications and adverse effects, using foods,
customized diets, and nutritional supplements. Proper nutrition for the
individual provides the foundation of preventive medicine and a healthy
lifestyle.
HOMEOPATHY.
This powerful system of medicine was first developed in its
modern form in Germany ore than 200 years ago. Homeopathic medicines act to
stimulate and organize the body�s innate healing response.
BOTANICAL MEDICINE.
Plants can be powerful medicines. A growing body of scientific research
demonstrates that herbs can often be as effective, and sometimes superior to,
pharmaceutical drugs in clinical situations.
When used appropriately, they are safe and effective.
PHYSICAL MEDICINE.
Naturopathic physicians are trained in techniques of massage, manipulation,
and physical therapeutics, which are used to treat injury and pain.
(back
to content)
4.3 The history of Naprapathy w
Naprapathy was founded in the
beginning of the 20s century by Dr. Oakley Smith. He was from the beginning
working with chiropractors, but quickly abandoned the thought that �fetlocks
can jump out of their place�, the so called �subluxation-theory�, which at the
time was the customary theory within chiropractics. Instead, Smith believed
that the reason behind dysfunction and pain in the neuromusculoskeletal system
(muscles, joints, bone structure, connective tissue and nervous system) could,
amongst other things, be explained by modifications in the connective tissues
and states of tension in surrounding soft tissues. Today�s science can explain
that big parts of his conclusions were correct. As a direct effect of Smith�s
realisation that the causes of pain and other discomfort was much more complex
than just fetlocks and their position, he widened the treatment techniques to
also cover soft tissue techniques. This characterize the naprapathy of today
when you combine specific joint techniques with soft tissue techniques such as
massage.
4.4 The History of Physical Therapy w
Physical therapy (or
Physiotherapy) is a health care profession primarily concerned with the
remediation of impairments and disabilities and the promotion of mobility,
functional ability, quality of life and movement potential through examination,
evaluation, diagnosis and physical intervention carried out by Physical
Therapists (known as Physiotherapists in most countries). In addition to
clinical practice, other activities encompassed in the physical therapy
profession include research, education, consultation and administration.
Physical Therapists play an
important role in today�s healthcare system. As trusted healthcare experts in
restoring and improving motion, they contribute to their patients� quality of
life by keeping them healthy, fit, and active and, in many instances, avoiding
surgery and long-term use of prescription medications. In work-related
injuries, physical therapy is often the last course of treatment utilized
before the patient is released to return to work and placed at Maximum Medical
Improvement. Although most people are familiar with the term physical therapy,
few know of how this very important profession came to be.
From the elite athlete, person
with back or neck pain to someone having a spinal cord injury or stroke, the
profession of physical therapy now treats a multitude of musculoskeletal
injuries and disorders. Physical Therapy, like modern medicine, has constantly
evolved over the last century, now able to treat problems successfully better
than ever before. Here is a small look at the history of physical therapy.
Physicians like Hippocrates and
later Galenus are believed to have been the first practitioners of physical
therapy, advocating massage, manual therapy techniques and hydrotherapy to
treat people in 460 BC. After the development of orthopedics in the eighteenth
century, machines like the Gymnasticon were developed to treat gout and similar
diseases by systematic exercise of the joints, similar to later developments in
physical therapy.
The earliest documented origins
of actual physical therapy as a professional group date back to Per Henrik
Ling, �Father of Swedish Gymnastics,� who founded the Royal Central Institute
of Gymnastics (RCIG) in 1813 for massage, manipulation, and exercise. The
Swedish word for physical therapist is sjukgymnast = someone involved in
gymnastics for those who are ill. In 1887, PTs were given official registration
by Sweden�s National Board of Health and Welfare. Other countries soon
followed. In 1894 four nurses in Great Britain formed the Chartered Society of
Physiotherapy. The School of Physiotherapy at the University of Otago in New
Zealand in 1913 and the United States' 1914 Reed College in Portland, Oregon,
which graduated "reconstruction aides."
Modern physical therapy was
established in Britain towards the end of the 19th century. Soon following
American orthopedic surgeons began treating children with disabilities and
began employing women trained in physical education, massage, and remedial
exercise. These treatments were applied and promoted further during the Polio
outbreak of 1916. During the First World War women were recruited to work with
and restore physical function to injured soldiers, and the field of physical
therapy was institutionalized. In 1918 the term "Reconstruction Aide"
was used to refer to individuals practicing physical therapy.
The first school of physical therapy was established at
Walter Reed Army Hospital in Washtington D.C. following the outbreak of World
War I.
Research catalyzed the physical
therapy movement. The first physical therapy research was published in the
United States in March 1921 in "The PT Review." In the same year,
Mary McMillan organized the Physical Therapy Association (now called the
American Physical Therapy Association (APTA) and which currently represents
approximately 76,000 members throughout the United States. The APTA defines
physical therapy as: "clinical applications in the restoration,
maintenance, and promotion of optimal physical function."
In 1924, the Georgia Warm Springs
Foundation promoted the field by touting physical therapy as a treatment for
polio. Treatment through the 1940s primarily consisted of exercise, massage,
and traction. Manipulative procedures to the spine and extremity joints began
to be practiced, especially in the British Commonwealth countries, in the early
1950s. Later that decade, physical therapists started to move beyond
hospital-based practice to outpatient orthopedic clinics, public schools,
colleges/universities health centers, geriatric settings (skilled nursing
facilities), rehabilitation centers and medical centers.
Specialization for Physical
Therapy in the United States occurred in 1974, with the Orthopaedic Section of
the APTA being formed for those Physical Therapists specializing in
Orthopedics. In the same year, the International Federation of Orthopaedic
Manipulative Therapy (IFOMT) was formed, which has heralded change and progress
in manual therapy worldwide ever since. During this period, the eastern United
States were greatly influenced by the training of Norway's Freddy Kaltenborn
(Osteopathic Physician, Chiropractor, Physical Therapist, and Athletic Trainer.
Mariano Rocabado, PT of Chile, who specialized in treatment of
Temporomandibular disorders, also brought much new information and continues to
contribute to our profession. Australia's Geoffrey Maitland, PT initially
influenced the training of manual therapy on the west coast.
In the 1980's, the explosion of
technology and computers led to more technical advances in rehabilitation. Some
of these advances have continued to grow, with computerized modalities such as
ultrasound, electric stimulators, and iontophoresis with the latest advances in
therapeutic cold laser, which finally gained FDA approval in the United States
in 2002. Other advances, such as electronic resistive exercise known as
Isokinetics, have fallen out of popularity for various reasons, despite having
their place within the profession.
The 1990's brought much attention
to manual therapy, with formal residency programs becoming more numerous.
During the summer of 1991, Norwegian manual therapist Freddy Kaltenborne helped
create the American Academy of Orthopedic Manual Physical Therapy (AAOMPT). Dr.
Stanley Paris, PT and Ola Grimsby, PT were among the founding members. This
organization was a means for physical therapists to band together with a common
specialization in manual and manipulative therapy.
In the 21st century, the
profession has continued to grow substantially, by further developing the
scientific basis for its services, and by creating entry-level education
standards to meet the demands of today�s health care system. This vital work
will continue as the health care system is reformed.
Today�s physical therapy
profession boasts confident, accomplished, professional practitioners on the
cutting edge of health care, and it consistently ranks as one of the
international most desirable careers. These practitioners help individuals of
all ages to have optimal functioning and quality of life, while ensuring
patient safety and applying evidence to provide efficient and effective care.
Extensive education, clinical expertise, and "hands on" approach give
Physical Therapist a unique, individualized approach. When you are in the hands
of a physical therapist, you have a plan of care that is safe and appropriate
and customized to meet your individual needs.
(back
to content)
4.5 Osteopathic Philosophy and History w
Michael A. Seffinger, Hollis H. King, Robert C. Ward, John
M. Jones, iii, Felix J. Rogers, Michael M. Patterson
HOW IT ALL BEGAN
Andrew Taylor Still (1828�1917)
was an American frontier doctor who was convinced that 19th century patient
care was severely inadequate. This resulted in an intense desire on his part to
improve surgery, obstetrics, and the general treatment of diseases, placing
them on a more rational and scientific basis.
As his perspectives and clinical
understanding evolved, Still created an innovative system of diagnosis and
treatment with two major emphases. The first highlights treatment of physical
and mental ailments (i.e., diseases) while emphasizing the normalization of
body structures and functions. Its hallmark was a detailed knowledge of anatomy
that became the basis for much of his diagnostic and clinical work, most
notably palpatory diagnosis and manipulative treatment.
The second emphasizes the
importance of health and well being in its broadest sense, including mental,
emotional, and spiritual health, and the avoidance of alcohol and drugs, and
other negative health habits.
ORIGINS OF OSTEOPATHIC PHILOSOPHY
Historically, Still was not the first to call attention to
inadequacies of the health care of his time.
Hippocrates (c. 460� c. 377
B.C.E.), Galen (c. 130�c. 200), and Sydenham (1624�1689) are others. Each, in
his own way, criticized the inadequacies of existing medical practices, while
focusing contemporary thinking on the patient‟s natural ability to heal.
In addition, Still was deeply
influenced by a number of philosophers, scientists, and medical practitioners
of his time. There is also evidence he was well versed in the religious
philosophies and concepts of the Methodist, Spiritualist, and Universalist
movements of the period.
Following the loss of three
children to spinal meningitis in 1864, Still immersed himself in the study of
the nature of health, illness, and disease. His goal was to discover definitive
methods for curing and preventing all that ailed his patients. He implicitly
believed there was �a God of truth,� and that: �All His works, spiritual and
material, are harmonious. His law of animal life is absolute. So wise a God had
certainly placed the remedy within the material house in which the spirit of
life dwells.� Furthermore, he believed he could access these natural inherent
remedies �by adjusting the body in such a manner that the remedies may
naturally associate themselves together, hear the cries, and relieve the
afflicted�. In this quest, he combined contemporary philosophical concepts and
principles with existing scientific theories. Always a pragmatist, Still accepted
aspects of different philosophies, concepts, and practices that worked for him
and his patients. He then integrated them with personal discoveries of his own
from in depth studies of anatomy, physics, chemistry, and biology. The result
was the formulation of his new philosophy and its applications. He called it:
�Osteopathy.�
Still‟s moment of clarity
came on June 22, 1874. He writes, �I was shot, not in the heart, but in the
dome of reason�. �Like a burst of sunshine the whole truth dawned on my mind, that
I was gradually approaching a science by study, research, and observation that
would be a great benefit to the world�. He realized that all living things,
especially humans, were created by a perfect God. If humans were the embodiment
of perfection, then they were fundamentally made to be healthy. There should be
no defect in their structures and functions.
Since he believed that �the
greatest study of man is man,� he dissected numerous cadavers to test his
hypothesis. He believed that if he could understand the construction (anatomy)
of the human body, he would comprehend Nature‟s laws and unlock the keys
to health. Still found no flaws in the concepts of the body‟s
well-designed structure, proving to him that his hypothesis was correct.
A corollary to Still�s revelation
was that the physician does not cure diseases. In his view, it was the job of
the physician to correct structural disturbances so the body works normally,
just as a mechanic adjusts his machine. In Research and Practice he wrote, �The
God of Nature is the fountain of skill and wisdom and the mechanical work done
in all natural bodies is the result of absolute knowledge. Man cannot add
anything to this perfect work nor improve the functioning of the normal body.
Man‟s power to cure is good as far as he has a knowledge of the right or
normal position, and so far as he has the skill to adjust the bones, muscles
and ligaments and give freedom to nerves, blood, secretions and excretions, and
no farther. We credit God with wisdom and skill to perform perfect work on the
house of life in which man lives. It is only justice that God should receive
this credit and we are ready to adjust the parts and trust the results�.
While Still practiced the
orthodox medicine of his day from 1853 to 1879, including the use of oral
medications such as purgatives, diuretics, stimulants, sedatives, and
analgesics, and externally applied salves and plasters, once he began using his
new philosophical system he virtually ceased using drugs. This occurred after
several years where he experimented with combinations of drugs and manipulative
treatment. In addition, he compared his results with those of patients who
received no treatment at all. After several years‟ experience, he became
convinced that his mechanical corrections consistently achieved the same or
better results without using medications.
It was at that point that Still
philosophically divorced himself from the orthodox practices of 19th century
medicine. He writes, �Having been familiar myself for years with all their
methods and having experimented with them I became disheartened and dropped
them�. His unerring faith in the natural healing capabilities of the
mechanically adjusted body formed the foundation for his new philosophy.
Unsure of what to call his new
hands-on approach in the early years, Still at times referred to himself as a
�magnetic healer� and �lightning bone-setter�. In the 1880s Still began
publicly using the term �osteopathy� as the chosen name for his new profession.
He writes: �Osteopathy is compounded of two words, osteon, meaning bone, (and)
pathos, (or) pathine, to suffer. I reasoned that the bone, �Osteon,‟ was
the starting point from which I was to ascertain the cause of pathological
conditions, and so I combined the �Osteo‟ with the �pathy‟ and had
as a result, Osteopathy�.
As the name osteopathy implies,
still used the bony skeleton as his reference point for understanding clinical
problems and their pathological processes. On the surface, he was most
interested in anatomy. On the other hand, he taught that there is more to the
skeleton than 206 bones attached together by ligaments and connective tissue.
In his discourses, Still would describe the anatomy of the arterial supply to
the femur, for example, trace it back to the heart and lungs, and relate it to
all of the surrounding and interrelated nerves, soft tissues, and organs along
the way. He would then demonstrate how the obstruction of arterial flow
anywhere along the pathway toward the femur would result in pathophysiologic changes
in the bone, producing pain or dysfunction.
He writes of his treatment
concepts: �Bones can be used as levers to relieve pressure on nerves, veins and
arteries�. This can be understood in the context that vascular and neural
structures pass between bones or through orifices (foramina) within a bone.
These are places where they are most vulnerable to bony compression and
disruption of their functions. In addition, fascia is a type of connective
tissue that attaches to bones. Fascia also envelops all muscles, nerves, and
vascular structures. When strained or twisted by overuse or trauma myofascial
structures not only restrict bony mobility, but also compress neurovascular
structures and disturb their functions. By using the bones as manual levers,
bony or myofascial entrapments of nerves or vascular structures can be removed,
thus restoring normal nervous and vascular functions.
(back
to content)
4.6 Craniosacral therapy
w
Craniosacral therapy (CST) or
cranial osteopathy is a form of alternative therapy that uses gentle touch to
palpate the synarthrodial joints of the cranium. CST is a pseudoscience, and
its practice has been characterized as quackery. It is based on fundamental
misconceptions about the physiology of the human skull and is promoted as a
cure-all for a variety of health conditions.
CST was invented in the 1970s by John Upledger as an
offshoot of cranial osteopathy, which had been devised in the 1930s by William
Garner Sutherland.
Medical research has found no
good evidence that either CST or cranial osteopathy confers any health benefit,
and they can be harmful, particularly if used on children or infants. The basic
assumptions of CST are not true, and practitioners produce conflicting and
mutually exclusive diagnoses of the same patients.
Practitioners of CST claim it is
effective in treating a wide range of conditions, sometimes claiming it is a
cancer cure, or a cure-all. Practitioners particularly advocate the use of CST
on children. The American Cancer Society cautions that CST should never be used
on children under age two. Pediatricians have expressed concern at the harm CST
can cause to children and infants.
Craniosacral therapy (CST)
Cranial-sacral therapy
Cranial osteopathy
Cranial therapy
Craniopathy
Sacro-occipital technique
Bio-cranial therapy
Craniosacral therapy
Alternative therapy
NCCIH Classification Manipulation and body-based School
Osteopathy
Effectiveness and safety
CST is potentially harmful. There
have been cases of people with head injuries suffering further injury as a
result of CST. If used as an alternative for legitimate therapy for a serious
condition, choosing CST can have serious adverse consequences.
According to the American Cancer
Society, although CST may relieve the symptoms of stress or tension,
"available scientific evidence does not support claims that craniosacral
therapy helps in treating cancer or any other disease". Cranial osteopathy
has received a similar assessment, with one 1990 paper finding there was no
scientific basis for any of the practitioners' claims the paper examined. A
2019 systematic review found limited evidence that CST may bring some relief
for up to 6 months for people with chronic pain.
In October 2012, Edzard Ernst
conducted a systematic review of randomized clinical trials of craniosacral
therapy. He concluded that "the notion that CST is associated with more
than nonspecific effects is not based on evidence from rigorous randomised clinical
trials."
Commenting specifically on this
conclusion, Ernst wrote on his blog that he had chosen the wording as "a
polite and scientific way of saying that CST is bogus." Ernst also
remarked that the quality of five of the six trials he had reviewed was
"deplorably poor", a sentiment that echoed an August 2012 review that
noted the "moderate methodological quality of the included studies."
Ernst criticized a 2011
systematic review performed by Jakel and von Hauenschild for including
observational studies and including studies with healthy volunteers. This
review concluded that the evidence base surrounding craniosacral therapy and
its efficacy was sparse and composed of studies with heterogeneous design. The
authors of this review stated that currently available evidence was insufficient
to draw conclusions.
The evidence base for CST is
sparse and lacks a demonstrated biologically plausible mechanism. In the
absence of rigorous, well-designed randomized controlled trials, it is a
pseudoscience, and its practice quackery.
Tests show that CST practitioners
cannot in fact identify the purported craniosacral pulse, and different
practitioners will get different results for the same patient. The idea of a
craniosacral rhythm cannot be scientifically supported.
REGULATION
Edzard Ernst wrote that in 2005
in the United Kingdom, a foundation of the Prince of Wales issued a booklet
listing CST as one of several popular alternative therapies, but admitted that
the therapy was unregulated and lacked either a defined training program or the
oversight of a professional body. Ernst writes that this makes the therapists
practising CST "less regulated than publicans."
Cranial osteopathy, a forerunner
of CST, was originated by Sutherland in 1898�1900. While looking at a disarticulated
skull, Sutherland was struck by the idea that the cranial sutures of the
temporal bones where they meet the parietal bones were "beveled, like the
gills of a fish, indicating articular mobility for a respiratory
mechanism."
From 1975 to 1983, Upledger and
neurophysiologist and histologist Ernest W. Retzlaff worked at Michigan State
University as clinical researchers and professors. They assembled a research
team to investigate the purported pulse and further study Sutherland's theory
of cranial bone movement. Later independent reviews of these studies concluded
that they presented no good evidence for the effectiveness of craniosacral
therapy or the existence of the proposed cranial bone movement.
Practitioners of both cranial
osteopathy and CST assert that there are small, rhythmic motions of the cranial
bones attributed to cerebrospinal fluid pressure or arterial pressure. The
premise of CST is that palpation of the cranium can be used to detect this
rhythmic movement of the cranial bones and selective pressures may be used to
manipulate the cranial bones to achieve a therapeutic result. However, there is
no evidence that the bones of the human skull can be moved by such
manipulations.
The fundamental concepts of
cranial osteopathy and CST are inconsistent with the human skull, brain, and
spine's known anatomy and physiology. Edzard Ernst has written "to anyone
understanding a bit of physiology, anatomy etc. [CST] looks like pure
nonsense."
In common with many other
varieties of alternative medicine, CST practitioners believe all llness is
caused by energy or fluid blockages which can be released by physical
manipulation. They believe that the bones of the skull move in a rhythmic
pattern which they can detect and correct.
The therapist lightly palpates
the patient's body, and focuses intently on the communicated movements. A
practitioner's feeling of being in tune with a patient is described as History
Conceptual basis entrainment.
CRANIAL OSTEOPATHY VS CRANIOSACRAL THERAPY
Comparing it to cranial osteopathy
Upledger wrote: "Dr. Sutherland's discovery regarding the flexibility of
skull sutures led to the early research behind CranioSacral Therapy� and both
approaches affect the cranium, sacrum and coccyx� the similarities end
there." However, modern-day cranial osteopaths largely consider the two
practices to be the same, but that cranial osteopathy has "been taught to
non-osteopaths under the name CranialSacral therapy."
(back
to content)
4.7 Origins and History of Chiropractic w
The word �chiropractic� comes
from the Greek words cheir (meaning �hand�) and praktos (meaning �done�), i.e.,
done by hand. Manual healing methods can be traced back to ancient times;
however, it was not until the late 19th century that the chiropractic
profession in the United States began to take shape.
Daniel David Palmer is widely
credited with giving the first chiropractic adjustment in 1895. He also
established the first chiropractic school in 1897 in Davenport, Iowa. From that
point forward, Palmer and others continued to refine chiropractic manual
adjusting techniques as well as study how manual manipulation can relieve pain
and improve function. While spinal manipulation continues to be a centerpiece
of chiropractic care, modern chiropractors have developed a variety of practice
styles, featuring different therapies and modalities, to address patients�
needs. They practice a holistic approach to health care that generally excludes
drugs or surgery.
As the new profession was getting
on its feet in the early 20th century, chiropractors began organizing into
professional societies. These groups launched efforts to standardize education
and support research. Today, there are almost 20 chiropractic colleges in the
United States accredited by the Council on Chiropractic Education, which was
officially recognized in 1974 by the U.S. Department of Education as the
accrediting agency for chiropractic schools. In 1996, the U.S. government began
funding chiropractic research through the National Institutes for Health and
over the years the profession has received millions in federal funding for
scientific research thanks to robust research programs at several of the
colleges.
Chiropractic is a regulated
healthcare profession in the United States and has been for more than 100
years. Before being granted a license to practice, doctors of chiropractic
(DCs) must meet stringent educational and competency standards set forth by the
National Board of Chiropractic Examiners and individual states. Kansas was the
first state to license chiropractic in 1913. Today, all 50 U.S. states, the
District of Columbia, all U.S. territories, and more than 40 countries
worldwide license chiropractors.
With an increasing body of
research supporting its approach, the chiropractic profession has over time
become integrated into many healthcare systems, hospitals, and public and
private health and managed care plans. Spinal manipulation was first included
in Medicare in 1972 (efforts continue to expand the services that chiropractors
can provide to Medicare beneficiaries), and two years later in 1974
chiropractic care became a benefit in the Federal Employee Health Benefits
Program. Chiropractic is also a benefit in most state workers� compensation
programs.
Nondrug pain relief has been
especially important to active-duty members of the military as well as
veterans, many of whom experience chronic musculoskeletal pain as a result of
their service. Congress passed legislation in 1993 to include chiropractic in
the U.S. Department of Defense healthcare system. Today Chiropractic services
are available to active-duty personnel at more than 60 military bases in the
United States, Germany and Japan.
Legislation to include
chiropractic in the U.S. Department of Veterans Affairs (VA) healthcare system
was passed in 1999. Chiropractic is now available at 70 major VA medical
facilities in the United States. In addition, in 2014 the VA launched a
chiropractic residency program�the first of its kind in the country�where
chiropractors train alongside their medical counterparts at VA medical systems
around the country. The residency is a full-time one-year program in integrated
clinical practice emphasizing the delivery of chiropractic care in hospitals
and other integrated healthcare settings.
In recent years, the epidemic of
opioid overuse has prompted many respected health organizations to recommend
the use of nondrug approaches for pain relief as a first line of defense,
potentially helping patients to reduce or avoid the need for prescription pain
medications. Notably, the American College of Physicians (ACP) updated its
guideline for the treatment of acute and chronic low back pain in 2017 to
recommend first using noninvasive, nondrug treatments�including spinal
manipulation�before resorting to drug therapies. A host of other organizations
have since endorsed ACP�s guideline or issued similar recommendations.
The chiropractic profession
continues to grow and evolve. There are more than 70,000 chiropractors licensed
today in the United States�practicing in solo practices, multidisciplinary
clinics and major hospital systems. It is estimated that more than 35 million
people visit a chiropractor each year.
(back
to content)
4.8 Immunology and Homeopathy. 1. Historical Background v
Paolo Bellavite1, Anita Conforti2, Valeria Piasere1 and
Riccardo Ortolani3 2005
Homeopathy was born as an
experimental discipline, as can be seen from the enormous amount of homeopathic
data collected over more than two centuries. However, the medical tradition of
homeopathy has been separated from that of conventional science for a long
time. Conventional scientific wisdom dictates that homeopathy should have no
effect above placebo but experiments on ultra-high dilutions of solutes
together with some clinical data suggest the intriguing possibility that it
might do in some circumstances. Today, an osmotic process between disciplines,
previously seen as in conflict, is facilitated because over the last few decades�
homeopathy has initiated the methods of current medical science and a
substantial number of experimental studies�at molecular, cellular and clinical
levels�are available. One area of dialogue and of common progress is that of
inflammation and immunity, probably because these are closely related to the
traditional �vital force� of the body�s self-healing power. In a series of papers,
we review the historical origins of homeopathy, the laboratory and animal
models related to the field of immunopharmacology, the clinical evidence in
favor and against the use of homeopathy in the inflammatory diseases and the
hypotheses regarding its action mechanism(s). Finally, we will enlighten the
specific characteristics of the homeopathic approach, which places great
emphasis on identifying a cure for the whole organism.
Keywords: Hahnemann � Hippocrates � history of medicine �
homeopathy � immunotherapy � isotherapy � nosodes � Paracelsus � similia
principle
The majority of substances have
more than one action; the first is a direct action, which gradually changes
into the second, which I call its indirect secondary action. The second is
generally the opposite of the first C.F.S. Hahnemann, 1796
INTRODUCTION
The main principle of homeopathy,
a unique scientific system of medicine established by Samuel Hahnemann two
centuries ago, is that of �similia� or �simile� (similarity), which means �let
likes be cured by likes�. In other words, when a substance is capable of
inducing a series of symptoms in a healthy living system, low doses of the same
substance can cure these symptoms under certain circumstances (�similia
similibus curentur�).
About 200 years have passed since
the original interpretation of the principle of similarity. During this period,
medicine evolved as never before and homeopathic theories and pharmacopoeias
have also been scientifically investigated, albeit slowly with considerable
delay in comparison with those of conventional medicine. However, the
fundamental nucleus of homeopathy has been little discussed. Similarity is frequently
considered unscientific because the statements of Hahnemann or other homeopaths
are not supported by documentary proof. The various principles of similarity,
Hahnemann as a scientist, Hahnemann�s homeopathy, various �homeopathic�
innovations such as electro-homeopathy and various types of alternative therapy
including herbal medicine have been indescribably confused, and this has led to
conclusions being drawn on the basis of summary subjective judgments.
Figure 1. Jenner vaccinating a child with cow smallpox.
�
Figure 3. E.A. Von Behring (1854�1917).
�
Figure 2. C.F.S. Hahnemann (1775�1843).
Unless these sources of confusion
are constantly and completely acknowledged and corrected, little progress can
be made in clarifying the concepts of homeopathy or the principle of
similarity.
Immunology is the study of the
structure and function of the immune system, the complex and integrated group
of organs, tissues, cells and cell products such as antibodies that, by
differentiating self from non-self, defend the body against infection or
disease and neutralize potentially pathogenic cells or substances. This branch
of biomedicine initially found resistance in differentiating from more
traditional medical disciplines such as pathology and physiology, recent
decades have witnessed an extraordinary development.
Western immunology and homeopathy
both began at the end of the eighteenth century: the first of Jenner�s smallpox
vaccinations (Fig. 1) were given at the same time that the German physician
Samuel Hahnemann (Fig. 2) was conducting his first homeopathic �provings�. The
first organic enunciation of the fundamentals of homeopathy was made by
Hahnemann in 1796: �One imitates nature, which sometimes cures chronic diseases
by adding another disease, and then uses in the (preferably chronic) disease a
drug that is capable of exciting another artificial disease as similar as
possible to the natural disease to be cured: similia similibus�.
The profound analogies between
homeopathic thought and immunology are due to the fact that the whole of
homeopathic theory is substantially based on the principle of regulating
endogenous systems of healing, the best known of which is certainly the immune
system and its neuroendocrine integrations.
A significant example of a pioneer of immunology with an
open mind towards the new homeopathic theories was Emil Von Behring (Fig. 3),
who wrote:
The mechanisms of action of my
anti-toxin therapy are still unclear, although many authors say that the
diphtheria and tetanus anti-toxins can be clearly understood on the basis of
Ehrlich�s lateral chain theory. (. . .) Despite all of the scientific
speculations and experiments of anti-smallpox vaccinations, Jenner�s discovery
remained a relatively isolated episode in medicine until Pasteur connected its
origin with a principle that cannot be better characterized than by Hahnemann�s
word: homeopathic. What else causes epidemiological immunity in a sheep
vaccinated against anthrax, if not the influence previously exercised by a
micro-organism having similar characteristics to those of fatal anthrax? And
what Figure 1. Jenner vaccinating a child with cow smallpox.
Homeopathy and immunology
technical term appropriately defines this influence exercised by a similar
micro-organism if not the word of Hahnemann: homeopathy?
In 1912 he wrote �Hahnemann
principle, according to our present way of thinking, was not bad at all� and
�The concept that the sick person reacts differently to medications than the
healthy one, which had to be established empirically by therapeutic trials,
also played a role in Hahnemann�s thinking�.
Hahnemann�s principles of
homeopathy were not totally new as traces of them can be found throughout the
history of medicine.
THE �MAGICAL� SIMILE
The principles underlying homeopathy can be traced to roots
dating back even further than those of immunology.
Mankind has always wondered how
to identify remedies capable of curing diseases. In the pre-scientific era,
empiricism based on chance observations, and trial and error, was probably the
most widely used approach, accompanied by various forms of oral or written
tradition. In many other cases, the sick relied (and still do among some
primitive people) on the intuition of individuals judged to be particularly
endowed with divine or natural powers: healers, shamans, witchdoctors and so
on. However, there was also another line of thought that, often in a marginal
manner, has accompanied various medical cultures in different epochs: the
identification of particular �resemblances� between remedies and the diseases
they were thought to be able to cure. The first examples of treating �like with
like� can be found in the papyrus of Ebers (1500 BC): ear diseases treated with
ear extracts, headache with fish heads, blindness with the eyes of a pig.
Attempting to treat a disease by
administering the agent capable of causing it or transmitting it is one of the
most general acquisitions of empirical medicine. Numerous primitive medicines
used to cure the effects of snake venoms by repeatedly inoculating them or
materials extracted from the venom apparati of snakes. In the Far East the
Chinese practiced a form of preventive smallpox vaccination both by wearing the
clothes worn by a smallpox victim in the full suppuration phase of the disease
and by inhaling dried smallpox pustules after storing them for 1 year. Pliny
claimed that the saliva of a rabid dog can afford protection against rabies.
Dioskurides of Anazarbo recommended that hydrophobia sufferers eat the liver of
the dog that bit them. Aetius of Antioch recommended eating the meat of the
viper that had just bitten you. In the seventeenth century the Irishman Robert
Fludd cured the victims of consumption with dilutions of their own sputum after
suitable preparation.
Equally primitive and often
elaborate applications of the same principle could be found in many
pharmacopoeias until the last century. The reasoning is sometimes elementary:
swallow human stones in cases of calculosis but, also here, the connection is
obscure in the light of current knowledge. It is well known that King
Mithridates VI (132� 163 BC) is said to have taken small quantities of poisons
and toxins to protect himself against the repeated attempts made to poison him.
Native Americans wear a headdress of eagle feathers partly to underline their
prowess as hunters and partly for decorative purposes, but the custom is also
based on a belief that the sight, speed, courage and other desirable
characteristics of the eagle can be magically acquired. The magical transfer of
the courage of a killed enemy to the victor by means of the ingestion of organs
(the heart) also explains some aspects of cannibalism.
THE �SIMILE� OF HIPPOCRATES
By means of highly acute
observations made without sophisticated instruments but still valid today, the
school of Hippocrates understood that many of the phenomena of a disease are
attempts at cure and suggested imitating them: this is the Hippocratic �simile�
(Fig. 4). The most frequently cited assertions are:
The pains (complaints) will be removed by means of their
opposite, each according to its own characteristics.
Thus, heat corresponds to a hot constitution that has been
made ill by the cold, and so on for the others.
Another way of removing pain is
the following: a disease develops by means of its like and is cured by means of
the use of its like. Thus, what causes urinary tenesmus in health cures it in
disease. Cough is caused and cured by means of the same agent, as in the case
of urinary tenesmus. Another method: the fever causing the development of
inflammation will be caused and cured by the same agent. At other times, it
will be cured by the opposite of its cause.
It is particularly worth
mentioning that Hippocrates did not adopt a dogmatic or ideological position,
but saw both approaches (�similarity� and �opposition�) as potentially useful.
Prognostic interest, a great capacity for controlled observation, the rejection
of fanciful tendencies and other characteristics unmistakably distinguish this
from magic.
Without going into the whole of Hippocratic medicine, it
must be said that his doctrine is permeated by the concept of natural healing.
Nature (�physis�) is the healer of disease.
�Physis� is an expression of
life, not a special energy; it is unconscious or similar to instinct; it prevails
over physiological and mechanical processes; it combats disease; it is
frequently incomplete and must be assisted by a doctor. It is likely that no
thought has had a more profound effect on medicine than Hippocrates�
observation that the manifestations of disease consist of two groups of events:
the first being the direct effects of the damage, the second the reaction of
repair. The corollary to this is that the direct effects must be removed
whenever possible, but the reparative reaction must be promoted in order to
imitate nature. Hippocrates considered many pathophysiological phenomena as
being fundamentally �defensive�: fever, skin eruptions and others. In line with
this pathophysiological conception, physicians must make a distinction between
useful and harmful symptoms by stimulating the former and blocking the latter.
Using typical Greek conciseness,
Hippocrates formulated what can legitimately be considered
one of the fundamental rules of therapy: nature is the primary physician and
the first duty of medicine is �to do no harm�.
THE �SIMILE� OF PARACELSUS
One further representative of
this line of thought was P.T. von Hohenheim, also known as Paracelsus (Fig. 5).
His works, which were first published in Basel in an almost complete version of
11 volumes between 1589 and 1591, contain a mixture of genial intuitions and
ingenuities; profound clinical observations and strange affirmations concerning
the influence of celestial bodies; new pharmacological observations and
convinced assertions as to the truth of alchemical and magical concepts. Among
other things, Paracelsus proposed the �doctrine of signatures� (�signa
naturae�) according to which the therapeutic properties of different remedies
were �similar� to�and could be deduced from�the external appearance of plants
and minerals: red remedies for blood diseases, sharply pointed leaves for the
pain caused by stab wounds, iriscolored Eufrasia for eye diseases, topaz
against jaundice (because both are yellow) and so on. In this way, �magical
similarity� was re-exhumed in an empirical and intuitive manner without any
scientific understanding or experimental proof.
However, not all of the work of
Paracelsus was �magical�: he had many important intuitions and made a number of
empirical observations that were to form the basis for a large number of
medical applications in subsequent centuries. For a long time, the following
citation was considered one of the most significant anticipations of the
�simile� as seen by homeopathy: �What causes jaundice also cures jaundice. That
is, the good and the bad lie in the same thing: the bad causes jaundice but, if
you separate the good, it becomes an efficacious remedy against jaundice. . .
Since the drugs that cure paralysis must come from the substances that cause
it. . . This is the way to understand the curative powers of minerals. . . What
may be harmful in our hands can be transformed into a medicine�. There is also
a certain harmony with the concepts concerning drug doses that were
subsequently adopted by homeopaths, since according to Paracelsus medicines
must be administered not on the basis of their weight, but according to
criteria that go beyond simple weight.
In the post-Paracelsian period,
the �simile� was often mentioned, but usually in reference to magical practices.
Typical authors are Porta, who attempted to apply the doctrine of signatures to
the whole botanic world (examples include the use of hairy plants for scalps,
beautiful plants to improve personal appearance, �happy� plants, �sad� plants,
etc.), and Schroder who presented related ideas, such as the fact that the
leaves of Hepatica triloba resemble the liver. One true predecessor of
Hahnemann was Stoerck (1731�1803), who in the 1760s published a series of works
on the treatment of diseases with poisons according to the principle of
similars. This author made a highly significant statement:
�If stramonium causes illness in
someone who is sound in mind by inducing mental confusion, why should we not
try to establish whether it can give mental health to someone who is confused
or whose senses are altered by disease?
If it cures someone affected by spasms, why should we not
investigate whether it causes the spasms?�.
�
Figure 5. P.T. von Hohenheim (Paracelsus) (1494�1541).
Christian Frederick Samuel Hahnemann
was born on April 10, 1755 in Meissen, Germany, graduated in Medicine from
Erlangen University in 1779, and died in Paris in 1843 after a long and
adventurous life. Although he worked in many fields of chemistry, pharmacology
and medicine, he has passed into history as the founder of homeopathy, of which
he is still unanimously acknowledged as being the greatest authority.
The first reflection of Hahnemann
concentrated on the fact that two diseases may interact in very particular ways
in the same individual, with one temporarily or permanently taking the place of
another. One example is the well-known alternation of eczema and asthma as
chronic expressions of an allergic constitution. Hahnemann studied the less
known lasting replacement of one disease by another and, for example, observed
that a chronic skin rash disappeared after the onset of measles. He wondered
what it was that led to this difference between temporary and permanent
replacement, and became convinced that the latter occurred when the two
diseases had similar symptoms.
His next step was to try to apply
this finding in a systematic and therapeutic manner. As he was also an expert
in chemistry, he was familiar with many of the symptoms caused by toxic agents
and aware of the fact that a number of naturally occurring diseases closely
resemble symptoms owing to intoxication:
e.g. the intoxication induced by
Belladonna resembles scarlet fever; that induced by quinine resembles malaria;
and that induced by arsenic resembles cholera. It did not take him long to
combine the idea of the replacement of similar diseases with that of the
replacement induced by �artificial� intoxication:
for example, he tried to use low doses of Belladonna to
treat patients with scarlet fever and of arsenic to treat cholera.
He intuitively understood that it was possible to discover
specific remedies for a number of diseases, and therefore sought other
potentially advantageous drugs and tested their �pathogenetic� power in healthy
volunteers. After a long series of experiments on himself, his family and the
medical students who followed his ideas, Hahnemann arrived at the first
generalization of his thought in 1796 and then its overall description in the
treatises called �Organon�, �Chronic Diseases� and �Materia Medica�, which were
published in various editions during the first decades of the nineteenth
century.
Little by little, Hahnemann refined his homeopathic ideas.
For example, he discovered that
diseases other than cholera could be cured by small doses of arsenic provided
that they had other common �characteristics of arsenic�. However, not all
cholera patients responded to arsenic, but required another remedy depending on
their individual symptoms. He thus changed the current nosological schema of
medical thought by introducing the concepts of drug-specific pathogenesis and
disease-specific individual status. He then noted that patients apparently
cured by means of homeopathy could suffer a recurrence of the same disease or
be affected by another, and drew the conclusion that permanent cure could only
be achieved by selecting the remedy on the basis of other criteria, including
the patient�s constitutional and psychological characteristics, as well as
previous diseases.
Hahnemann interpreted his
�simile-based� therapy as the result of a reactive process that we would now
call homeostatic or, better, homeodynamic: �If, in the case of a chronic
disease, you give a medicine whose primary direct action corresponds to the
disease itself, its secondary indirect action exactly represents the state of
the body it is desired to obtain. . .�.
The fundamental points of
Hahnemann�s �simile� can be summarized in Table 1. In other words, according to
Hahnemann the �vital energy� alone is not sufficient to combat the disease.
By giving a remedy that resembles
the disease, this instinctive natural force (in analogy to the hippocratic
�physis�) is driven to increase its energy to a point at which it becomes
stronger than the disease itself, which finally disappears.
Hahnemann also claimed that
diluting the remedies in a particular manner (�potentiation� obtained by the
extensive succession of serial dilutions) not only reduced or abolished their
toxic effects, but also paradoxically increased their curative power, which is
still one of the most controversial aspects of homeopathy. Another highly
criticized aspect is the theory of the �psora� and the �miasmas�, by means of
which Hahnemann tried to describe the diseases of his time.
However, it is necessary to point
out that Hahnemann never claimed that homeopathy was the only guide to therapy,
but often said that the primary method of treatment (�the highest to be
pursued�) is to remove the fundamental cause of the disease.
He called this the �real way� or
�causal therapy� and, rather than contesting its value, doubted the possibility
of applying it. It must be remembered that he lived between the end of the
eighteenth and the beginning of the nineteenth century.
The application of Hahnemann�s
theory of �simile� not only requires a scrupulous study of �Materia Medica� (a
compendium of the symptoms caused by the various substances in normal human
beings), but also of the symptoms and pathophysiological characteristics of
each individual patient:
We must, on the one hand, first
precisely understand the essential characteristics and incidental
manifestations of the diseases of the human body and, on the other, the effects
purely due to the use of drugs: that is, their essential characteristics and
the incidental symptoms of the specific artificial diseases they induce (as a
result of differences in dose, form, etc.).
In this way, by choosing a remedy
capable of causing an artificial disease that is very similar to a given
natural disease, we will be able to cure the most obstinate of diseases.
As we have already mentioned and
as is only logical, further discoveries and applications have gradually added
themselves to the initial concepts and ground rules. Among these, particularly
worthy of note are �isopathy� and the introduction of the use of the so-called
�nosodes�.
Table 1. Essential principles of classical homeopathy
_ Potentially therapeutic substances must be tested
carefully in healthy subjects in order to document their �pure�, direct
effects: this is the basis of the medical matter
_ The remedy capable of causing a similar state in a healthy
subject causes a counter-reaction in a patient that is stronger than the
pathological stimulus of the disease itself
_ The disease must be studied as a whole (and not only in
terms of its main
symptom or pathology) in order to ensure that it and the
drug interact in a global manner; the choice of the remedy must be based on the
complex of individual symptoms rather than on the name of the disease
_ The dose must be the minimal effective dose and therefore
adjusted on the basis of individual sensitivity
_ Homeopathy empirically maintains that the dose should be
higher in the case of acute diseases affecting specific organs, whereas chronic
diseases that are more sensitive to pharmacological stimulation should be
treated with high dilutions (�potencies�) separated by much longer intervals Isotherapy
and Nosodes
One of the earliest and most notable innovations of
homeopathy, mentioned even in the later editions of the Organon, is isopathy or
isotherapy. The term was probably coined by the veterinarian Wilhelm Lux
somewhere around 1831�33:
after starting to treat his
animals with the homeopathic method, he became convinced that every contagious
disease bears within itself the means whereby it can be cured. He observed that
the technique of dilution and dynamization of a contagious product (bacterium,
virus or infected secretions, and organic material) would put such a product in
a position to exert a therapeutic action on the disease resulting from the
contagion.
The law of similars �Similia similibus curentur� thus
becomes �Aequalia aequalibus curentur� or the law of sameness.
Three authors dominate the
history of isopathy, and all three were homeopaths: Constantine Hering, Wilhelm
Lux and Denys Collet. Constantine Hering (Fig. 6) was born in Saxony in 1800
and became an assistant to the surgeon Robbi, who entrusted him with the task
of writing a book for him confuting homeopathy once and for all, as had already
been requested by the publisher Baumgartner. After taking a closer look at
Hahnemann�s works, Hering was not only intrigued, but ended up by defending
Hahnemann and coming out in favor of the new method. Hering contributed a great
deal to homeopathy, but above all it is to him that we owe some drug provings
and the preparation of homeopathic remedies from pathological excretions and
secretions, which he terms �nosodes�. Originally this term denoted any remedy
extracted from pathological excretions or secretions obtained from human
subjects or animals. Animal poisons were included in this definition, so much
so indeed that Hering was the first to �prove� �Lachesis� (venom of the
bushmaster snake, the first nosode in history, later to become a homeopathic
remedy to all intents and purposes) and the rabies �poison�. Convinced that
every disease contains within it its own remedy and prophylaxis, he extended
his studies to the scabies �virus�, extracting the alleged �virus� from
blisters from a subject with well developed scabies.
Hering also maintained that
products of the human body and the various parts of the body in the healthy
state all have a preferential action on the corresponding diseased parts, and
as early as 1834 he advised the use of diluted and dynamized homologous organs
(�iso-organotherapy�). Finally, he assumed that the chemical elements exerted a
particular action on those organs in which they were mainly contained. His
studies and papers on minerals and salts preceded the work of Schu�ssler on
biochemical salts.
The second great isopath was the
veterinarian Joseph Wilhelm Lux, born in Silesia in 1776. Lux was appointed
Professor of Veterinary Science at the University of Leipzig in 1806, and his
work constituted a landmark in the history of veterinary medicine. From 1820
onwards he was familiar with Hahnemann�s works and applied the new method in
veterinary medicine, becoming a staunch advocate of veterinary homeopathy. In
1831 Valentin Zibrik asked him for a homeopathic remedy for distemper and
anthrax. As he knew of no homeopathic remedies for these epidemics at the time,
his advice was to replace the homeopathic �similar� (i.e. the drug prescribed
on the basis of the symptoms) with a 30c dilution of a drop of nasal mucus from
an animal with distemper and a 30c dilution of a drop of blood of an animal
with anthrax, and get all the animals suffering from distemper and anthrax,
respectively, to take them. He was thus the first to create the strain called
Anthracinum. In 1833 Lux published the results obtained in a booklet entitled Isopathik
der Contagionen, in which he claimed that all contagious diseases bear within
their pathological phenomena and products their own means of cure. Moreover,
Lux also extended the principle to substances that had become iatrogenic as a
result of abuse, so that a method which was originally used only in contagious
diseases was also applied to non-contagious illnesses. Isopathy Table 1.
Essential principles of classical homeopathy Potentially therapeutic substances
must be tested carefully in healthy subjects in order to document their �pure�,
direct effects: this is the basis of the medical matter The remedy capable of
causing a similar state in a healthy subject causes a counter-reaction in a
patient that is stronger than the pathological stimulus of the disease itself
�The disease must be studied as a whole (and
not only in terms of its main symptom or pathology) in order to ensure that it
and the drug interact in a global manner; the choice of the remedy must be
based on the complex of individual symptoms rather than on the name of the
disease
�The dose must be the minimal effective dose
and therefore adjusted on the basis of individual sensitivity Homeopathy
empirically maintains that the dose should be higher in the case of acute
diseases affecting specific organs, whereas chronic diseases that are more
sensitive to pharmacological stimulation should be treated with high dilutions
(�potencies�) separated by much longer intervals
|
�
|
Figure 6. C. Hering (1800�80).
provoked endless arguments in the
homeopathic circles: other nineteenth century relevant physicians who employed
isopathy were Stapf, Rademacher (founder of �organotherapy�), Brown- Se�quard,
Arnold, Veith, while Griesselich, Berridge and others disapproved this method
because the isopathic substancs were rarely subjected to proving and were not
prescribed on the basis of symptom similarity as in the original Hahnemann�s
method.
After this early period of
expansion, the new method ran into continuous and increasingly severe
criticism, so much so that isopathy went into decline for several years, even
within the homeopathic community. Only a few solitary practitioners went on
using isopathic remedies. It was Father Denys Collet, a doctor and Dominican
friar born in 1824, who eventually brought isopathy back onto the scene. In
1865 he witnessed a homeopathic healing which convinced him to devote himself
to the new method. He rediscovered isopathy alone and after several decades of
practice published a book entitled Isopathie, Me�thode Pasteur par Voie Interne
at the age of 74. According to Collet, there are three ways of healing, namely
allopathy, homeopathy and isopathy, all of which are useful depending on the
clinical indications. In addition, he distinguishes between three types of
isopathy: (i) �Pure isopathy�, which uses secretion products from the patient
to cure the same disease. (ii) �Organic isopathy�, which cures the diseased
organs with dynamized derivatives from healthy organs. (iii) �Serotherapeutic
isopathy� or �serotherapy� (dilutions of hyperimmune serum). The book also
contains 42 personal observations and the rules of isopathic pharmacopraxis,
which is the starting point for a substantial renewal of the method.
In the twentieth century two
works devoted entirely to nosodes have been published: the first in 1910 by
H.C. Allen, entitled The Materia Medica of the Nosodes. The second is by the
Frenchman O.A. Julian, who first published Materia Medica der Nosoden in German
in 1960, later to come out in two French versions, one in 1962 entitled
Biothe�rapiques et Nosodes and the other in 1977 entitled Traite� de Micro-Immunothe�rapie
Dynamise�e. The above-mentioned book by O.A. Julian in 1960 was a success in
Germany, where it revived the study of nosodes.
In particular, R. Voll accorded therapy
with nosodes a central role in his diagnostic�therapeutic procedure called
electroacupuncture-organometry, and H.H. Reckeweg, the founder of
homotoxicology, made extensive use of nosodes and immunomodulators in his
biotherapy. The use of the nosode Meningococcinum as prophylaxis of meningitis
was suggested by others.
SUBSEQUENT DEVELOPMENTS OF HOMEOPATHY
The rapid initial spread of
homeopathy was probably due, on the one hand, to the fact that the orthodox
medicine of Hahnemann�s day and age was still extremely backward and lacked
truly effective therapeutic remedies, and, on the other, to the distinct
superiority of homeopathy in treating the various epidemics of typhoid fever,
cholera and yellow fever which raged across Europe and America in the 1800s.
Homeopathic medicine has
undergone substantial ups and downs in its historical development. The rapid
early boom throughout the world in the nineteenth century and its immense
popularity were due to the fact that the other modes of medicine practiced at
that time often used rather crude and painful means for a cure. A survey of the
periodicals and other literature of the first decades of the nineteenth century
reveals that in the medical practice among physicians of the orthodox
persuasion the most common methods of treatment were bloodletting, sulfur,
camphor, calomel and mineral medicines, mostly mercurial salts.
However, this rapid spread was
followed by a head-on clash with orthodox medicine, which stopped homeopathy in
its tracks and then led to its progressive decline, particularly in Western
countries, where in some cases it all but disappeared.
Over the past few decades,
however, we have been witnessing a steady recovery of homeopathic practice,
even in very advanced countries such as France, Germany, and Italy.
Hahnemann, right from the outset,
found himself faced with stern opposition from colleagues and even more so from
the apothecaries, who felt that he was undermining the foundations of their
profession: since he was recommending the use of small doses and was against
multiple prescriptions, this new medicine was perceived as a serious threat to
their profits.
Moreover, he was accused of
dispensing his own medicines and administering them to his patients, which was
illegal at the time. He was thus arrested in Leipzig in 1820, convicted and
forced to leave the city. He then obtained special permission from Grand Duke
Ferdinand to practice homeopathy in the town of Ko�then, where he continued to
work, write, and instruct his followers who were swiftly increasing in numbers
and spreading their wings further afield. At his death (1843), homeopathy was
known in all European countries (except Norway and Sweden), as well as in the
United States, Mexico, Cuba and Russia, and not long after his death it reached
India and South America. It was first introduced into Italy in 1822 thanks to
G. Necker who founded the Neapolitan School.
By the middle of the nineteenth
century, there were a large number of homeopathic journals, clinics, hospitals,
societies and pharmacies; homeopathic physicians could be found throughout the
world; and more than 20 faculties of homeopathic medicine were founded in the
United States. However, there were many controversies between the Hahnemann
school and the other trends of twentieth century medicine, particularly in
Germany. Furthermore, homeopathy itself also began to develop different
tendencies and conflicts, such as that between physicians who used albeit
diluted ponderal doses and those who insisted on extremely diluted/dynamized
preparations; that between those who gave only single medicines and those who
gave combinations; or that between those who combined homeopathic and
conventional medicines and those who relied exclusively on homeopathic
remedies.
Homeopaths had separated into two
groups even before the death of Hahnemann: one group considered itself the
representative of pure Hahnemann homeopathy, and recognized the founder as the
ultimate authority; the others formed a group of �scientific homeopaths� who
acknowledged Hahnemann as a brilliant innovator, but did not consider him
infallible or hesitate to question his opinions. The �scientific� conception of
homeopathy that developed during the nineteenth and early twentieth century was
largely due to the efforts of this second group of homeopaths, who encouraged
the greatest theoretical and experimental progress.
Early attempts to investigate the
principle of similarity on the experimental ground can be traced back to the
years around the end of nineteenth century, when H. Schulz published a series
of papers that examined the activity of various kinds of poisons (iodine,
bromine, mercuric chloride, arsenious acid, etc.) on yeast, showing that almost
all these agents have a slightly stimulatory effect on yeast metabolism when
given in low doses. He then came into contact with the psychiatrist R. Arndt
and together they developed a principle that later became known as the
�Arndt-Schulz law�, stating that weak stimuli slightly increase biological
responses, medium and strong stimuli markedly raise them, strong ones suppress
them and very strong ones arrest them.
Similar observations were
reported by several other authors in the 1920s and from their findings one can
conclude that the occurrence of inverse, or biphasic, effects of different
doses of the same substance was known before the era of molecular medicine.
This phenomenon is now well
recognized in cell biology, with a number of explanation at the molecular level
(e.g. different receptors for the same substance having different ligand
affinities and triggering transduction pathways) and in immunology, where the
systemic and local responses are known to depend on the dose in a complex way
(e.g. foreign antigens may sensitize the host but low doses of the same
substance may suppress the system if administered by oral route). We will go
back to these concepts in a subsequent paper dealing with the scientific models
of the similia principle. The delayed recognition of the possible contribution
of homeopathic ideas to mainstream medical science and, insistent attacks of
some homeopaths against allopathy are at least partially responsible for the
rejection of homeopathy by the majority of modern physicians and academic
circles.
It is generally agreed that one
of the greatest physicians in Germany at the time of Hahnemann was Christoph
Wilhelm Hufeland (1762�1836), a rich and magnanimous physician who was a friend
of Goethe and Schiller (Fig. 7). He was a pioneer of medical journalism and
dedicated his Journal der Praktischen Arzneikunde (which he edited for 40 years
and which subsequently took his name) to the correction of the medical
deviations of his time. Although being a leading representative of �official�
medicine, he also dealt extensively with the developments of homeopathy. His
works include��
Figure 7. C.W. Hufeland (1762�1836).
many references indicating his openness to homeopathic
ideas, such as:
The first reason inducing me to write is the fact that I
considered it incorrect and unworthy of science to ridicule or persecute the
new doctrine of homeopathy.
. . I find suppression and despotism in science repugnant;
here, the only rule should be freedom of spirit, basic research, the
confutation of hypotheses, the comparison of observations, adherence to facts
and not to personalities. (. . .) Homeopathy must necessarily be contested if
it intends to present itself as a general principle of every therapy. In fact,
if this affirmation were to be taken literally, it could seem to be the grave
of all sciences and human progress.
(. . .) But homeopathy is valid as a field of observation
and, instead of being repudiated, should be used as a special method of cure,
subordinate to the higher concepts of rational medicine. On the basis of my
personal observations, I am convinced that it can render a service not rarely,
but sometimes in a highly striking manner, particularly after the failure of
other treatments. (. . .) I am not in favor of homeopathy, but of the inclusion
of a homeopathic method in rational medicine. I would not speak of homeopathic
physicians, but of physicians that use the homeopathic method at the right time
and in the right place.
Unfortunately, the history of medicine during the second
half of the nineteenth and, particularly, the twentieth century was
characterized by bitter struggles between the �official� and Figure 7. C.W.
Hufeland (1762�1836).
��alternative� medical
worlds that made vain these hopes of Hufeland. As a result of an irrational
policy of reciprocal excommunication, the two disciplines failed to develop any
common points for a long time and continued along their own separate and often
conflicting ways. With some exceptions (e.g. the German school), homeopaths
have failed to scrutinize homeopathic concepts and theories in relation to
conventional biology and immunology, possibly because they feel that any
reductionist scientific approach is incapable of interpreting the greatness of
their �art�.
OPPOSITION TO THE DEVELOPMENT OF HOMEOPATHY
In the nineteenth century
homeopathy was immensely popular in the United States where major figures such
as Hering, Kent and Farrington were practicing. Homeopathy was taught at Boston
University and at the Universities of Michigan, Minnesota and Iowa. By the turn
of the century as many as 29 homeopathic journals were being published. The
year 1844 marked the founding of the American Institute of Homeopathy, which
thus became the first American national medical society.
Despite this, strong organized
opposition was soon forthcoming from �orthodox� medicine, which viewed the
growth of homeopathy as a major threat: homeopathy was calling into question
the very philosophical basis, clinical methodology and official pharmacology of
orthodox medicine. Right from the very beginning the new approach embodied a
strong critical attitude towards the use of conventional medicines, which were
judged to be harmful, toxic and counterproductive for the practice of
homeopathy, in that they were all based on suppression of symptoms. What is
more, good homeopathic practice called for a long apprenticeship and
individualization of treatment, both of which demanded more time than
physicians were normally prepared to give their patients.
The year 1846 marked the
foundation of the American Medical Association (AMA), one of the first
objectives of which was to combat homeopathy: homeopaths could not be members
of the AMA, and AMA members were not allowed even to consult a homeopath, the
penalty for this being expulsion from the Association; legal recognition was
denied to graduates with diplomas from universities with full professors of
homeopathy on their academic boards. In 1910, a classification of American medical
schools was drawn up (the Flexner Report) on the basis of criteria which
assigned high ratings to schools which placed the emphasis on a physicochemical
and pathological approach to the human body and strongly penalized the
homeopathic approach. The homeopathic colleges obviously obtained poor ratings,
and as only the graduates of schools with high ratings had their qualifications
recognized, this was a mortal blow to the teaching of homeopathy.
Of 22 homeopathic colleges
operating in 1900, only two were still teaching homeopathy in 1923. By 1950
there was not a single school in the United States teaching homeopathy and it
was estimated that there were only about a hundred practicing homeopaths,
almost all over 50 years of age, throughout the United States. For similar
reasons, there was also a parallel decline in homeopathic practice in Europe in
the early decades of the twentieth century.
We should not conclude, however,
that the decline of homeopathy was due to only political and economic reasons.
At least two other factors played
a decisive role, namely the internal struggles within homeopathy itself and the
new major scientific and pharmacological discoveries. As regards the splits in
the homeopathic world, there were disputes between the various schools over
dilutions (high or low potencies), over single or multiple prescriptions, and
over whether prescribing should be based on total symptoms or on the main
disease present. The various different schools developed their own
organizations, hospitals and journals, thus making it very hard even for
doctors seriously interested in learning about homeopathy to get their bearings
in this field.
A severe blow to homeopathic
theory was delivered by the chemical sciences and in particular by the law
formulated by Amedeo Avogadro (Fig. 8), that was published initially as a
hypothesis in 1811 and then tested experimentally by Millikan in 1909: as is
well known, this law establishes that one mole of any substance contains
6.02254 � 1023 molecular or atomic units. As a result, a simple calculation
demonstrated that dilutions of any substance beyond 1024 (24� or 12c in
homeopathic terms) presented an increasingly remote chance of containing even
only a single molecule or atom of the original compound. From this it was
obviously but a short step to ridiculing the use of homeopathic medicines, and
homeopaths were branded by their adversaries as being on a par with some kind
of esoteric sect. Such opinions have continued to be voiced virtually unaltered
up to the present day.
The decisive factor, however,
permitting conventional scientific medicine to prevail over homeopathy was its
own development as a science capable of identifying the causes of many diseases
and as a source of effective techniques and technologies for curing them.
Lister�s discoveries in the antiseptic field and the development of
anesthesiology greatly increased the success, indications and popularity of
surgery. While chemistry, physiology and pathology were making giant strides in
the theoretical sphere, the discovery of vitamin and hormone replacement
therapies and, above all, the advent of antibiotics, analgesics and
anti-inflammatory drugs enabled orthodox therapy to demonstrate its practical
superiority. The possibility of interpreting pathological phenomena rationally
on the basis of a scientifically validated model of the human body and the
availability of chemical, physical or technological means capable of repairing
defects detected with the utmost precision by increasingly sophisticated and
reliable instruments was (and is) altogether too attractive and convincing a
prospect to allow scope for exploring alternatives based on outdated and
mysterious theories.
HOMEOPATHY REVIVAL
As we have already stated, the
enormous progress of conventional medicine in this century has reinforced the
opinion that allopathic treatment by means of �opposites� is the only effective
form of treatment and, generally speaking, has also strengthened the view that
it is only a question of time before a treatment is found for every disease.
The great epidemics of infectious diseases have been defeated by a combination
of improvements in living conditions, hygiene, vaccinations and antibiotics.
Our knowledge of disease due to vitamin, enzyme or hormone deficiencies has
furnished new weapons in the struggle against diseases such as pernicious
anemia, dwarfism and diabetes. If it were not for the problem of finding
donors, transplants would already be routine therapy for a sizeable number of
diseases. Cortisone and its derivatives are solving many problems of immune
hypersensitivity. Recent developments in molecular biology give us good reason
to believe that not even the genetic sphere will be able to escape our
manipulative capability.
Against this background, one
cannot see any real scope for homeopathy, though at present its use is still
spreading. This spread of homeopathy is happening in countries such as Italy,
France and Germany, and parallels the renewed interest in homeopathy in many
other countries throughout the world.
Homeopathy is even more popular
in Asia, most notably in India, Pakistan and Sri Lanka. In the United States,
too, we are witnessing a revival of homeopathic practice: sales of homeopathic
medicines in the USA have been growing at an annual rate of 20�25% during the
1990s.
These considerations alone should
be enough to justify a greater commitment of official scientific institutions
towards monitoring and clinically verifying the efficacy of therapeutic agents
and measures adopted. A need is also felt for at least some teaching of the
basics of homeopathy to doctors trained in universities, since, at general
practitioner level particularly, patients often tend to be keenly interested in
homeopathy and to ask their general practitioners for information and advice on
the subject.
There may be any number of
reasons for the revival of homeopathy, despite the lack of university teaching
in the field and of support on the part of public health authorities
(homeopathic drugs are not available on the NHS), but it can hardly be
accounted for merely on commercial grounds. The main reason for the success of
the so-called �alternative� medicines lies in the fact that they offer
something which today�s physician is unable to provide. This can be traced, on
the one hand, to the greater degree of individualization of the treatment,
attention being paid to the human and psychological elements, which are
becoming increasingly neglected in this era of ultra-high-tech medicine; on the
other hand, it is due to the awareness that many of the challenges still facing
us today in the fight against disease call for a different approach from that
adopted to date.
In fact, the public at large and
also the medical profession itself are becoming increasingly aware that modern
medicine must come up with new means and new ideas for tackling problems. These
include contamination of the environment by toxic agents, ever-growing numbers
of diseases induced by increasingly potent drugs themselves, degenerative
diseases to which errors of diet or life-style contribute, allergies,
autoimmunity and immune deficiency, large numbers of neurological and
psychiatric diseases, psychosomatic disorders, and tumors. Despite undoubted
progress made over the past decades in these crucial fields of medicine,
despite the fact that we so often hear of new �major� breakthroughs� paving the way towards
achieving a definitive cure for this or that disease, and despite the fact that
our knowledge of the intimate mechanisms of the various diseases has increased enormously
as a result of techniques of molecular biology, it has to be admitted that, as
far as general practice and the vast majority of patients suffering from the
above-mentioned diseases are concerned, the actual practical benefit of such
knowledge is not exactly spectacular!
That this is not merely a
commercial phenomenon is also suggested by the fact that we are witnessing a
renewed interest on the part of scientists in experimental trials in this
field.
Studies are beginning to appear on the biological effects of
homeopathic drugs, as well as studies on the so-called �highdilution effect�,
or double-blind placebo-controlled clinical trials.
The debate in scientific circles is becoming increasingly
heated, and many researchers are setting themselves the objective of developing
reliable methods for tackling the problem.
Reilly�s group has published a
series of trials describing randomized and double-blind studies of patients
with chronic allergic rhinitis or bronchial asthma treated with homeopathic immunotherapy
(HIT). The studies involved administration of a 30c potency of the main
allergen or (in the control group) an indistinguishable placebo. Results
demonstrated a significant improvement of symptoms in the treated patients in
comparison with those receiving placebo (P � 0.0001). This study offered proof
that high homeopathic dilutions of antigens cannot be assimilated to a simple
placebo. However, as underlined by the authors themselves, this does not mean
that their proposed therapy is an efficacious homeopathic therapy for chronic
rhinitis (also because homeopathy requires individualized treatment).
These results have not yet been
confirmed by independent groups; on the contrary, a paper recently published by
Lewith and coworkers in the Br Med J describes apparently opposite results (the
homeopathic medicine caused a slight but statistically significant worsening
during the early phases of treatment than placebo). This latter study sparked a
considerable discussion in the same Journal. The reply of Reilly, the author of
previous (positive) studies on HIT, stated that the Lewith�s study was not
actually a reply of their work, because the patient population, the drug
administration, and the outcome measures were different. The debate on the
clinical effectiveness of homeopathy is still quite hot.
We now have the results of
studies that have used homeopathic remedies under well-known experimental
conditions, as well as conventionally produced experimental evidence indirectly
explaining homeopathic phenomena. The current scientific literature contains a
substantial body of evidence and examples that may provide new insights
improving our understanding of the principle of similarity and the action of
small (or highly diluted) doses of medicines, particularly on the immune system
and host defenses. These studies document and may clarify some of the specific
aspects of the biochemical regulatory mechanisms possibly underlying the
observed paradoxical phenomena. The �simile��brought back to its biological meaning
of the inverted, or paradoxical, effects of the same or similar compounds�can
operate under a number of experimental and reproducible conditions. Within the
framework of our current knowledge of living systems and modern investigational
techniques, it will be possible to reformulate the ancient principle with the
aim of constructing reasonable models that can be tested at different
biological levels, from cells to human beings.
Anyone who adopts an unprejudiced
position will discover that immunology and the whole of modern biology in
general can offer a considerable contribution to the understanding of
homeopathy in a framework that is not very different from the conventional
context. In other words, although it is true that some of the most reductionist
molecular lines of modern science are ultimately incompatible with the systemic
nature of homeopathic thought, it is equally true that many others are
perfectly compatible.
�
�Figure 8. A. Avogadro
(1776�1856).
(back
to content)
4.9 Electrohomeopathy w
Electrohomeopathy,
Electrohomoeopathy, or Mattei cancer cure is a derivative of homeopathy
invented in the 19th century by Count Cesare Mattei. The name is derived from a
combination of electro (referring to an electric bio-energy content supposedly
extracted from plants and of therapeutic value, rather than electricity in its
conventional sense) and homeopathy (referring to an alternative medicinal
philosophy developed by Samuel Hahnemann in the 18th century).
Electrohomeopathy has been defined as the combination of
electrical devices and homeopathy.
Lucrative for its inventor and
popular in the late nineteenth century, electrohomeopathy has been described as
"utter idiocy". Like traditional homeopathy, it is regarded by the
medical and scientific communities as pseudoscience and its practice as
quackery.
Electrohomeopathy was devised by
Cesare Mattei (1809�1896) in the latter part of the 19th century. Mattei, a
nobleman living in a castle in the vicinity of Bologna, studied natural
science, anatomy, physiology, pathology, chemistry and botany. He ultimately
focused on the supposed therapeutic power of "electricity" in
botanical extracts. Massei made bold, unsupported claims for the efficacy of
his treatments, including the claim that his treatments offered a nonsurgical
alternative to cancer. His treatment regimens were met with scepticism by
mainstream medicine:
HISTORY AND CRITICISM
The electrohomeopathic system is an invention of
Count Mattei who prates of "red," "blue," and
"green" electricity, a theory that, in spite of its utter idiocy, has
attracted a considerable following and earned a large fortune for its chief
promoter.
Notwithstanding criticisms,
including a challenge by the British medical establishment to the claimed
success of his cancer treatments, electrohomeopathy (or Matteism, as it was
sometimes known at the time) had adherents in Germany, France, the USA and the
UK by the beginning of the 20th century; electrohomeopathy had been the subject
of approximately 100 publications and there were three journals dedicated to
it.
Remedies are derived from what
are said to be the active micro nutrients or mineral salts of certain plants.
One contemporary account of the process of producing electrohomeopathic
remedies was as follows:
As to the nature of his remedies
we learn...that...they are manufactured from certain herbs, and that the
directions for the preparation of the necessary dilutions are given in the
ordinary jargon of homeopathy. The globules and liquids, however, are
"instinct with a potent, vital, electrical force, which enables them to
work wonders." This process of "fixing the electrical principle"
is carried on in the secret central chamber of a Neo-Moorish castle which Count
Mattei has built for himself in the Bolognese Apennines...The "red
electricity" and "white electricity" supposed to be
"fixed" in these "vegetable compounds" are in their very
nomenclature and suggestion poor and miserable fictions.
According to Mattei's own ideas
however, every disease originates in the change of blood or of the lymphatic
system or both, and remedies can therefore be mainly divided into two broad
categories groups to be used in response to the dominant affected system.
Mattei wrote that having obtained plant extracts, he was "able to
determine in the liquid vegetable electricity".
Allied to his theories and
therapies were elements of Chinese medicine, of medical humours, of apparent
Brownianism, as well as modified versions of Samuel Hahnemann's homeopathic
principles. Electrohomeopathy has some associations with Spagyric medicine, a
holistic Philosophy medical philosophy claimed to be the practical application
of alchemy in medical treatment, so that the principle of modern
electrohomeopathy is that disease is typically multi-organic in cause or effect
and therefore requires holistic treatment that is at once both complex and
natural.
A symposium took place in Bologna
in 2008 to mark the 200th anniversary of the birth of Cesare Mattei, with
attendees from India, Pakistan, Germany UK, and the USA. Electrohomeopathy is
practised predominantly in India and Pakistan (although it is not a recognised
healthcare discipline in India), but there are also a number of
electrohomeopathy organisations and institutions worldwide.
(back
to content)
4.10 The History of Magnetism in Medicine w
Urs Ha�feli
1.1.1 ORIGINS
Although magnetic effects such as
the ��northern lights�� in the northern hemisphere have been observed for
thousands of years, it was not until the discovery of iron smelting, at around
1200 BC, that a body of knowledge on magnetism began to develop. The first
effects of magnetism were observed when the smelted iron was brought close to
the iron oxide in the chemical form of FeOFe2O3 (Fe3O4), a natural iron ore
which came to be known as lodestone or magnetite.
The origin of the term
��magnetite�� is unclear, but two explanations appear most frequently in the
literature. In one of these, magnetite was named after the Greek shepherd
Magnes, who discovered it when the nails on the soles of his shoes adhered to
the ore. In the other explanation, magnetite was named after the ancient county
of Magnesia in Asia Minor, where it was found in abundance.
The first treatise on magnetized
needles and their properties (see Fig. 1.1) was presented by Petrus Peregrinus
in 1289 (Peregrinus, 1269). This treatise clearly documented a number of
magnetic properties including that: (1) magnetic forces act at a distance; (2)
magnetic forces attract only magnetic materials; (3) like poles repel and
unlike poles attract; and (4) north poles point north, and south poles south.
Equipped with this knowledge, the medieval Europeans navigated the globe,
discovering and conquering countries as they went.
Peregrinus, however, failed to
note that the Earth itself is a magnet. Yet it was not until 1600 that this
discovery was finally made by William Gilbert, a physician of Queen Elizabeth
I. In order to arrive at this conclusion, Gilbert performed numerous
experiments that separated hearsay from truth, documenting them in his book De
magnete along with a summary of the knowledge of the time about magnetism and
electricity (Gilbert, 1600). Gilbert�s systematic and scientific treatise is
considered by many to be one of the first great works in science (Butterfield,
1991) (see Fig. 1.2).
1.1 THE HISTORY OF MAGNETISM IN MEDICINE
Fig. 1.1. One of Petrus Peregrinus� inventions is this
��Astrolabium��, an oval lodestone mounted inside a wooden box. The four points
of the compass and 360 subunits were painted on the inside of the box. This instrument
was placed in a bowl of water to determine the azimuth of the sun, for example,
and the angle was read after the astrolabium had stopped moving.
1.1.2 FIRST MEDICAL USES OF MAGNETS
Thales of Miletus, the first
Greek speculative scientist and astronomer (ca. 624�547 BC) was also the first
to make a connection between man and magnet. He believed that the soul somehow
produced motion and concluded that, as a magnet also produces motion in that it
moves iron, it must also possess a soul. It is likely that this belief led to
the many claims throughout history of the miraculous healing properties of the
lodestone.
|
�
|
Fig. 1.2. The terrella (spherical lodestone), and the
location of its poles from Gilbert�s book De Magnete. The magnetic versorium (compass
needle) on top of the sphere is pointing along a meridian circle; the versorium
at D points directly to the center of the sphere and hence to the pole A, in
contrast to the versorium at E.
Medical references to magnetism
were made by Hippocrates of Cos (ca. 460�360 BC), who used the styptic iron
oxides magnetite and hematite to stop bleeding and to control hemorrhage
(Mitchell, 1932). Unraveling the true early medical applications of magnetite
as described by Hippocrates and his scholars is, unfortunately, complicated by
the two meanings of the same term. In particular, magnetite overlaps with the
older term ��magnesite��, a magnesium carbonate with laxative properties.
In the first century, Pliny the
Elder (23�79 AD), a Roman scholar, collected and condensed the entire knowledge
of the time into a thirty-seven-volume encyclopedia, which was used for the
next 1700 years. Amid its wealth of information lies a description of the
treatment of burns with pulverized magnets. Pliny, however, failed to
discriminate fact from fiction, and included much folklore and superstition in
his writings. He also theorized that ��sympathies and antipathies�� were the
cause of magnetic phenomena, a viewpoint which was shared by Galen of Pergamum
(129�199 AD). Galen compared the lodestone to cathartic drugs which attract
certain ��qualities�� such as bile and phlegm, to drugs which remove thorns and
arrow-points or draw out animal and arrow-tip poisons, and to ��corn��, which
is better able to draw water into itself than the sun�s heat is to draw water
out of it (Brock, 1916). The same attracting properties of lodestone were
advocated by Dioscorides of Anazarbos in the first century in his encyclopedia
of medical matter. He recommended their external use for ��drawing out gross
humors�� (Gunther, 1934).
When magnetite was applied
externally, this was either as the unbroken lodestone or in pulverized form,
compounded with other ingredients, under the name of Emplastrum Magneticum. The
usual practice seems to have been to bind the lodestone or magnetic plaster
directly to the affected body part. This technique was thought to be
efficacious in treating diseases such as arthritis, gout, poisoning, or
baldness. Lodestones were even thought to have strong aphrodisiac potency
(Mourino, 1991).
Although most ancient medical
uses of magnetite were external, it was also promoted for internal applications
by the Egyptian physician and philosopher Avicenna (980�1037 AD). Avicenna
recommended using the magnet in doses of one grain as an antidote for the
accidental swallowing of poisonous iron (rust). The pulverized magnet was often
taken with milk, and the magnetite was believed to render the poisonous iron
inert by attracting it and speeding up its excretion through the intestine.
This remedy may have worked as a consequence not only of its intended mechanism
but also because it induced vomiting (Stecher, 1995).
Albertus Magnus (1200�1280), in his book Mineralia,
recommended the same milk/magnetite mixture for the treatment of edema (Magnus,
1890).
1.1.3 USE OF ATTRACTING FORCES OF MAGNETS IN MEDICINE
The earliest known account of the
surgical use of lodestone is believed to be found in the writings of Sucruta, a
Hindu surgeon who lived around 600 BC (Hirschberg, 1899). Sucruta wrote in his
book Ayur- eda that the magnet which is in Sanskrit called ��Ayas Kanta�� � the
��one loved by iron�� � can be used to extract an iron arrow tip. Sucruta
specified that the extraction works best if ��. . . the piece of iron is
embedded parallel to the fibers of the tissue, does not contain any ears
(barbs), and the opening is wide��.
Sucruta�s applications were not
explored again for almost 2000 years. Gilbertus Anglicus wrote around 1290 in
his earliest medical work that ��. . . certain surgeons apply adamant or
magnet, if iron is concealed in the flesh�� (Anglicus, 1290). This concept was
described in a publication from 1640 which suggested that iron in the form of
iron filings should be fed to a patient with a hernia (Kirches, 1640). The
appropriate placing of an externally attached magnet was then expected to
attract the iron, thus drawing in and restoring the protruding intestine. The
successful employment of this treatment was reported some years later by
surgeon Ambrose Pare` , a claim which he asked doubters to take at face value
��. . . on the faith of a surgeon�� (Johnston, 1678)!
Other accounts of successful
magnetic extractions also appeared, including the description by G. Bartisch.
In 1583, he wrote: ��A good cream, in case iron, steel or stone had leaped into
your eyes, is made from 3 lots of rabbit fat, 1 lot of wax, 1 quint of yellow
agstone and 1/2 a quint of lodestone. Such a cream, if applied over your eyes
in form of a plaster, helps.�� Hirschberg, who cited this description
(Hirschberg, 1899), added: ��Of course, it doesn�t help at all!�� A similar
dose of skepticism may be appropriate in the case reported by Andry and Thouret
(Andry, 1779) who reported that around 1635 surgeons succeeded in bringing the
point of a knife that had been swallowed accidentally to the integuments with
the aid of the emplastrum magneticum. The point was then surgically removed
from that location.
Gilbert cited such claims at the
end of the 16th century, and categorically denied them: Lodestone ground into a
plaster would not be strong enough to extract large iron objects; the same
plaster applied to the head could not cure headaches; if lodestone were used
with incantations it would not cure insanity; magnets applied to the head would
not cause unchaste wives to fall out of bed; and lodestones would draw neither
the pain out of gout nor poisons from other parts of the body (Butterfield,
1991). Gilbert believed that the only effect of this plaster was to heal
ruptured tissues by drying them out. What magnetite (or iron) was good for,
Gilbert maintained, was chlorosis, as patients with this disease were thought
to benefit from small doses of iron filings mixed with strong vinegar. Gilbert
found that this mixture also helped older patients with splenomegaly, chronic
malaria and anemia � diseases not uncommon in the East Anglian swamps of
England at that time.
More believable accounts of the applications of magnetic
forces � at least in terms of present-day standards � began to appear in the
17th century. For example,
Andreas Frisii described a case
in which a needle accidentally lodged in the side of a person�s throat was
removed by a traveling mountebank, as ��. . . fools rush in where wise men fear
to tread�� (Frisii, 1670):
�
Fig. 1.3. Hand-held electromagnets used for the removal of
magnetic objects from the eye. Left: The original Hirschberg magnet. Right: A further
development of Dr. Hubbell. The needle-like tip is placed, preferably through
the entry wound, as close as possible to the foreign iron or steel particle.
The magnet is then turned on and the foreign body pulled out.
iris of the eye, which I endeavored to push out with a small
spatula, but could not.
But on applying a lodestone, it
immediately jumped out.�� Again more than 80 years later, the use of lodestone
for eye surgery was reported by Dr. Morgagni in a case involving the cornea
(Morgagni, 1761). A more spectacular case involving the removal of iron
fragments from behind the iris was reported by Dr. Nicolaus Meyer of Minden,
Germany, in 1842. According to Hirschberg, one of the great experts in the
field, this was the first case on record for the removal of pieces of iron from
the interior of the eye (Hirschberg, 1883). The first case in America, was
performed by Dr. Alex. H. Bayly of Cambridge, Maryland (Bayly, 1886). The
magnet used in this case was an ��artificial�� or horse-shoe magnet.
Since 1879, the use of magnets
has become the established procedure for the removal of magnetic objects from
the interior of the eye (Tost, 1992). In that year, Dr. Julius Hirschberg
reported the first ophthalmic use of electromagnets (Hirschberg, 1880). His
magnet had the shape of an ��electric handmagnet�� and was used like forceps,
in close proximity to the foreign metallic objects (see Fig. 1.3). Further
developments in electromagnets by the Swiss ophthalmologist Otto Haab led to
extractions in which the magnet was placed at greater distance from the eye
(Haab, 1892). He used Ru�hmkorff �s apparatus, a 130-kg heavy electromagnet
with a small pointed horizontal protruding tip, designed at the Federal
Institute of Technology in Zurich. The patient sat in front of the tip with
their head fixed in a 90cone.
The cone was then moved by the physician into the extraction
position. This magnet produced forces of 11.3 mT (@105 dyne) at a distance of 5
mm from the tip.
Due to the size of this magnet, it was later termed ��the
giant magnet�� (Fig. 1.4).
�
Fig. 1.4. Dr. Haab�s giant magnet for the removal of iron or
steel foreign bodies from a patient�s eyes. The magnetic field lines around the
tip of the instrument are shown to the right.
Haab and Hirschberg�s different
approaches to the removal of magnetic objects from the eye resulted in a
22-year-long (from 1892 to 1914) scientific battle waged through letters and
articles. Their views differed with respect to the type of magnet to use, the
position of the patient, and the route of removal of the foreign objects.
Haab favored the direct removal
of small objects through the front of the eye, ��der vordere Weg��, while
Hirschberg preferred removal through the back of the eye, ��der hintere Weg��.
Both methods were known to be associated with peeling of the iris, a serious
side effect, although it was not until 1970 that both techniques were shown to
be equally risky (Springer, 1970). It is no longer necessary to establish the
superiority of either method since the use of magnets to remove objects from
the eyes is currently declining, due to advancements in modern eye surgery.
Magnets have been employed to
remove iron or steel objects not only from the eyes, but also from other body
parts. Swallowed pins and nails are commonly extracted magnetically from the
stomachs of unlucky children, and shrapnel drawn from the surface wounds of
war, bomb or crime victims. The extraction of a safety pin from a child�s
stomach is illustrated in Figure 1.5 (Luborsky et al., 1964).
Another interesting approach to render ingested and potentially
dangerous metallic objects harmless is seen in the application of magnets in
veterinary medicine.
Grazing cows often swallow sharp steel objects such as the
barbs from barbed wire,��
Fig. 1.5. Removal of an open safety pin from a patient�s
stomach. A probe is ��swallowed�� by the patient (left) and maneuvered by the physician
until the tip is near the rounded end of the pin. When the tip of the probe is
magnetized, it attracts the pin (right). With the pin in position, the point is
less likely to do damage to the digestive tract as it is pulled out.
(Photograph courtesy of F.E. Luborsky; Luborsky et al., 1964).
or pieces of wire from bales of
hay. In order to prevent these sharp objects from damaging the stomach and
intestinal walls, the cows are forced to swallow a ��cow magnet��, a 7 cm-long
and 1 cm-diameter rod Alnico magnet covered with an anticorrosive plastic
coating. The cow magnet remains in one of the cow�s stomachs, where it attracts
any steel or iron objects that pass by, rendering them nondangerous and
preventing the so-called ��hardware disease��. The magnets can be easily
retrieved when the cow is slaughtered, and do not appear to have any adverse
side effects (Livingston, 1996).
1.1.4 TREATMENT OF NERVOUS DISEASES AND MESMERISM
The first person to mention the
topical application of a magnet in nervous diseases was Aetius of Amida
(550�600 ad), who recommended this approach primarily for the treatment of
hysteria, and also for gout, spasm, and other painful diseases.
Some five centuries later, abbess
Hildegard of Bingen (1098�1179) � who was said to have received the words for
her books directly from God � described the use of plants and minerals (stones)
for medical purposes and devoted a whole chapter to the lodestone. Her method
of using the lodestone was somewhat new, in that the magnet had to be held in
the patient�s mouth to remedy fits of anger or rage, to make fasting bearable,
and to keep lies and maliciousness at bay (Riethe, 1961).
Several hundred years later, the
Swiss Theophrastus Bombast von Hohenheim (1493�1541), a doctor and alchemist,
reasoned that since magnets have the mysterious power of attracting iron, they
should also be able to attract diseases from the body. He was often criticized
for his beliefs and was mockingly called ��Paracelsus��, which means ��greater
than Celsus�� (Celsus was a famous Roman doctor who lived around 25 BC to 50
AD); he finally adopted the name Philippus Aureolus Paracelsus.
In his work, Volumen Medicinae
Paramirum, Paracelsus described exact procedures to transplant diseases from
the body into the earth by using a magnet. The choice of magnetic pole was
important for these procedures. In his treatment of epilepsy � a disease in
which there is ��. . . more nervous fluid in the brain��, ��. . . the repulsing
pole of a magnet�� was ��. . . applied to the head and the spine��, and ��. . .
the attracting pole to the abdominal region��. Paracelsus further extended the
use of magnets to leucorrhea, diarrhea and hemorrhages, for which his procedures
were often successful. However, the effectiveness of his methods could probably
be attributed more to the amazing powers of human imagination than to
magnetism.
Reports from England during the
1740s regarding the production of strong artificial (not lodestone) magnets led
to renewed interest in the use of strong magnets for healing purposes. It is
unclear who was responsible for the introduction of steel magnets, but evidence
points to it being either Gowin Knight, a physician; John Canton, a schoolmaster
and amateur physicist; or John Michell, an astronomer.
The term ��horse-shoe magnet��,
however, came from Michell. One of the people who experimented with the new
magnets was Father Maximilian Ho�ll (1720�1792), a Jesuit priest and astronomer
at the University of Vienna. In 1774, Ho�ll became friends with the then
40-year-old physician Franz Anton Mesmer, to whom he gave some of these
magnets. By applying them to his patients � who mainly had symptoms of
hysterical or psychosomatic origin � Mesmer achieved many seemingly miraculous
cures.
Mesmer first conjectured that the
magnets worked by redirecting the flow of the universal ��fluidum�� from the
atmosphere or the stars to the patients� bodies. He soon discovered, however,
that magnets could be replaced by nonmagnetic objects such as paper, wood,
stone, and even humans and animals. This led Mesmer to coin the term ��animal
magnetism�� for the fundamental biophysical force he considered responsible for
the free flow of fluidum. Disease originated from an ��obstructed�� flow, which
could be overcome by ��mesmerizing�� the body�s own magnetic poles and inducing
a ��crisis��, often in the form of convulsions. The patients� health and
��harmony�� could thus be restored (Mourino, 1991). A graphic account of the
treatment of Mesmer�s first patient was given by Macklis (1993).
Mesmer�s theories and, probably
even more so, his rapidly gained fame soon enraged the medical faculty of
Vienna. In 1777, they used the case of Maria Theresia von Paradies as the
reason to expel him both from the fraternity of medicine and from the city of
Vienna. Maria Theresia was a blind child piano prodigy who regained her sight
after being treated by Mesmer. Unfortunately, she simultaneously lost her
equilibrium as well as her musical talents. Her parents were angered and
demanded that Mesmer stop the treatment. The child�s reaction to the suspension
of treatment was spectacular, in that she dropped immediately to the floor in
convulsions, blind once again.
1.1.4 TREATMENT OF NERVOUS DISEASES AND MESMERISM 11
�Fig. 1.6. Mesmer�s
tub, the first medical device from 1780 designed for the biomagnetic treatment
of men and women. (Illustration courtesy of Dr. A. Dittmar, Lyon).
Evicted from Vienna, Mesmer went
to Paris, where his theories of ��animal magnetism�� were eagerly embraced. He
used his many talents in a curative, psychological way (Darnton, 1972), and his
clinic soon became famous for spectacular spiritualistic sessions. In one of
his best-known treatments, patients bathed in magnetized water in an oval
vessel called the ��Baquet de Mesmer�� (Mesmer�s tub) (see Figs. 1.6 and 1.7).
With time Mesmer�s theories
evolved from his initial teachings, developing into an empirical psychological
healing science, a mix of hypnotism and psychotherapy, imaginative and
psychosomatic medicine. Taken up by many healers and quacks, Mesmer�s ideas
were promoted in many books, and periodicals were soon crowded with reports of
the successful treatment of nervous maladies. King Louis XIV of France was skeptical
about these reports of animal magnetism and requested an investigation from
Benjamin Franklin and Antoine Lavoisier. After having performed 16 different
experiments � many of them in a blinded setup � the two scientists showed in
1784 conclusively that magnetism had nothing to do with the reported healings
(Shermer, 1997). Many of the beneficial effects attributed to the use of
magnets in the treatment of nervous diseases were evidently due to the
increased suggestibility of the subjects to whom this novel remedy was applied.
In such cases, with the necessary amount of faith, almost anything is a remedy.
Even today, magnets continue to
be advertised as health-promoting, and are sold in amazing numbers and in many
different forms and shapes for all purposes. Recent advertisements, for
example, claim that magnetic bracelets cure headaches, and that magnetic
mattresses, shoe inserts, and belts have beneficial health effects by
influencing the body�s magnetic field. The use of supermagnets (neodymiumiron-
boron magnets) is advocated as a pseudo-scientific cancer cure. Some of these
interesting claims are described in more detail by Livingston (1996).
�Fig. 1.7. Mesmer�s
tubs existed in different sizes, with large versions in great demand by the
high society and the court of King Louis XVI from France during the 18th
century. (Illustration from an engraving from 1779, collection of M. Gaston
Tissandier; courtesy of the Lyon Historic Museum of Medicine, University Claude
Bernard, Lyon).
1.1.5 OTHER MEDICAL USES OF MAGNETS AND MAGNETISM
During the past 20 years, the
medical use of magnets has spread to fields as diverse as dentistry,
cardiology, neurosurgery, oncology, and radiology, to mention only a few. The
scientific advancements that made these new applications possible include the
evolution and miniaturization of electromagnets, the development of
superconducting electromagnets at Bell Laboratories in 1961, and the
introduction of strong permanent magnets made of samarium-cobalt between 1960
and 1970 (McCaig and Clegg, 1987) and of neodymium-iron-boron (NdFeB) in 1983
(Kirchmayr, 1996; Goll and Kronmu�ller, 2000).
The new, much stronger magnetic
materials allowed the construction of miniaturized magnets and electromagnetic
coils, the smallest of which is so tiny that it could fit into the tip of a
vascular catheter (Hilal et al., 1974). These small catheters permitted
intravascular guidance from outside of the body with a strong magnetic field,
and have been used clinically both for monitoring intracranial
electroencephalograms and for producing electrothrombosis of inoperable
arterial aneurysms.
Furthermore, with the help of such a catheter, a discrete
embolus or an intravascular adhesive can be deposited for the selective
occlusion of vascular lesions.
In 1979, a magnetically fixable
catheter that electrically stimulated the heart was clinically tested in
patients with bradycardic arrhythmia, providing temporary pacemaker therapy
(Paliege et al., 1979). The design included an electrode almost identical to
those of the stimulation catheters, except that its 18 mm-long and 0.9
mmdiameter tip was made from soft iron coated with gold rather than from
platinum or iridium-coated NiCr-steel. It was thus ferromagnetic. Using this
catheter together with an external magnet, a stable stimulation position was
reached in the��
|

|
Fig. 1.8. (a) The Niobe3 system, a magnetic navigation
system built by Stereotaxis Inc., St. Louis, Missouri, USA. The system is based
on two large permanent magnets that, upon proper rotation and movement, are
able to precisely direct a magnet-tipped guide wire (b) or electrophysiology
mapping catheter (c) within the patient�s vascular system. This system was
approved by the FDA in the USA in 2003 for multiple interventional cardiology
and electrophysiology procedures.
right auricle of 17 out of 19 patients, and in the right
ventricle of 28 out of 32 patients.
A more recent report described
the successful diagnosis of a complex congenital heart disease through the use
of a catheter magnetically guided through a neonate�s heart (Ram and Meyer,
1991). As the distance from a baby�s heart to the skin above is relatively
small, an appropriately placed magnet was able to direct the magnetic catheter
tip into the right ventricle, thus allowing for the injection of a contrast
agent.
The magnetic guidance of catheters and similar devices in
adults requires the use of higher magnetic fields and field gradients than
those employed with children.
One system which attains the
required fields is the magnetic-implant guidance system developed for
stereotactic neurosurgery (McNeil et al., 1995a, b). This system made use of
very strong superconducting magnets to deliver a small magnetic NdFeB capsule
within the brain with an accuracy of 2 mm. The capsule was moved by six
independently controlled superconducting coils mounted in a helmet, and
described to be used, in the future, to deliver radioactivity, heat, or
chemotherapeutic drugs to a tumor in the brain.
During the early 2000s, the
company Stereotaxis Inc., in St. Louis, Missouri, USA, further developed this
system by replacing the superconducting electromagnets with easier to maintain
NdFeB permanent magnets. In this new setup, the magnets are placed in a housing
a few meters away from the surgical table. When the patient is ready to undergo
the navigation of surgical guidewires and catheters
(Fig. 1.8b and c), the two
magnets in their housing are rotated into place for magnetic navigation (Fig.
1.8a). The magnetic force vector established under computer�
�Fig. 1.9. Using an
alternating magnetic field of 100 kHz, the magnetic field applicator MFH 300F
(MagForce Applications GmbH, Berlin, Germany) is able to induce hyperthermia in
tumors containing magnetic nanoparticles. Clinical trials are currently being
performed (Jordan et al., 2001; Gneveckow et al., 2005).
and joy stick control by the
surgeon then guides a catheter with a magnetic tip to chosen positions in the
heart or coronary vasculature. For this purpose, the two magnets can be rotated
independently and turned from one side to the other inside their housing, thus
establishing precise force vectors with a 360-degree control over the catheter
tip and an accuracy within 1 mm. With this system, the company hopes to improve
on cardiovascular care through the performance of more complex intravascular
procedures. Since 2003, when the FDA approved the Niobe1 System, multiple
interventional cardiology and electrophysiology procedures can now be
performed. These include the placement of a catheter against the wall of a
beating heart in order to record its electrical activity and to identify heart
tissue that is the source of the arrhythmia. Future applications currently
being investigated by Stereotaxis Inc. include the ablation of atrial fibrillation,
the repair of chronic total occlusion, the placement of percutaneous cardiac
bypass grafts, the repair of mitral valves, and the drug delivery of angiogenic
factors to diseased areas in the heart.
Rather than using the magnetic field of a magnet to move
ferromagnetic substances to a target location, a patient�s own blood flow can
accomplish this task.
An externally applied magnet
which produces a strong local magnetic field can then be employed to stop these
magnetic substances at or in the target organ (e.g., a tumor). The magnetic
substances � preferentially in the form of nanospheres or microspheres � thus
become concentrated in the target area. The spheres, which can be filled with
either chemo- or radiotherapeutic drugs, then produce their effects either by
releasing the drug or by blocking the vessels and capillaries (embolization)
(Poznansky and Juliano, 1984).
In addition to the embolization
effect, the application of selective radiofrequency heating (similar to a
microwave) to the area containing the magnetic microspheres can increase the
tumor cell killing even further. First results of this approach using
ferrosilicone were reported in 1976 by Rand et al. The systemic toxicity of
this method is very low (Barry et al., 1981); furthermore, it can be combined
with chemoembolization, as carried out by Sako for the treatment of liver
tumors (Sako et al., 1985).
Developments by Jordan and Chan led to the current
��magnetic fluid hyperthermia�� (MFH) application of single domain,
dextran-coated magnetite nanoparticles in tumors (Chan et al., 1993; Jordan et
al., 1993). Since 2003, Jordan has been conducting a clinical Phase II trial of
a combined magnetic hyperthermia and radiation therapy (Jordan et al., 2001;
Gneveckow et al., 2005) using the magnetic field applicator MFH 300F built by
his company MagForce Applications GmbH in Berlin,
Germany (Gneveckow et al., 2004).
The magnetic field applicator (Fig. 1.9) runs at 100 kHz and produces a
magnetic field strength of up to 18 kA m 1 in a cylindrical treatment area of
20 cm diameter. The first clinical results were presented in 2004 at the 5th
International Conference on the Scientific and Clinical Applications in Lyon,
France. Eight patients had been treated for cervix (n � 2), rectal, and
prostate (n � 2) carcinoma, chondrosarcoma, rhabdomyosarcoma, and liver
metastasis. The magnetic particles were injected locally directly into the
tumors.
The treatment, which increased
the tumor temperature to 43�50 C, took 60 min per session and was repeated from
two to eleven times. No additional applications of magnetic particles were
necessary after the initial injection. The magnetic fluid hyperthermia was very
well tolerated, and none of the patients stopped the treatment. There was no
pain and no burns, but some discomfort was felt due to excessive tumor heating
(transpiration, heat sensation). Of the eight patients, six showed local
control with no recurrent growth of the tumor, while the other two showed
complete remission (at 9 and 14 months after treatment, respectively).
These results are very promising, however, and this topic
will be discussed further in Chapter 4, Section 4.6.
In the field of dentistry,
magnets are most commonly applied to aid in the retention of oral and
maxillo-facial prostheses. The first treatment in orthodontics was reported in
Holland in 1953 by Dr. Crefcoeur (Duterloo, 1995), since when magnets have been
used for the treatment of unerupted teeth and tooth movement, as well as for
the expansion, fixed retention, and correction of an anterior open bite. It
seems that a prolonged constant force exerted by implanted rare-earth magnets
provides effective tooth movement (Daskalogiannakis et al., 1996).
Other retention applications
include the use of small rare-earth magnets to keep eyelids closed during sleep
in patients suffering from facial paralysis or, conversely, to keep lids open
during waking hours in patients with drooping eyelids, such as those with
muscular dystrophy.
Magnetic intrauterine devices
(IUD) for use in contraception have recently been developed (Livesay, 1987).
The nonmagnetic versions of such devices often have a�
�
Fig. 1.10. The Isolex4 300i Magnetic Cell Selection System
is the only FDA-approved product in the USA specifically for removing tumor
cells in stem cell transplants.
string which extends from the
uterus into the vagina; this is used by the gynecologist to remove the device.
However, some studies have suggested that this string provides an entry path
for bacteria and other organisms, and increases the chances of uterine
infections. The addition of a small rare-earth magnet to the IUD allows for the
string to be omitted. The IUD�s correct position can be detected magnetically
from the outside and removed using an extractor.
A recent ex-vivo application of
magnetism in medicine is the purification of bone marrow from tumor cells with
magnetic microspheres. In this procedure, the bone marrow is extracted from the
patient prior to the use of conventional cancer therapy.
Following high-dose treatment
with radiotherapy and/or chemotherapy, the patient is rescued with an
autologous bone marrow transplantation. In order to ensure that the patient�s
own bone marrow is free of cancer cells at the time of transplantation, a
purification procedure is performed. This procedure, which was developed during
the early 1980s and uses monoclonal anti-tumor antibodies conjugated to
magnetic polystyrene microspheres, has now become standard (Treleaven et al.,
1984; Treleaven, 1988). An initial purification system based on this technique,
the Isolex 300i from Baxter (Fig. 1.10), was approved by the FDA and introduced
into general therapy in 1999.
The medical use of magnets is not
confined to treatment approaches, but also extends to the most powerful modern
diagnostic methods such as positron emission tomography (PET) and magnetic
resonance imaging (MRI). In PET, magnets are used in a cyclotron to produce
short-lived radioisotopes such as 15O. These radioisotopes, when injected into
a patient and imaged with the PET system, allow determination of the
biodistribution and biochemical functioning of different organs and tissues. In
contrast, MRI utilizes the magnetic properties of the elements, and is used
extensively for three-dimensional, noninvasive scans of the patient�s body; indeed,
it is currently the most important diagnostic method available. The history,
principle and applications of MRI are covered extensively in Chapter 3.
1.1.6 THE INFLUENCE OF MAGNETIC FIELDS ON MAN
The human body is composed of
atoms of different elements surrounded by water molecules. These atoms react to
magnetic and electric forces and fields, and this may lead to, for example, a
net-nuclear magnetization of a person when placed in a clinical MRI machine. It
is therefore easy to imagine that magnetic and electromagnetic forces could
alter physiologic functions, induce effects, or influence the organism in
either a positive or negative way. Although the extent and importance of these
phenomena has been under investigation for the past 100 years, the effects
observed have generally been minimal and seldom statistically significant. A
report of the American National Research Council which examined more than 500
studies spanning 17 years of research concluded, in 1996, that ��No conclusive
evidence shows that exposures to residential electric and magnetic fields
produce cancer, adverse neurobehavioral effects, or reproductive and
developmental effects�� (National Research Council, 1997). A more succinct
overview, but with the same conclusions, was provided by Tenforde (2003).
When investigating magnetic
effects on humans, two different magnetic field ��types�� are generally
distinguished: (1) a static magnetic field, which exists around a large magnet;
and (2) a magnetic field that is pulsed at frequencies higher than 10 Hz, often
abbreviated as EMF (electromagnetic fields). The study of these effects is
termed ��biomagnetism��, some sub-fields of which are highly controversial,
while others have already been established in medical applications.
Most scientists agree that static
magnetic fields of up to 10 Tesla have no obvious effects on long-term plant
growth, mouse development, body temperature, or brain activity (Barnothy et
al., 1956; Barnothy and Barnothy, 1958; Maret et al., 1986).
Such conclusions echo findings
made more than a century ago, at which time, Mr. Kennelly � the chief
electrician at the Edison Laboratory � wrote, after exposing a volunteer to 27
000 times the magnetic field of the Earth, that, ��. . . the human organism is
in no wise appreciably affected by the most powerful magnets known to modern
science; neither direct nor reversed magnetism exerts any perceptible
influence upon the iron contained in the blood, upon the
circulation, upon ciliary or protoplasmic movements, upon sensory or motor
nerves, or upon the brain.��
(Peterson and Kenelly, 1892) (Fig. 1.11).
The lack of any apparent effects
of strong magnetic fields on humans placed near powerful magnets does not imply
that there are no effects at all. It would�
Fig. 1.11. Field magnet used in the studies of magnetic
effects on dogs at the Edison laboratory (humans were not mentioned in the
original legend!). The powerful attraction of bolts and chains is noticeable.
The circular door at the side was made from brass.
also be foolish to conclude that
humans have no magnetosensitive organs. During the past years, evidence has
been mounting that not only do pigeons (Keeton, 1971), bees (Kirschvink et al.,
1992a) and fin whales (Walker et al., 1992) possess magnetic receptors, but
humans might also (Kirschvink et al., 1992b). Chains of magnetite particles
similar to those known from magnetic bacteria and algae have been found �
chains which supposedly are either a part of, or form the magnetosensitive
organ itself. Several research investigations have been conducted in an attempt
to show that humans have a ��magnetic sense��. One study reported an experiment
in which students were driven around blind-folded and then asked to point in
the direction of their dormitories. Those students who used only their natural
��magnetic sense�� had a higher success rate than those whose ��magnetic
sense�� had been deceived by the field of a magnet attached to their heads
(Baker, 1989).
Clearly, further research is needed in this area as the
results are often contradictory and suggest several interpretations.
Research indicates that humans
are sensitive to small changes in magnetic field gradients, but not to the
overall magnetic field (Rocard, 1964). Evidence supporting this has come from
studies of the dowser reflex. A dowser, a person holding firmly onto a divining
rod (see Fig. 1.12) will, under certain physical conditions, experience a force
which results in an involuntary upward or downward movement of their rod. To
skeptics the movement appears illusory, to believers it appears magical, but
the effect has been consistently reported over the past 70 years by a number of
authors. In the most-often performed experiment, a group of dowsers was made to
walk along the same stretch of street. At points within 1 or 2 m of each other,
they all had their divining rods pulled down to the earth.
Magnetic field measurements have
shown that the dowser reflex occurs when the dowser passes through a region
where the Earth�s magnetic field is not entirely uniform. This field anomaly
produces a magnetic field gradient, which must exceed 0.1 mOe m 1 (8 mA m 2) to
be detected. The speed with which the dowser��
Fig. 1.12. Dowser holding a divining rod while searching for
underground water. (Illustration from Abbe� de Vallemont�s Treatise on the
divining rod, Paris, 1693).
passes through this field
gradient also influences their magnetic reception. The dowser must pass through
a 0.1 mOe m 1 field gradient within at least 1 s in order to detect it.
Furthermore, the detection level can be increased by adding up the small
differences in field gradients. Higher magnetic field gradients, however, lead
to saturation and can only be detected by moving faster. Of additional interest
is Rocard�s notion that although most people are sensitive, a good dowser has a
more accurate and rapid reflex than the bad dowser.
Physiological explanations of the
dowser reflex have included the physiological induction of magnetic moments,
electromagnetic currents, and nuclear magnetic resonance. None of these
possibilities has, however, been able to account convincingly for the
phenomenon, and thus the search for an explanation continues.
Electromagnetic machines produce fields and field gradients
which are constantly changing and which have been found to influence humans.
The earliest experiments to test the effects of these fields using humans were
performed at the end of the 19th century. D�Arsonval�s experiments were among
the most spectacular (Rowbottom and Susskind, 1984). In one of these experiments,
a person was completely enclosed in a large solenoid resembling a cage, and
insulated from all contact with it (Fig. 1.13). Owing to the high-frequency
oscillating magnetic field within the solenoid, strong currents were induced
within the subject�s body, and��
Fig. 1.13. D�Arsonval�s great solenoid or cage for
auto-conduction in which the person is insulated from all contact with current carrying
wire. The photograph shows the cage actually used by D�Arsonval in 1893 for his
experiments.
although neither pain nor any
other sensation was felt, a lamp held in the person�s hands became incandescent
during the procedure. D�Arsonval called this method of applying high-frequency
currents to man ��autoconduction��.
As the 20th century began, the serious
investigation of the physiologic consequences of electromagnetic fields became
tainted by association with quack science and the pseudo-technology of
electromedicine. Dr. Albert Adams (1863�1924), one of the controversial
therapists applying electromedicine, was named ��Dean of 20th century
charlatans�� by the American Medical Association. Adams postulated that each
organ system and each patient were tuned to a characteristic electromagnetic
wavelength. It should therefore have been possible to diagnose medical
conditions and to deliver therapy to individuals hundreds of miles away simply
by using a properly tuned, radio-based device. This therapy was called
��physiologic frequency manipulation��, and it aroused public interest in
bioelectricity and electromagnetic physiologic effects. The science community
gradually lost interest in bioelectricity, but before its fall from grace, the
groundwork was laid for such major clinical applications as electroconvulsive
therapy, cardioversion, and transcutaneous nerve stimulation.
Between 1930 and 1960, the
physiological and biological effects of electromagnetic fields were studied
only minimally. Research accomplished by the small group of investigators who
continued working in this area was reviewed comprehensively by Barnothy during
the late 1960s (Barnothy, 1964, 1969). Although the design of many of those
studies performed up to this time was flawed, some of their results have been
confirmed by more stringent research. For example, results recently endorsed in
a report by the National Research Council (1997) support previous findings that
electromagnetic fields induce changes in the brain�s electroencephalographic
(EEG) activity (Bell et al., 1991), produce measurable changes in polypeptide
synthesis in salivary glands (Goodman and Henderson, 1988), and are able to
influence the levels of calcium and melatonin in cells exposed to highlevel
fields (Graham et al., 1996). Additionally, recent double-blind studies have
confirmed the effects of low-frequency pulsed electromagnetic fields greater
than 0.5 mT on growth induction in bone. Indeed, their use is now the treatment
of choice for certain recalcitrant problems of the musculoskeletal system,
including salvage of surgically resistant nonunions in children and adults and
chronic refractory tendinitis (Bassett, 1989).
Available data indicate that
humans are susceptible to alternating electromagnetic fields. Epidemiological
studies even suggest health effects attributable to relatively small magnetic
fields such as those found underneath a high-voltage line (Jauchem, 1995). The
report of the National Research Council, for example, acknowledged a 1.5-fold
higher incidence of childhood leukemia in homes situated close to high-voltage
power lines, though the examined studies failed to show a statistically
significant association between exposures and disease (National Research
Council, 1997). Unless new theories for these effects are proposed on the
grounds of molecular mechanisms, it will be very difficult to either prove or
disprove any association between disease and the small magnetic fields produced
near electric devices, machines and power lines. Even the electromagnetic
fields in heavily industrialized regions amount only to a few tenths of one
mTesla, which is less than 1% of the ambient terrestrial magnetic field. Most
experts would not anticipate any serious effects related to these additional
magnetic fields.
Current laboratory investigations
employ more sophisticated techniques, more sensitive instruments and more
refined statistical methods than ever before. When combined with our deeper
understanding of magnetic resonance patterns in tissues (see Chapter 3), this
vastly improved instrumentation should provide a strong base from which to
improve our understanding of the electromagnetic field effects at the cellular
and molecular levels. In time, this will likely lead to the introduction of
new, magnetism-based medical techniques for diagnosis and therapy.
(back
to content)
4.11
A Brief History of Aromatherapy w
Available evidence suggests that
humankind recognised the power of aromatics as early as the Neolithic Period,
which ended some 4,000 years ago. Aromatic herbs may have been used in cooking
and medicine, as indicated by the discovery of medicinal plant deposits found
in graves dating from some eight thousand years ago.
Egyptian culture used resins,
balms and fragrant oils for medical, magical and religious ceremonies, for
embalming, and as an offering to their gods. Other ancient cultures recognised
the physical and psychological benefits of scented ointments and oils,
including China and India, during the same period as ancient Egypt. Greek and
Roman cultures refined and added to this knowledge. Hippocrates, known as the father
of modern medicine, maintained 2,500 years ago that �the key to good health
rests on having a daily aromatic bath and scented massage�.
Dioscorides wrote about aromatics in his Materia Medica
about 100 AD.
With the fall of the Roman Empire
and the expansion of Christianity, Roman physicians fled to Constantinople with
the books of Galen, Dioscorides and Hippocrates. These were translated into
Persian and Arabic and passed into the Arab world.
Most aromatic oils used (prior to
about 1600 AD) were not distilled, as we know today, but were produced by
macerating plants in hot vegetable oils or more commonly in animal fats.
However, distillation of some
sort is an age-old process, which may have begun as early as 2000 BC. This
suggests that the Arabs revived or improved upon the process that had been
known but perhaps little used for over four thousand years.
Between the 7th and the 13th
centuries Alchemist Arabic philosophers devoted themselves to the old hermetic
art of alchemy, the purification and concentration of spiritual forces.
Reviving the use of aromatics in
medicine and perfumery, they perfected the techniques. Alchemists
optimistically searching for the "elixir of life" and "the
philosophers' stone" made many chemical discoveries.
HISTORY
800-870 AD - Al-Kindi is known to
have written a volume called The Book on Chemistry of Perfumes and
Distillation. Avicenna, the Great Physician, lived between 980-1037 AD and has
been credited with the discovery of the refrigerated coil (a breakthrough in the
art of distillation) and wrote the Canon of Medicine, a standard text until the
mid-sixteenth century.
16th CENTURY - 16th Century - By
the 16th century the printing press made possible the spread of aromatic and
herbal knowledge, resulting in many herbal books; and "waters" and
"chymical oils" could be bought from the local Apothecaries' shops. A
German physician, Hieronymus Braunschweig, wrote several books on essential oil
distillation. In 1597 he referenced 25 essential oils included rosemary,
lavender, clove, cinnamon, myrrh and nutmeg.
17th &18th CENTURY - By the
beginning of the seventeenth century, with the isolation of Artemisia,
bergamot, cajeput, chervil, cypress, mustard, orange-flower, pine, savin, thuja
and valerian along with others, most of the useful essentials of Europe and the
Near East had been discovered. The 17 18th centuries saw the beginnings of the
common use of essential oils and aromatics for health. During the great plague
of Toulouse (1�628-1631), a formula was revealed by four thieves caught
red-handed, thus began the story of the origin of the "Four Thieves
Vinegar" which used herbs and spices in vinegar. The next few centuries
saw the medicinal properties and applications of essential oils analysed and
recorded. These included such oils as cedar, cinnamon, frankincense, juniper,
rose, rosemary, lavender, sage, Artemisia, cajeput, chervil, orange flower,
valerian and pine.
19th CENTURY - With the arrival
of technical chemistry and modern science in the 1800s the scientific revolution
of the early 19th century began and aromatics were investigated more
scientifically; and attempts were made to control the adulteration of essential
oils from the eighteenth century onwards. This science revolution had two
important effects on the study of essential oils. By 1887 we saw the first
recorded laboratory tests on the anti-bacterial properties of essential oils
thus spurring natural practitioners and herbalists to continue to use essential
oils widely in herbal preparations. But the mainstream medical profession
became firmly fixed on isolating the active principles of natural substances
and producing chemicals as drugs, which remains today.
As research on essential oils
continued, Drs. Gatti and Cajola, (Italy, 1923) published "The Action of Essences
on the Nervous System", explaining how odours influence mood and emotion
and defining two opposing states of anxiety and depression. They demonstrated
that, by reflex action, the sense of smell has influence on the function of the
central nervous system. Their work also included information on medicinal and
skin care properties. Paolo Rovesti (1973), Professor and Research Director of
the Instituto Derivati Vegetali, Milan University, Italy, showed antiseptic
properties and psychological properties (stimulant/ sedative). Citrus
(bergamot) was first clinically proven to be beneficial to anxiety and
depression.
PEOPLE IN HISTORY
1920's - RENE M. GATTEFOSSE
In 1928, the French perfumer and
cosmetic chemist Rene M. Gattefosse, was researching the cosmetic uses of
essential oils. He was badly burnt in an explosion and he began to use lavender
when the wound was not healing; he was surprised when the skin healed at a
phenomenal rate with no sign of infection or scar. He published his book
Aromatherapie showing the use of essential oils as antiseptic, antibacterial
skincare and coined the term "Aromatherapy". In an article, he said:
"The French cosmetic chemists are concerned that the natural complexes
should be utilized as complete building units in the instance without being
broken up. Dermatological therapy would, thus, develop into "Aromatherapy�
or a therapy employing aromatics in a sphere of research opening enormous
vistas to those who have started exploring it". (i)
1940's - 1970's - JEAN VALNET
Jean Valnet, a French doctor and
researcher/scientist, had a background in using herbs therapeutically and began
using essential oils for treating patients during his time in French colonial
Vietnam. He realised the potential of essential oils as part of treatment for
specific medical and psychiatric disorders and by 1954, had established doses;
the results were published in the book Practice of Aromatherapy (1964). This
became our first materia aromatica of recent times and was a consolidation and
expansion of the therapeutic applications of essential oils. He not only
integrated essential oils as treatment into herbal medicine again, but also
brought essential oils full circle back to the way they were originally used
during the Renaissance. Considered the father of modern essential oil medicine,
his students include Belaiche, Lapraz, Duraffourd, Penoel, and Mailhebiau. They
have continued to develop his approach from the 1960s to the present day.
MARGUERITE MAURY
Marguerite Maury, a nurse,
surgical assistant with an interest in biochemistry, explored the therapeutic
use of oils in the 1940s and wrote The Secret of Life and Youth. She combined
essential oils and massage producing a medico cosmetic therapy based on
massage. She conceived the notion for the "individual prescription"
(or IP), which is a blend to operate on physical/ psychological/ spiritual
levels, to normalise the unbalanced functions of the whole person. In
describing the effect of essential oils on the psyche, she said: "But of
the greatest interest is the effect of fragrance on the psychic and mental
state of the individual. Powers of perception become clearer and more acute and
there is a feeling of having, to a certain extent, outstripped events. They are
seen more objectively and therefore in truer perspective." (ii)
Maury is responsible for the type
of non-medical aromatherapy that developed in England in the 1950s. Madeline
Arcier carried on Maury's work, operating a clinic and school in London.
Danielle Ryman, a student, is responsible for the reprinting of Maury's book.
Robert Tisserand, a massage therapist from the UK, influenced by both Valnet
and Maury wrote the very first aromatherapy book in English in 1977 entitled,
'The Art of Aromatherapy'. This book became the inspiration and reference for
virtually every future author on the subject for almost two decades. This
holistic approach is the foundation of what is globally generally called
�aromatherapy�.
�
AROMATHERAPY TODAY
United States
Today aromatherapy as a modality
is practiced by licensed body workers, massage and beauty therapists, and other
holistic practitioners. Essential oils are also combined with massage,
skincare, physical therapy, chiropractic, acupuncture, yoga, and other
complementary therapies. Few medical doctors offer aromatic medicine at this
time, but capsules for IBS and relaxation are available with a prescription.
More hospitals are including essential oil training in wellness staff
education.
Since there is no certification
available nationally, independent schools have developed their own programmes
and titles for graduates such as Certified, Clinical, etc. but there remains no
standard and programmes range from a one-hour online to live year-long
programmes of 425 hours. Practitioners are trained online or in live classes in
everything from a one hour hand massage to full 425 hour programme including
aromatic medicine treating serious illness. Several attempts have been made to
organise therapists resulting in two active organisations, namely the National
Association of Holistic Aromatherapists and the Alliance International
Aromatherapy. At this time the Aromatherapy Registry Council is the only
national testing body that can give the title Registered Aromatherapist or R.A.
Europe
France has an abundance of holistic
practitioners who use or research essential oils such as Prof. Pradal, Dr.
Girault, and Dr. Belaiche, in the medical circles and Dr. Lamblin, Prof.
Raymond Lautie, D. Sc., Andre Passebecq, M.D., D.Ps., and Pierre Franchomme in
the naturopathic movement. Dr. Jean- Claude LaPraz is a medical doctor
responsible for developing phytotherapy training of doctors and pharmacists in
Lille, Montpelier, Athens and Monastir (Tunisia), and created a National
Diploma in Clinical Phytotherapy. Dr. Christian Duraffourd also lives in France
and teaches phyto-aromatherapy to medical professionals. Many naturalistic
doctors use and prescribe essential oils within their practice, along with
other natural medicines, but aromatherapy is not used in the mainstream medical
arena. Additionally, there are aromatherapists practicing (although slightly
illegally) through, say a chiropractor's office, or under some other licensed
professional.
The rapid growth of the number of
companies offering essential oils, especially the massive multi level market
companies, has created a massive growth in the last ten years. They have also
contributed to a large overuse problem so that some oils become scarce. And
because many give no safe use advice, and promote unsafe uses (e.g. undiluted on
skin, oral use in water,) that we now have a rise in adverse effects occurring.
Time will tell how this all plays out.
(back
to content)
4.12 The History of Massage Therapy s: 5,000 Years
of Relaxation and Pain Relief
THE ORIGIN OF MASSAGE THERAPY AND ANCIENT METHODS
The history of massage therapy
dates back to 3000 BCE (or earlier) in India, where it was considered a sacred
system of natural healing. Used by Hindus in Ayurveda �life health� medicine,
massage therapy was a practice passed down through generations to heal
injuries, relieve pain, and prevent and cure illnesses. Promoters of Ayurveda
believe that illness and disease are caused when people are out of sync with
the environment. Massage is believed to restore the body�s natural and physical
balance so that it can heal naturally.
As culture and history evolved,
the healing methods of massage traveled to China and Southeast Asia about 2700
BCE. Chinese massage methods developed as a combination of skills and practices
of traditional Chinese medicine, martial arts and the spiritual yoga training
of Buddhists and Taoists. Their methods were very similar to those of the
Indians, based on the belief that disease was caused by an imbalance or
deficiency of energy of various pathways. The ancient Chinese developed a text
called The Yellow Emperor�s Classic Book of Internal Medicine that is today
considered a staple of massage therapy alternative medicine (acupuncture,
acupressure and herbal remedies).
By 2500 BCE, massage therapy had
made its way to Egypt, where it was depicted in tomb paintings. The Egyptians
added their own bodywork techniques and are credited with developing
reflexology, which involves applying pressure to specific points or zones on
the feet and hands to effect healing.
Later, monks studying Buddhism in
China brought massage therapy to Japan in 1000 BCE and put their own twist on
it, calling it �anma,� later known as Shiatsu. This technique is designed to
regulate and strengthen organs by rebalancing energy levels through the
stimulation of pressure points in hopes of bringing natural resistance to
illness.
MASSAGE THERAPY IN ANCIENT GREECE AND THE ROMAN EMPIRE
The Egyptians influenced the
Greeks and Romans who used massage therapy in different ways. In Greece,
between 800 and 700 BCE, athletes used massage to condition their bodies before
competitions, and doctors often applied herbs and oils in combination with
massage to treat various medical conditions. Hippocrates, the �father of
medicine,� treated physical injuries in the 5 Century BCE with friction, a
massage technique, and was the first to prescribe a combination of massage,
proper diet, exercise, fresh air and music to restore health imbalance � a
remedy we hear of even today.
Roman physician Galen, in the 1
Century BCE, used massage therapy on emperors, echoing Hippocrates� ideas of
treating injuries and illnesses. The wealthy Romans would have massages in
their homes, but the general public would flock to the Roman baths for �spa�
treatments and full-body massages, to stimulate circulation and loosen their
joints.
The popularity of massage therapy
declined in the West until the 17 Century, when new discoveries in pharmacology
and medical technology changed modern medicine. However, many doctors could see
the health benefits of massage.
A Swedish doctor brought massage
therapy out of retirement. In the early 1800s, Swedish doctor/gymnast/teacher
Per Henrik Ling created a method that became known as the Swedish Movement Cure
to help relieve chronic pain. As much medical gymnastics as massage therapy, it
was the precursor to what we now know as Swedish massage � a style that
involves stroking, pressing, squeezing and striking.
Whereas Ling�s method used massage in his movements, 19
�Century Dutchman Johan George Mezger is credited with incorporating techniques
that are used today:
Effleurage, which uses long, gliding strokes from the
extremities inward at various levels of pressure
Petrissage, a technique that is
rhythmic and may include kneading, skin rolling, lifting or a push-pull
movement Tapemotement, a beating/tapping administered with the side of the
hand, a cupped hand or fingertips used in Swedish massage Friction, a technique
that is physically demanding, consisting of deep, circular or crosswise
movements with the thumbs, fingertips, palms or elbows, designed to penetrate
deep tissue America jumps on the massage therapy bandwagon
As early as the 1700s, �rubbers�
(women hired by surgeons to treat orthopedic problems with manual rubbing and
friction) were the massage practitioners of the day. By the 1850s, however,
�medical gymnasts� used movement and manipulation, as developed by Ling, to do
the same thing.
Their comprehensive training included anatomy, physiology,
hygiene, pathology and movement perceptions that they practiced in hospitals
and clinics.
By the late 1800s, the names �masseur� and �masseuse� became
popular.
These practitioners were trained in soft tissue manipulation
� la Mezger.
Hydrotherapy was used in conjunction with massage at this
time and could be considered the origin of today�s spa services, like body
wraps and scrubs.
Curiously, the full-body massage
became part of the �rest cure� for the melancholy known as neurasthenia that
was popular among society ladies who lived the wealthy life of the late 1800s.
Massage therapy in the 20 and 21 Centuries
The demand for masseurs and
masseuses increased in the early 1900s. By the 1930s, Swedish massage had
evolved, and the physiotherapists who used it in regular medicine helped
massage therapy to become a legitimate and respectable form of medicine.
Once physical therapy was
licensed in the 1950s, massage therapy had its own category. The American
Massage Therapy Association (AMTA) was established and laid the groundwork for
today�s massage practitioners by establishing ethics and education standards.
Between 1970 and 2000, massage
therapy experienced a transformation, as people chose to live healthier
lifestyles and preferred more holistic approaches to health care, pain
management and restoring and maintaining healthy bodies. Today, many realize
that �massage is good medicine.�
(back
to content)
4.13 A brief history of spa therapy r
A van Tubergen, S van der Linden 2001
Bathing in thermal water has an
impressive history and continuing popularity. In this paper a brief overview of
the use of water in medicine over the centuries is given.
NOMENCLATURE
The word �spa� may be derived
from the Walloon word �espa� meaning fountain. This, in turn, came from the
name of the Belgian town Spa, where in the 14th century a curative, thermal
spring was discovered. Spa may also originate from the Latin word �spagere� (to
scatter, sprinkle, moisten) or may be an acronym of the Latin phrase �sanitas
per aquas� (health through water). In Britain, the word spa is still used, whereas
in the rest of Europe the term �thermal waters� is preferred. Bathing in
thermal water for therapeutic purposes has several descriptions (for example,
taking the waters, balneotherapy, spa therapy, hydrotherapy), which will all be
used throughout this paper, and are more or less interchangeable.
ANCIENT GREECE AND THE ROMAN EMPIRE
Taking the waters used to be a
popular treatment for a wide range of diseases in classical times. The Greeks
preferred baths in fresh water from natural resources, although bathing in the
sea (thalassotherapy) was also applied. Initially, bathing was confined to the
more wealthy people in private baths, but soon public baths were opened. The
baths were considered sacred places and were dedicated to several deities.
In Homeric times, bathing was
primarily used for cleansing and hygienic purposes. By the time of Hippocrates
(460�370BC), bathing was considered more than a simple hygienic measure; it was
healthy and beneficial for most diseases. Hippocrates proposed the hypothesis
that the cause of all diseases lay in an imbalance of the bodily fluids. To
regain the balance a change of habits and environment was advised, which
included bathing, perspiration, walking, and massages.
The baths were often combined with sports and education, the
precursors of the gymnasium.
Influenced by the Greeks, the
Romans built their own thermal baths at mineral and thermal springs. A military
presence was often the key to development of such a spa resort. Spas served not
only for recuperation of wounded soldiers but also as rest and recreation
centres for healthy soldiers. In contrast with the Greeks, who took the waters
after intensive physical exercises, the Romans considered the baths more important
than the gymnastics alone.
Besides cleansing, exercises,
socialising, relaxation, and worship, medical treatment was also applied
extensively. Spa treatment consisted of application of water to afflicted parts
of the body, immersion of the whole body in the water (especially for rheumatic
and urogenital diseases), and drinking excessive quantities of water.
Asclepiades (c 124 BC), a Greek physician who practised in
Rome, introduced general hydrotherapy and drinking cures as treatments.
He recommended bathing for both
therapeutic and preventative purposes. Pliny the Elder (AD 23�79) assigned
different properties and indications for cure to different types of waters.
Galen (AD 131�201) also advocated the use of water for the treatment of a
variety of diseases.
He preferred cold water, a concept that was reconsidered
periodically throughout the following ages.
In Rome three different types of baths developed: baths at
home (balnea), private baths (balnea rivata), and public baths (balnea publica)
that were run by the state.
With the introduction of
aqueducts, the public baths later developed into huge and impressive edifices
(thermae) with a capacity for thousands of people. During the heyday of the
Roman bathing culture, the inhabitants of Rome used 1400 litres of water per
person per day, mainly for bathing.
The Roman legions, far away from their homeland, built their
own baths at mineral and thermal springs in the newly conquered lands.
Examples are found all over Europe.
Throughout the years the Roman bathing culture gradually
changed towards a place for relaxation and pleasure, rather than for medical
treatment, although this was still provided.
The Romans preferred to use the baths and very hot waters
for renewing their appetites and thirst, and the baths became, rather, centres for
various sexual practices.
Deterioration of morals became manifest, the hygienic and
medical indications for bathing disappeared, and baths as a haunt for pleasure
ruled.
THE DARK AND MIDDLE AGES
With the fall of the Roman Empire
in 476 and the rise of Christianity, the bathing culture fell into disrepute
and bathing was officially prohibited. Faith in cure through worship and
praying was regarded as more important than a medicinal bath.
Baths were redeveloped as churches, although some remained
available for the aristocrats who were not affected by the church�s decrees.
The aversion to bathing remained
for many centuries. People abstained from bathing as long as possible,
sometimes for years.
�People abstained from bathing, sometimes for years�
From the 13th century onwards,
baths gradually came into re-use, particularly in southern Europe under the
influence of the Moors. Public baths were rebuilt and the entrance was usually
free. The baths were often crowded and people bathed for hours, sometimes days
in the same bath. Blood letting, enemas, and drinking cures (up to 10 litres a
day) were prescribed, although relaxation and pleasure were most often the
reasons for bathing.
RENAISSANCE
In the 16th century the image of
the public baths again deteriorated in many countries, which led to the closure
of many public baths. They were considered to be a source of contagious diseases
such as syphilis, plague, and leprosy, and the baths became dangerous meeting
places for political and religious dissidents.
In addition, owing to a shortage of firewood, public baths
became more expensive for a population that had already become impoverished by
many wars.
Nevertheless, the gentry
continued to visit the baths, although they preferred to go to baths from
natural sources with warm, mineral water instead of the public baths.
Taking the waters was now no
longer a spontaneous activity, but it was increasingly prescribed under medical
direction.
Several famous Italian doctors
recovered lost texts on medical treatment from the ancient world, and the value
of balneology as a therapeutic modality was reconsidered.
By this time, the first attempts
to analyse the waters for their mineral components were made, although the results
were often controversial.
It was equally important to
recognise the quality of each mineral and its effect on the body, as to know
which parts of the body might be influenced by taking the waters.8 In 1553 an
encyclopaedic work, De balneis omniae qua extant, was published, containing an
overview of ancient and modern literature on the use of medicinal water. In
1571, Bacci published De thermis, in which he taught the art of the baths from
Galen and the Aristotelians. According to Bacci, taking the waters was not a
matter of empiricism, but a sound discipline with its own rationale,
institutes, and doctrine, which the learned physician alone was qualified to
understand.
Minardo published in 1594 a
compendium on the two baths of Caldiero in Verona. The first bath was used for
drinking and bathing, the second was used by bathers with skin conditions, for
bathing of animals, and for washing off therapeutic mud.
Seventy-eight conditions that
might benefit from these baths were listed. The treatments consisted of
drinking cures, bathing, purging, and application of mud. It was advised to
follow this type of treatment for 15 days, and repeat it every year.
According to Bacci, essential to
the cure was a quiet orderly life in pleasant surroundings with good food and
wine, and a maximum of comfort.8 Therefore, he argued, the baths would do no
good to the poor. Other, practical obstacles also restrained the poor from
attending the baths: they had no time for leisure and the baths and mud were
usually not free.
The new bathing culture that had
developed in Italy gradually spread over other parts of Europe, and was
particularly popular with the elite. The development of spa treatment north of
the Alps was mainly provided by the Paracelsians.
By the turn of the 17th century, many spas were rediscovered
in France. Two types of spas existed: hot springs for drinking and bathing, and
cold springs for drinking cures only.
Taking the waters in French spas was a serious activity and
quite sober.
Doctors created centres for
treatment, not for leisure. Much attention was paid to purging, drinking cures,
eating well balanced diets, and bathing. In the afternoons some indoor leisure
activities were provided. Late in the afternoon, people walked about on the
promenade, and went to bed early in the evening.
This was in contrast with many other European countries, where
in the evenings diverse leisure activities were offered such as theatre and dance.
19TH AND 20TH CENTURIES
Around 1800 interest in the
bathing culture grew. Further attempts to analyse the mineral water were made,
aiming at improving its use in medicine, and at preparing mixtures of water
identical to those mineral waters famous for their curative properties.
Doctors were convinced that for
each disease Mother Nature possessed an appropriate medicinal spring, which
could be discovered through chemical analysis of the waters.
Priessnitz and Kneipp further
developed the principles of balneotherapy (medicinal use of thermal water) and
hydrotherapy (immersion of the body in thermal water for therapeutic purposes).
Individual treatments were
prescribed, based on the composition and temperature of the water. Also,
combinations of treatments were developed consisting of hot and cold baths,
herbal baths, mud packs, active physical exercises, massages, and diets. Kneipp
advocated a holistic approach to the treatment of a disease. In contrast with
the spa resorts, which aimed at the elite, Kneipp directed his attentions to
the common man.
The use of mineral waters and the development of hotels and
guesthouses at the springs became prevalent throughout Europe and North
America.
Every spa resort had its own theatre, casino, and promenades
besides the bathing buildings.
In Britain, Germany, Austria, and
Belgium much importance was attached to ostentation. Grand hotels arose with
casinos and dancing establishments surrounding the spa resorts. The spa resorts
became not only a meeting centre for the elite but also a place of creativity
for painters, writers, and composers.
The baths were again crowded.
Baden Baden (Germany) became the most glamorous resort in continental Europe.
It was the place to see and to be seen.
�The medical significance of bathing is acknowledged by many
rheumatologists�
However, in Britain use of the
spa declined. The English spa resorts were run by amateurs, and the medical
hydrology was poorly organised.
The resorts aimed more at
pleasure, rather than medical treatment, and were exploited by estate developers
with commercial interests.
Competition from seaside and
foreign resorts, and an economic depression in the 1930s led to a further
decline. Eventually, spa therapy was excluded from the National Health Service,
which meant that many spa resorts in Britain closed down.
After the second world war and
with the rise in welfare, spa treatment became available for the common man in
many European countries, mainly owing to reimbursement by state medical systems.
Other activities and new
treatments were introduced, and balneology, hydrotherapy, and physiotherapy
underwent major developments.
In the past decades, a large
change in the use of mineral water for the treatment of several diseases has
taken place in continental Europe.
The medical significance of
bathing is now acknowledged, especially by many rheumatologists and
dermatologists, and this aspect is considered more important for a number of
spa resorts than prestige and leisure. Bathing is usually combined with many other
treatments, such as physical exercises, hydrotherapy, and mud packs. The spa
resorts are differentiated according to their location (for example, seaside,
mountain area) and the chemical composition of their mineral water (for
example, sulphurous, bicarbonated, or sulphated).
Each spring has its own characteristics and related
therapeutic properties.
However, a substantial number of
spa resorts also direct more attention towards leisure. Steam baths, saunas,
whirlpools, and solariums are standard equipment of many such spa resorts, with
the main objective being to relax and strengthen the body and mind, and to
prevent development of disease. In Britain, a revival of the spa culture may be
expected, with the re-opening of the hot springs in Bath in 2002. This spa will
offer facilities for medical treatment, but, in addition cater for a growing
number of so-called health tourists, who combine their holidays with an
investment in wellbeing.
SCIENTIFIC EVIDENCE FOR THE EFFICACY OF SPA THERAPY
Despite the popularity of spa
therapy, reported scientific evidence for its efficacy is sparse. A decade ago,
Heywood reviewed well documented records on spa treatment for lead poisoning in
the 18th and 19th century in Bath.
Paralysis occurring as a result
of chronic lead intoxication (colica pictonum) was a common problem in those
days owing to the widespread use of lead in household ware, cosmetics, food
colorants, wine, and salts for medicinal use. Already at the beginning of the
16th century, Bath was famous for curing paralysis, even in those patients who
were regarded as incurable.
The treatment consisted of
bathing, drinking cures, diet, and purges. Patients admitted to the Bath
Hospital came from all over England, and often had already been treated for
their paralysis elsewhere, without success. However, many of these presumed
incurable patients were cured after their (months) stay in Bath.
An example can be found in the comparison of medical records
of Bath and Exeter Hospitals between 1762 and 1767.
During these five years, 285 patients with colica pictonum
were admitted in Exeter and 281 patients in Bath.
Seventy-three per cent of the
patients from Exeter were cured or improved, whereas the figure was 93% from
Bath. Moreover, the group in Bath included some 80 patients referred from
Exeter who had not been cured by treatment in Exeter.
From 1760 to 1879, 3377 patients were admitted in Bath for
paralysis due to lead intoxication. Forty-five per cent were cured and 93% had
at least improved.
The high cure rates for paralysis
by spa therapy in Bath may be attributed to several factors. Sitting in warm
water produces diuresis, with increased excretion of sodium, potassium,
calcium, and also lead. Also the good food, exercises, removal from the source
of lead, and the large quantities of water rich in calcium and iron contributed
to the success of spa therapy in Bath.
In the past decade several
randomised controlled trials have studied the effects of spa therapy in
rheumatoid arthritis and osteoarthritis. Patients were randomly allocated to
receive spa therapy or sham/no therapy. The authors of a recent systematic
review on the effects of spa therapy in rheumatoid arthritis and osteoarthritis
stated that a definite judgment about its efficacy is impossible because of
methodological flaws in these studies. Overall, the results showed positive
effects lasting for three to nine months. Recently, a randomised controlled
trial has shown that spa therapy is clearly effective in ankylosing
spondylitis.
Two intervention groups followed
a three week course of spa therapy at two different spa resorts, and were
compared with a control group who stayed at home and continued standard
treatment consisting of anti-inflammatory drugs and weekly group physical
therapy. Significant improvements in function, pain, global wellbeing, and
morning stiffness were found for both intervention groups until nine months
after spa therapy.
CONCLUSION
Throughout the ages the interest
in the use of water in medicine has fluctuated from century to century and from
nation to nation. The (medical) world has viewed it with different opinions,
from very enthusiastic to extremely critical, and from beneficial to harmful.
Today, spa therapy is receiving renewed attention from many medical specialties
and health tourists, and having a revival. However, the exact therapeutic
potential of spa therapy still remains largely unknown. Better and more
profound scientific evidence for its efficacy is therefore warranted, in
particular for its effects on the musculoskeletal system.
(back
to content)
4.14 A History of Kinesiology q
Jaime Schultz
LEARNING OBJECTIVES
1. Understand the importance of context in understanding
historical change.
2. Describe the difference between physical education as a
profession and physical education as a discipline.
3. Explain why departments of physical education became
departments of kinesiology.
4. Recognize the importance of integrating kinesiology�s
subdisciplines.
INTRODUCTION
What we call ourselves matters.
The discipline we know today as kinesiology has gone through several different
names, and with each change came debate, contention, and a particular emphasis
that gives the field its current meaning. We are now well into the second
century of kinesiology�s many evolutions, and a brief historical analysis is
important to understanding where we came from, who we were, who we are, and
where we might be going.
To appreciate the history of
kinesiology requires recognizing its key precursor�physical education. In this
case, physical education does not refer to the classes you took in elementary
or high school, or even the skill or lifestyle classes you may take in college.
Instead, it represents academic departments of physical education in higher education,
many of which are now called departments of kinesiology. These are units
dedicated to creating and sharing knowledge about physical activity and human
movement, and as you will find in this chapter, these departments now include a
variety of subdisciplines�specialized domains of study within the broader
subject.
The Embryonic Period: 1880s�1900s
Sport studies scholar Joan Paul
(1996) classifies the era between 1880 and 1900 as the embryonic period for
physical education. In other words, the field was in the very beginning stages
of development. During this time, advocates recognized the value of activities
such as gymnastics (which then referred to a series of precise and regimented
exercises), calisthenics, physical culture, and physical training to encourage
health and physical fitness.
However, physical education did
not have a central mission, and multiple, competing philosophies and exercise
systems created a lack of organization and coherence.
What encouraged the need for
formalized physical education? Historical understanding requires situating the
phenomenon in question within its historical context. It is important to ask
what the larger social, cultural, political, and economic issues were at the
time, how those issues affected physical education and, in turn, how physical
education influenced those historical circumstances. For example, the
modernization and industrialization of society in the 19th century reduced the
amount of physical activity required in the average American�s day. Activists
therefore worried about the lack of �vigor� in people�s lives, and promoted
exercise as the antidote to a �soft� life. At the same time, lingering concerns
about military preparedness resulted in the establishment of physical training
programs. And with the large increase in immigration during this time,
reformers turned to sport and physical activity to address their anxieties
about health, assimilation, and Americanization. Thus, physical education
developed within the context of great historical change and was designed to
meet numerous social needs.
In the 1880s and 1890s, most
programs aimed at training physical educators were located in private normal
(or teachers�) colleges. Instructors of these programs were often physicians,
illustrating the close ties between the field and medicine and the biological
sciences. Accordingly, the curriculum included aspects of anatomy and
physiology, physics, and anthropometry (the scientific study of the
measurements and proportions of the human body), as well as educational theory.
Physicians made up the majority
of the first members of the Association for the Advancement of Physical
Education, established in 1885 as a way to begin to institutionalize and
legitimize the area of study. The following year, the organization (which had
changed its name to the American Association for the Advancement of Physical
Education, or AAAPE; see Table 3-1 for a series of name changes that offer
historical insight) published the American Physical Education Review (now the
Research Quarterly for Exercise and Sport), a journal that disseminated and
encouraged professional knowledge.
At the 1890 AAAPE conference, physician Luther Halsey Gulick
declared physical education a �new profession� that involved �a profound
knowledge
Table 3-1 The Evolution of SHAPE America
1885 Association for the Advancement of Physical Education
1886 American Association for the Advancement of Physical
Education
1903 American Physical Education Association
1937 American Association for Health and Physical Education
1938 American Association for Health and Physical Education
and Recreation
1974 American Alliance for Health, Physical Education and
Recreation
1979 American Alliance for Health, Physical Education,
Recreation and Dance
2013 Society of Health and Physical Educators (SHAPE)
America
of man [sic] through physiology,
anatomy, psychology, history and philosophy�. Although many think that the
subdisciplinary movement of kinesiology is something that originated in the
mid-20th century, it is clear that it has deeper roots (Park, 1989).
The Profession of Physical Education: 1900�1960
In the early 1900s, physical
education also included elements of nutrition and hygiene, which originally
signified elements of exercise, but later aligned more with what we think of
today as health education. Before long, however, physical educators began to
emphasize the value of play, games, and sport, leaving behind the gymnastic
tradition. This happened in both men�s and women�s programs, which were almost
always separate from one another.
Men�s intercollegiate sport grew
evermore popular during this time, and physical education programs extended
their training to the preparation of coaches. After a brief period of
intercollegiate sport for women, the majority of women physical educators
advocated intramural and interclass athletics and, more often, dance,
instruction in posture, hygiene, and �play days.� These activities were
supposed to promote cooperation, instead of the type of competition that would
damage participants� bodies and minds.
The �play attitude� promoted the
�ideal of universal opportunity for participation in athletic activities�
(Sefton, 1941). In this way, physical educators kept tight control over the
development of women�s sport, a situation that lasted throughout much of the
20th century.
Initially, many programs, for
both men and women, operated under the name �physical culture,� but in the late
1920s and early 1930s, the term physical education became the dominant title
for the field. Most faculty �did not carry active programs of research in any
area of specialization,� but instead focused on teaching and advising their
students (Massengale & Swanson). Education �was dedicated to acquiring
motor skills and methods of teaching these skills, planning curriculum, and the
organization and administration of programs in athletics, health, and
recreation as well as physical education� (Corbin, 1993).
Times of war offer occasions to
assess the physical fitness of the nation and often highlight the importance of
physical education. This happened during World War I, when military officials
rejected an alarming number of young men drafted into service due to �lack of
fitness.� As a result, many states enacted mandatory physical education
instruction in public schools, which, in turn, created a need for trained and
qualified teachers.
It happened again during World
War II, when physical assessments deemed many potential draftees unfit to
serve. Events in the postwar era also pointed to the need to bolster national
health. The 1953 Kraus-Weber tests demonstrated that American youth were less
fit than their European counterparts. President Dwight D. Eisenhower suffered a
heart attack, which directed greater attention to the benefits of exercise for
both health and rehabilitation. For these and other reasons, in 1956 President
Eisenhower initiated the President�s Council on Youth Fitness (now the
President�s Council on Physical Fitness, Sports, and Nutrition�once again, what
we call ourselves matters). This high-profile, government-sanctioned program
boosted the profession of physical education.
The end of World War II marked
the beginning of Cold War hostilities between the United States and the Soviet
Union. In the absence of �hot war� (or actual fighting), political and
ideological tensions spilled over into symbolic arenas in which the two sides
could compete for dominance.
Sport was one such arena. In
fact, the Cold War helped convince women physical educators and others to
revise their views on women�s sport and begin to promote elite-level training
and competition. During this same time, administrators of high-profile men�s
athletic programs began to move into separate units and away from their
historical homes within physical education. As coaches left physical education,
it became possible for administrators to hire faculty dedicated to teaching and
research.
Like sport, scientific innovation
provided another place where Cold War opponents could compete. In 1957, the
Soviets successfully launched Sputnik 1, the first artificial satellite,
sparking a great deal of concern about the status of science education in the
United States. This affected physical education and incited calls to
�scientize� the field.
Physical educators added their voices to these calls.
Some of this impulse came on the
heels of James Conant�s 1963 book, The Education of American Teachers. Conant,
the former president of Harvard University, was critical, writing, �I am far
from impressed by what I have heard and read about graduate work in the field
of physical educations � To my mind, a university should cancel graduate
programs in this area�. As you might imagine, this alarmed physical educators,
who already felt as though their work did not receive academic respect (see
Twietmeyer, 2012).
The year after Conant published
The Education of American Teachers, Franklin Henry, a professor at the
University of California at Berkeley, pushed the idea that physical education should
be an academic discipline, or a branch of knowledge designed to produce and
disseminate expert knowledge, as opposed to a program that trained future
physical educators and coaches for a profession. Henry (1964) claimed �that the
proper academic study for physical education would only come by grounding the
discipline in theory.� He continued:
An academic discipline is an
organized body of knowledge collectively embraced in a formal course of
learning. The acquisition of such knowledge is assumed to be an adequate and
worthy objective as such, without any demonstration or requirement of practical
application. The content is theoretical and scholarly as distinguished from
technical and professional.
Henry defined the �scholarly
field� of physical education as one that includes �anatomy, physics and
physiology, cultural anthropology, history and sociology, as well as
psychology�. No matter the students� career goals, he argued, they should be
educated in these areas that would provide a broad-based understanding of human
physical activity.
The academic Discipline of Physical Education:
1960�1980
In the early 1960s, prodded by
the words of Conant and Henry, members of the American Academy of Physical
Education sought to determine what should constitute the discipline�s �body of
knowledge.� The subsequent Big Ten Body-of-Knowledge Symposium identified six
areas of specialization: (1) administrative theory in athletics and physical
education, (2) biomechanics, (3) exercise physiology, (4) history and
philosophy of physical education, (5) motor learning/sport psychology, and (6) sociology
and sport education. These subdomains, along with several others, are currently
recognized within kinesiology.
Consequently, the 1960s and the
1970s fostered specialization within physical education (Table 3-2). Members of
the various subgroups formed their own organizations, journals, texts, and
specialized courses within the major. With this trend came greater respect for
the field and the production of new knowledge, but �disciplinization� also had
some negative consequences.
First, the move devalued the
importance of physical education as it pertained to the preparation of teachers
and coaches�suggesting that practitioners of physical education were somehow
worth less than those who researched it.
Second, disciplinary
specialization brought fragmentation, such that the subdomains too often acted
independently, rather than in concert. Instead of integrating their knowledge
for a more holistic understanding of human movement, scholars became isolated
from one another. This lack of integration
and unification troubled physical
educators, who worried that students would fail to appreciate and, more
important, assimilate the depth and�
Table 3-2 The Evolution of Subdisciplinary Organizations
1953 American College of Sport Medicine
1967 International Society of Biomechanics in Sports
1968 North American Society for the Psychology of Sport and
Physical Activity
1972 North American Society for Sport History
1972 Philosophic Society for the Study of Sport
1973 International Society of Biomechanics
1974 The Association for the Study of Play
1978 North American Society for the Sociology of Sport
1983 Sport Literature Association
1985 North American Society for Sport Management
1985 Association for the Advancement of Applied Sport
Psychology
breadth of information in their
respective programs. They also worried that researchers in the subdisciplines
could just as easily belong in departments of physiology, physics, biology,
history, sociology, philosophy, and psychology as they could in physical
education, which might, in turn, render departments of physical education
obsolete in the eyes of campus administrators.
The number of programs dedicated
to teacher training, often called pedagogy, started to decline. Some
departments even eliminated the programs altogether. In time, �physical
education� no longer seemed an appropriate title for the discipline. One by
one, different units began to change their names, becoming departments of
exercise science, sport science, sport studies, human movement, human kinetics,
and kinesiology, to name a few.
In the 1980s, colleges and
universities used as many as 100 different names for the area of study once
known as physical education (Corbin, 1993, p. 85). By 1990, wrote Karl Newell,
it was not �an overstatement to suggest that physical education in higher
education is in a state of chaos� (1990a, p. 228). One way to remedy this,
Newell (1989) argued, was to bring everyone together under the umbrella of
kinesiology. He offered the following rationale for this name:
� It was representative of the entire field.
� It sounded academic.
� It was succinct.
� It was neutral with respect to the major subdomain debates
on each dimension.
� It was already established as the departmental title in a
number of leading academic institutions.
Not everyone has agreed with the wholesale change to
kinesiology, and several departments have resisted the trend.
As we consider the
subdisciplinary movement, it is important to understand that kinesiology not
only has a history�it also includes history. Sport history is an important
subdiscipline that emerged in the late 1960s and early 1970s. Sport historians
consider a range of fascinating topics, including organized athletics, physical
education, physical culture, active leisure, dance, recreation, and other
physical practices. Historians look at these topics as they relate to
technology, media, education, religion, the military, race, ethnicity, class, sex,
gender, sexuality, disability, popular culture, politics, the environment,
public policy, geography, and ideas about the body. In the United States and
Canada, the North American Society for Sport History has been the most
important organization for work in this area, although sport historians are
often involved with other organizations in kinesiology, sport studies, history,
American studies, women�s and gender studies, and popular culture.
Kinesiology as a Unifying Title:
1990�Present
The word kinesiology can be
broken down into the Greek words kinesis, which means �movement,� and ology, or
�the study of.� Newell was certainly not the first to suggest the word. Within
physical education, it has been used since at least 1886 (Paul, 1996). However,
the 1990s brought a concerted quest for a common professional identity and,
according to Newell (1990b), �kinesiology provides the best option in promoting
a broad-based disciplinary, professional, and performance approach to the study
of physical activity�. Debates about the title and focus of kinesiology
continue to rage. Some critics contend that the word is too esoteric for the
general population. Others find the term�s focus too narrow, aligned more with
structural�functional research, particularly biomechanics, and divorced from
practical application. Still others contend that guiding concepts, such as
�movement� and �physical activity,� are too broad and will lead (indeed, have
led) to topics of study that deviate far afield from the field�s roots in physical
education. We continue to question what areas should constitute our collective
body of knowledge.
Table 3-3 The Evolution of the National Academy of
Kinesiology
1904 Academy of Physical Education
1926 American Academy of Physical Education
1993 American Academy of Kinesiology and Physical Education
2010 National Academy of Kinesiology
However, kinesiology is
frequently, though not entirely, the overriding title for the many things we
do, study, and promote. If you take a look at Table 3-3, for example, you can
see that what was once the American Academy of Physical Education gradually
added �kinesiology� to its title and eventually dropped the phrase �physical
education� altogether to become the National Academy of Kinesiology (NAK). The
organization�s dual purpose is to encourage and promote the study and
educational applications of the art and science of human movement and physical
activity and to honor by election to its membership persons who have directly
or indirectly contributed significantly to the study of and/or application of
the art and science of human movement and physical activity (NAK, 2016).
Embedded in this description is an appreciation of the field
as both a profession and a discipline.
It bears mention that the need
for unity also extends to work done within departments of kinesiology�not just
among them. Kinesiology is composed of many subdisciplines; it is therefore
multidisciplinary. But multiband even cross-disciplinarity falls short, argues
Gill (2007): �Inter-disciplinary implies actual connections among subareas, and
an interdisciplinary kinesiology that integrates subdisciplinary knowledge is
essential�.
As you move forward in your
studies, your challenge is to start to see the many ways that kinesiology�s
subdisciplines inform one another�to see cross-disciplinary and
interdisciplinary connections. Your ultimate goal is to take an integrative
perspective to consider the many ways that knowledge from each area informs,
enhances, and complements your understanding of human movement.
Chapter Summary
From its humble beginnings in the
19th century, the field we know today as kinesiology has gone through many
changes. From unorganized efforts to provide health and fitness opportunities
for children, to the profession and eventual discipline of physical education,
to the move toward kinesiology, physical activity and human movement have
remained our core concerns. Kinesiology includes subdisciplines from the
natural sciences, social sciences, and humanities, all of which help us understand
how, when, and why people move.
(back
to content)
4.15 Radiesthesia History o
Abb� Mermet
RADIESTHESIA seems to be a
strange word to most people on both sides of the Atlantic. On the Continent,
however, every educated man knows what it means and the literature on the
subject is both extensive and popular, especially in France, Belgium and Italy,
where masters of the art and science of Radiesthesia have been practising it
successfully for the last few decades.
Abbe Mermet had the satisfaction
of being acclaimed during his lifetime as the �King of dowsers�, not only in
France but all over the continent of Europe. He was one of the few prophets who
gained recognition in his own country. Wherever he went he made an
unforgettable impression, not only by virtue of his amazing practical results,
but also by his unfailing willingness to help those in need of such material
things as water and coal, and those in distress about missing relatives whom he
invariably traced. And he did it all with a modesty akin to saintliness. He was
indeed a priest who had found his real vocation.
All kinds and conditions of men
consulted him from various parts of the world. A poor distressed widow in
France, whose son had been missing for some time; the chief engineer of the
world-famous firm of Suchard in Switzerland; a missionary in South America; and
even the Pope himself, who took a great interest in his work, all appealed to
him for help and guidance to solve problems which had left experts and specialists
completely baffled. And never did anyone appeal to him in vain.
Abbe Mermet almost invariably
gave the final and true answer without any thought of pecuniary reward.
Not only did he establish
Radiesthesia on a sound practical basis but he raised it to the level of a new
science, making people realise, in the words of Shakespeare, that �There are
more things in heaven and earth than are dreamt of in our philosophy.�
Radiesthesia may be defined as
sensitivity to radiations. And every one without exception is sensitive to
them. It is only a question of degiee. The word �dowsing� is the nearest
equivalent to Radiesthesia, but whereas dowsing is confined to searching for
latent water or minerals with a divining rod or pendulum, Radiesthesia covers
the whole field of radiations from any source, living or inert. Of late years,
Teleradiesthesia, which is prospection at a distance, has made great strides
and the subject is fully dealt with in the third part of the present work.
In this country, we have had some
notable medical pioneers in Radiesthesia, who unfortunately are no longer with
us. Special tribute should be paid to Drs E. W. Martin, W. Guyon Richards, E.
T. Jensen, Hector Munro, Dudley d�Auvergne Wright, to mention but the leading
ones. There are now quite a number of medical men who use Radiesthesia in their
practice. Indeed, we have a Medical Society for the Study of Radiesthesia in
London which publishes a quarterly journal.
This Society welcomes any
qualified medical man with an open mind on the subject, who wants to become
familiar with this fundamental approach to the nature of health and disease so
that the knowledge now acquired may be used both for diagnosis and treatment.
Many important works on
Radiesthesia have been written by Continental medical men, engineers and
chemists. In this country, we have a few eminent medical radiesthetists and
quite a number of distinguished amateurs. But none has ventured to write an
authoritative work on Radiesthesia for the guidance of the medical profession and
especially the general public.
The translation into English of
such a greatly needed work is indeed overdue, and the publishers have been
fortunate in securing the rights of what is generally regarded as the great
classic work on Radiesthesia, namely the present textbook written by the late
Abbe Mermet. Not only is it a work indispensable to any student or practitioner
of Radiesthesia, but it is also a perennial.
The first edition was published
before the war and it has been constantly revised and reprinted ever since, the
latest edition having appeared as recently as 1957.
In France, Abbe Mermet�s work has
been awarded a prize by the National Society for the Encouragement of Public
Welfare.
His remarkable achievements have
often been reported in the French Press and in particular his �Psychic
Radiesthesia� which enabled him to discover fields of petroleum in Africa,
Galicia and other parts of the world by distant prospection. He was consulted
by the Vatican authorities for important archaeological researches in Rome, all
of which met with success. The records are in the Archives of the Vatican
Library.
Over 5o,000 copies of Abbe
Mermet�s work on Radiesthesia have been sold and it shows no sign of being in
the least out of date. Abbe Mermet called it his testament and at long last we,
in this country, are called to be its legatees.
The nature of Radiesthesia has
not yet been finally elucidated but its practical results have been so firmly
established by a host of reputable research workers that a sceptical attitude,
or unwillingness to investigate, is no longer justified.
We do not understand the nature
of electricity but we go on using it simply because experience has shown that
it works.
Similarly, with Radiesthesia.
Preconceived ideas and prejudices due to our present imperfect knowledge of
scientific laws can only hinder human progress. We must approach Radiesthesia
with an open mind for, after all, it is the results that count.�
And here we have the finest possible opportunity of studying
the most comprehensive work that has yet been written on Radiesthesia, based as
it is on forty years� practical experience.
One of the greatest scientists of
our time, Dr Alexis Carrel, Nobel Laureate, and perhaps the most famous
research worker that the Rockefeller Institute in New York has ever had,
realized the importance of Radiesthesia over thirty years ago, and expressed
his opinion in the following words: �The physician must detect in every patient
the characteristics of his individuality, his resistance to the cause of the
disease, his sensitivity to pain, the state of all his organic functions, his
past as well as his future. He must keep an open mind free from personal
assumptions that certain unorthodox methods of investigation are useless.
Therefore, he should remember that Radiesthesia is worthy of serious
consideration.�
This translation is the English version of the posthumous
and definitive French edition, published in Paris in 1957, and includes all the
essential data concerning experiments and prospections which appeared in the
preceding editions.
Some technical and unusual words are fully explained in the
Preface
NO man can give more than what he
has and therefore one must not expect an author to impart more knowledge than
he possesses. Thus at the outset of a new work it should be carefully specified
what is involved and what is not. In this particular case we are dealing with
the subject of Radiesthesia, often called the art of dowsing. I have not
attempted to present a synthesis of other methods but only to give a detailed
exposition of one method among others, namely my own.
The reader will not find any
elaborate explanation in these pages. One�s intelligence, ever eager to find
out truth, and with good reason, concentrates on the causes of phenomena, and
this may well prove misleading and deceptive. Rather must one admit that, in
the present state of our knowledge, no theory appears to be satisfactory. The
same applies to the phenomena of light, heat, electricity, wireless and others.
If it is a question of undulations, what is the undulating substance?
One must have the wisdom to avoid coming to conclusions.
When an Indian fisherman first
got an electric shock from a torpedo-fish, or numb-fish, he would have been
utterly incapable of giving a true explanation of the phenomenon and his
impressions would have been purely imaginary, not to say absurd. It is better
to keep silent, rather than put forward chimerical theories with the risk of
preventing the developments of science at the outset, by confining them to some
preconceived hypothesis.
My intention in the present work
has been to set out, in an orderly manner, the facts observed in the course of
forty years� practice, to explain experiments with sufficient precision so that
they may be repeated by anyone, to expound a method which has proved its worth,
and to bring into relief some fundamental laws emerging from this somewhat
limitless and disconcerting subject of Radiesthesia. Criticism made in a truly
scientific spirit will be welcome.
In France, the pioneers in the
field of Radiesthesia have been, in the majority of cases, Catholic Priests who
invariably have a strong aversion to spiritualism, occultism and all kinds of
magic. Is it conceivable that if, in the course of their experiments, they had
discovered some suspicious element, they would have continued their researches?
The constancy of physical laws, their neutrality in regard to any religious or
philosophical question, constitute criteria showing that we are confronted with
purely natural forces. Therefore, if there is no co-operation with any
misleading influence, it is a question of pure science. It has always been a
fatal mistake to oppose real progress in Science, affecting not only those
responsible for such an attitude, which is of little importance, but also those
whose authority was unquestioned and whose supporters they gratuitously decided
to become. But this is not the first time that men with a religious vocation,
like shrewd detectives, have shown the way to a discovery useful to humanity.
There is no need to get alarmed in the present case. I am not to be held
responsible for the occult practices, more or less unconscious, to which some
people might become addicted under cover of my method.
I should like to make it quite
clear that I submit my work to the judgment of those in authority in the
Catholic Church who are not in the least likely to be led astray by unwarranted
claims on the part of any individual.
In this work, it seems to me that I have written a
supplementary chapter to the old textbooks of classical physics.
It may take many years before all
the phenomena of Radiesthesia are elucidated and its nature completely
understood including the range of wave-lengths involved, their periodicity,
their influence on environment, and the best method of capturing them and
controlling their effects so that they may be used to give beneficial results.
This work, therefore, is but an
outline, an accumulation of material intended to build, one day, a cathedral. I
hope it will also inspire other radiesthetists to reveal their own secrets and
thus create a fraternal link between all those devoting their efforts, hitherto
too individualistic, to the progress of Radiesthesia.
I must also express my deep
gratitude to all those who have helped me in this work, first to the members of
L�Association des Amis de la Radiesthesie who have urged and encouraged me to
write this book, and particularly to my friend Father de Belinay, s.j., whose
great knowledge has guided me at all times and prevented me from falling into
scientific heresies.
The reader will find here facts
and experiments, and certain laws, or rather constant manifestations of
radiesthetic forces, based on tentative hypotheses necessary for the
explanation of facts. But he will find no theory accounting for them. This is
quite intentional and the reason for it is obvious for no theory could account
for all the facts. Any explanation would be more obscure than the particular
fact to be explained. It is better, therefore, to remain silent and frankly
admit that we do not know.
In Radiesthesia some discover
various things while others discover explanations. In the practical field of discovery,
we can distinguish those who find something from those who never find anything.
But as far as discussion is concerned we are all equal and different views are
often expressed in radiesthetic circles.
It is a natural tendency of the
mind to find out the cause and explanation of any phenomenon. But when this is
impossible, the scientific attitude should be one of benevolent curiosity,
patient, obstinate; controlling one�s work, repeating, varying and multiplying
experiments in order to establish future theories on sound scientific foundations.
Actually, in Radiesthesia, it is only facts that are of primary importance.
Aristotle differentiated physics
from metaphysics. It would seem that Radiesthesia takes an intermediate place
between the two. By reason of its obvious similarities with the elements and
laws of classical physics, gravitation, light, heat, electricity, magnetism and
Hertzian waves, Radiesthesia is closely linked up with the group of sciences
which studies the laws and forces of Nature. On the other hand, owing to
certain results which might be regarded as supernatural, the apparent
disproportion of the means employed, and the mysteries associated with it which
it is not yet able to elucidate, Radiesthesia appears to be concerned with the
suspect domain of forces transcending those of Nature.
Among radiesthetists, I have
observed two tendencies. Some, endowed with a really scientific temperament,
see and seek in Radiesthesia a new branch of the physics of waves and
radiations. Others, possessing psychic and metaphysical tendencies, attracted
by the wonders*of occultism, aim at linking up Radiesthesia with phenomena of
abnormal hypersensibility or spiritism.
Personally, I must make my own
position quite clear. I regard Radiesthesia as being purely scientific. If it
had not been so, I should have given it up long ago. All the facts I have
observed, whether explicable or not, appear to be purely natural and the
mystery associated with them is of the same kind as that characteristic of
luminous, calorific and Hertzian waves. Hence my endeavours have always been to
discover the points of contact between these branches so closely akin to the
same science and I hope that those more learned than I will continue to
investigate on the same lines.
My own conviction is that those who try to associate
Radiesthesia with occultism are doing a great deal of harm to it.
I formally decline any solidarity
with them, any responsibility for their theories and explanations and terms
they use. Of course, one cannot stop anyone calling himself a radiesthetist but
it would be most unfair if the misconceptions of some misguided enthusiasts
should bring discredit to Radiesthesia.
And now let us discuss the
subject of distant prospection or Teleradiesthesia which is very topical.
Having practised it for over twenty years I may venture to give a word of
advice. A comparison may help us to see the subject in its proper light.
Let us imagine the case of a
surgeon who has discovered a new method of operating for cancer. In performing
100 operations, he achieved success in 80, leaving 20 failures. The president
of a society of surgeons suggests that he should perform two controlled
operations. Result: two failures. It would be fair to conclude: 102 operations,
80 successes and 22 failures. But the reckoning in this case is different: two
operations, two failures. All the facts involved, confirmed by the cured
patients themselves as well as by the professional staff, are ignored so that
the final impression is falsified.
Where would science be today if
only controlled experiments had been taken into account? And if, in the case
mentioned above, a generalised statement condemning the operation in question
had been made consequent upon two failures?
If students ^ Radiesthesia will
only proceed to work as explained in Chapter XIIL on a map or photograph, they
will find that it is not more difficult to succeed at a distance than on
location. Personally, after having surveyed a certain site, I never give a
final opinion without having controlled my work on a map or plan in the quiet
atmosphere of my own study.
There is a demand for results. In
the first edition of the present work, we gave 20 results. It is easy for
anyone to verify them. Dates, testimonies, references, are all there. Surely,
that should be enough.
Practical conclusion: when you
are asked to make a prospection, begin by making a study of the map or plan
representing the site. If you find nothing, do not go on the site.
If you feel anything, you should
go, if possible, in order to check up on the site. On returning, another
control should be made on the plan, map or photograph. Later on, with greater
experience, it will be unnecessary to go on the site but useful only to
indicate to those concerned where digging operations should be done to obtain a
good result.
It is, of course, understood that
to achieve a successful prospection on a plan, it is essential that it should
be property made. An ordinary piece of paper is not a plan. In chapter XII the
necessary conditions to be fulfilled for making a good plan are indicated. They
may be briefly summarised here. The plan should be so detailed (altitude, water
streams, forests, hedges, ditches, houses, etc.) that the teleprospector should
feel he is actually on the site itself. Black or white lines which may stand
for roads, paths, streams, tunnels, etc., are not sufficient indications.
Moreover, and this is also
essential, one must choose to work on a favourable day and at a favourable
time. Thus, to give an example, the teleprospectors who worked on the plans put
forward for the Congress of Paris (June 1933) a fortnight before the date of
the Congress must have encountered insurmountable difficulties as during that
time the atmosphere was highly charged with parasitic radiations.
One day I had to go to the South
of France to make a prospection but on that particular day parasitic radiations
were so strong that from nine o�clock in the morning until five o�clock in the
afternoon I found it impossible to detect a single stream.
For those who are feeling
sceptical about' these radiesthetic phenomena capable of disturbing and even
preventing any kind of work, either on the site or on paper, I will mention a
case in which I was both a witness and a victim. On 4th March 1933 I was called
to make a prospection in the small town of Penthalaz, near Lausanne
(Switzerland) with a view to increasing the water supply. Accompanied by a
pupil, I arrived on location at 1.30 p.m. We began to work right away. All was
going well when suddenly the pendulum stopped and refused to function.
I said that it must be due to
fading and advised waiting for a while but at � p.m. we were still waiting for
the end of the fading. In spite of all our efforts, and surveying the site at
different points, sometimes with the rod and sometimes with the pendulum, we
failed to detect anything at all. The pendulum remained motionless for three
hours both in the hands of my companion and in my own. As this happened in the
presence of the local council and the schoolmaster who had brought his pupils
to witness a demonstration of our radies-thetic powers, our embarrassment may
well be imagined.
When it was time to leave I said
to my audience: �There is something very serious happening in the atmosphere
today. It may be an earthquake or a volcanic eruption but I do not know for
certain.� The next day, I had a �phone call from Penthalaz:
�Have you seen the papers this morning? You were right
yesterday.�
And that morning the papers gave a full account of the
terrible tidal-wave catastrophe in Japan.
It is also worth noting that as
soon as I arrived home I tried to do my prospection on a plan with the same
negative result.
It was only at 6.40 p.m. that
suddenly the radiations reappeared and the pendulum began to move again.
This somewhat sensational example
serves to stress the fact that there are certain times and days when the
pendulum cannot be used.
And now little book, bearer of
proven truths, go wherever you find welcome in the five parts of the world.
Sustained by the indulgence of the learned, by the sympathy of colleagues, and
by the sole desire of doing good, with a prayer, too, that Heaven may not
withhold its blessing, go, teach all who seek with good will, to discover and
use those treasures that the earth hides from us, and, through the observation
of beneficent laws, to relieve the sufferings of humanity.
Abbe A. Mermet Recteur de la Chapelle de Sainte-Madeleine
President honoraire de 1�Association des Amis de la
Radiesthesie
Jussy, pres de Genkve, Suisse
(back
to content)
4.16
Bioresonance Therapy � a complementary medical method y
Michael Galle 2006
HISTORY
The bioresonance method was
developed in the 70s of the twentieth century by natural medicine oriented
physician Franz Morell and electronics engineer Erich Rasche out of the
medication test of electroacupuncture in accordance with Voll.
Using a sender for
electromagnetic vibrations which was in electrically conducting contact with
homeopathic medications and a receiver system which was connected to the
electroacupuncture measuring circuit, Morell and Rasche obtained the same
electrical skin conduction parameter changes on acupuncture points as if the
original medications were present in the measuring circuit. They thereupon
postulated that medicament information is marked by weak low-frequency
electromagnetic vibrations in the range of 1 Hz to 106 Hz and that consequently
� due to the physiological effects (resonances) on the acupuncture points -
such weak electromagnetic vibrations are part of the information transmission system
in human beings.
Therefore, based on the mode of
the tests and on the determined biological effects on the wholeness of human
beings, weak, coherent electromagnetic vibrations are postulated as information
carriers. However, they are not explicitly measurable. When there is contact
between a person and the unit, an electromagnetic white noise which is clearly
above the electronic white noise of the unit is measured. This active
electromagnetic white noise of human beings seems to provide the basis for the
transmission of information in an as yet unknown manner. In order to obtain a
first theoretical understanding of this phenomenology, Galle applied
explanatory concepts of biophoton theory to the low frequency electromagnetic
vibrations which are relevant in bioresonance therapy.
The therapeutic utilization of
this knowledge led to the development of bioresonance therapy. In this method,
the postulated electromagnetic vibrations are obtained via flat electrodes from
specific skin regions of humans. After optical uncoupling, they are inverted in
a phase constant manner in the unit (mirrored) and returned to the person as
therapeutic input.
This can be selectively applied either throughout the entire
frequency passage range (1 Hz � 20 0000 Hz) or with highly specific frequency
passage range.
The methodological approach of
Morell and Rasche was typical for experience healing. This method was developed
by means of input-output research on the wholeness (black box) of human beings.
Thus far, only relatively hypothetical explanatory models exist with regard to
the physical and physiological interactions. In order to test the reproducible
effect of a healing method, one does not, however, require
reductionistic-materialistic explanatory concepts.
Theoretical explanation is a claim, but not a necessary
criterion of natural science.
It is of historic interest that
at the same time, Fritz-Albert Popp and Bernd Ruth discovered biophotons. These
are weak coherent electromagnetic vibrations in the 1014 Hz range which are
emitted by living systems and to which, according to the theories of Popp and
his co-researchers, fundamental regulatory functions within living systems are
ascribed.
Bioresonance therapy has been
successfully applied by natural healing oriented practitioners worldwide for 30
years. There are numerous positive documentations of individual cases regarding
a variety of indications, including�among others - allergies and intolerances,
functional disorders, psychosomatic illnesses and the rheumatic forms. Scientists
have given more attention to Morell�s theses and practices particularly in the
last 10 years. Several work groups carried out clinical human studies as well
as plant and animal studies to verify the bioresonance method (see below).
The BICOM unit, the IMEDIS unit
and many other bioresonance units which work according to this method are built
in the manner of the MORA III unit which was developed by Morell and Rasche.
�
The Edwin Smith papyrus: written in Egypt in 1600 BC, it is
the oldest surviving surgical document.
(back to content)
4.17
Anthroposophic medicine w
HISTORY
Anthroposophic medicine grew out of the belief that health
is a matter of the whole person, not merely an absence of injury or disease.
Anthroposophic medicine at its
core is a response to a reductionism in medicine � that is, the idea that
health can be understood by examining only isolated parts of a system, its
chemical or cellular interactions and their resulting symptoms. Anthroposophic
medical practitioners instead view their patients as whole people, with
lifestyle, social and spiritual dimensions that contribute as much to their
overall well-being as their physical symptoms or injuries.
Anthroposophic medicine has its
origins in the wider Anthroposophic movement developed by Austrian scientist
and philosopher Rudolf Steiner. Anthroposophy aims to expand scientific
processes to increase understanding of the spiritual and social dimensions that
it views as equally important to human beings. Anthroposophy has practical
applications in several fields, including: Waldorf education
(https://www.freunde-waldorf.de/en/home/), where analytical thinking is taught
alongside activities to foster creativity, imagination and ethics; biodynamic
agriculture (https://www.sektion-landwirtschaft.org/en/), which emphasises
ecologically-friendly practices, such as using local plant varietals, crop
diversification, and avoidance of chemical fertilizers and pesticides;
architecture, most notably in the Goetheaneum (https://www.goetheanum.org/en/)
building in Switzerland; and, more recently, responsible banks and financial
institutions that aim to achieve positive social and environmental returns
alongside economic returns.
�
German scientist and philosopher Rudolf Steiner in 1905.
Dutch physician
�
Dutch physician Ida Wegman in 1899.
Anthroposophic medicine in
particular was developed in 1920 through a collaboration between Steiner and
Dutch physician Ita Wegman. Several small anthroposophic hospitals were set up
in Switzerland and Germany in 1921, followed by further development of
therapies, techniques, and medicines.
In 1925, Wegman and Steiner published the book Fundamentals
of Therapy
(https://ivaa.thoughtlabs.be/wpcontent/uploads/2021/09/Fundamentals_of_Therapy.pdf)[pdf],
which endorsed the scientific principles of conventional medical practice but
laid out a way to glean additional insights and enhance health outcomes by
understanding a patient as not merely a body, but also an individual with a
life, a soul and a spirit [see Therapeutic Approach
(https://ivaa.thoughtlabs.be/about-anthroposophic-medicine/therapeuticapproach/)
for more detail].
Between 1925 and 2000,
anthroposophic medical therapies continued to be developed and to gain
popularity, primarily within Europe. The German Medicine Act of 1976 legally
recognised anthroposophic medicine as a therapy system; it was later
incorporated into the national health systems of other countries, including
Switzerland and Brazil.
Since 2000, anthroposophic medicine has begun to gain
popularity worldwide, with interest increasing not only in clinical practice
but also in scientific research and publication.
In 2009, the World Health Organization adopted a resolution
(http://apps.who.int/medicinedocs/documents/s21477en/s21477en.pdf) [pdf] that
recognized �traditional medicine� as a resource that could improve �health
outcomes, including those in the Millennium Development Goals.� A subsequently
published 2014-2033 WHO strategy (http://www.who.int/traditional-complementaryintegrative-medicine/publications/trm_strategy14_23/en/)
noted that expanding access to traditional, complementary and integrative
medical therapies (including anthroposophic medicine) could help combat
escalating levels of illness and health care costs worldwide.
Currently, the IVAA and others
are part of a growing global movement to further increase the recognition of
anthroposophic medicine into national health systems, to improve access to
anthroposophic treatments and therapies and to improve the health of their
citizens.
(back
to content)
4.18 The Autogenic Training Method of J. H. Schultz w
Wolfgang Linden
THE HISTORY OF AUTOGENIC TRAINING
In the practice of stress
management, autogenic training (AT) is and remains a �classic�. It is one of
the oldest bio-behavioral techniques known and used. Although widely practiced
all over Europe, in Russia, and in Japan, AT is less popular in North America,
and may - undeservedly - have lost some of its luster given current advances
and enthusiasm about mindfulness therapies (Davidson, Kabat-Zinn, Schumacher et
al., 2003) which in many ways have overlapping rationales with AT.
The objective of this chapter is to describe AT, its
rationale, practice and outcomes but also to place AT within the current trends
of self -regulation therapies.
The German neurologist Johannes
Heinrich Schultz (1884-1970) is credited with the development and promulgation
of AT, which is considered a self-hypnotic procedure. During his medical
training in dermatology and neurology, Schultz became fascinated with
heterohypnosis, which, however, had a dubious image to many of his medical
supervisors and peers at that time. Initially, Schultz worked with hypnosis
only on his own time, outside of his regular clinic duties. The dominant
therapeutic approach then for mental and psychosomatic problems was
psychoanalysis but Schultz rejected analysis as a promising treatment for
psychosomatic disturbances. In a brief biography, Schaefgen (1984) cites
Schultz as having said that "it is complete nonsense to shoot with
psychoanalytic guns after symptom-sparrows."
The breakthrough of AT came after
Schultz opened his own medical practice in neurology and psychiatry in Berlin
in 1924, where he promulgated AT without the constraints of medical superiors
who did not share his vision. His first formal presentation of his experiences
with AT was in 1926, in front of his colleagues in the Medical Society; his
first book followed 6 years later (Schultz, 1932). In all he is accredited with
over 400 publications, numerous books, and translations of these into six
languages. His ground-breaking book on AT had seen 18 editions by 1984.
The development of AT has two
sources: Schultz's own experiences with clinical hypnosis, and Oskar Vogt's
observations in brain research. Schultz himself noted that his hypnotized
patients regularly reported two distinct sensations�a strange heaviness,
especially in the limbs, and a similarly unfamiliar sensation of warmth. He was
convinced that hypnosis was not something that the hypnotist actively did to
the learner but that individuals did to themselves. For the patient to enter
this state, there had to be a "switch," a point of change. Activating
this switch�placing the control in the hands of the patient�was what Schultz
wanted to achieve. Oskar Vogt's experiences further strengthened Schultz's
belief that it was possible to reliably trigger an autogenic state, because
Vogt, a brain researcher, had observed that his patients could volitionally
produce the sensations of heaviness and warmth and could switch into
selfhypnotic trance. Herein lay the seed for autogenic formulas which represent
a set of mental self-instructions to seek out particular physical sensations.
Over several years, Schultz further developed the idea of formulas to reliably
achieve deep relaxation and its accompanying sensations in various parts of the
body. The publication of his 1932 book on AT was the culmination of his efforts
to standardize the procedure.
AT remained unknown on the other
side of the Atlantic Ocean until one of Schultz's followers, Wolfgang Luthe, a
physician, emigrated to Canada and began clinical work, teaching, and research
about AT in English. A benchmark paper appeared in the American Journal of
Psychotherapy (Luthe, 1963); and this was later followed by a hefty six-volume
book series that Luthe coauthored with Schultz (Luthe, 1970a, 1970b, 1970c;
Luthe & Schultz, 1969a, 1969b; Schultz & Luthe, 1969). These volumes
provide extensive descriptions of supporting experimental research, case
studies, and clinical success reports of AT for a wide range of clinical
problems. For the reader with a strong empiricist bent, however, reading the
original works will likely be a frustrating task because in the ultimate evaluation
of AT's effectiveness no distinction is made by Schultz and Luthe among
opinions, single-case reports, and controlled studies (of which there were
precious few at the time). For a more detailed description of the background
research and applications, I refer the reader to my book Autogenic Training: A
Clinical Guide (Linden, 1990), and for diligent reports on outcome the reader
may want to peruse Stetter and Kupper�s (2002) work or Grossman et al�s (2004)
excellent meta-analysis, or a detailed review paper that combines a narrative
with a meta-analytic review approach (Linden, 1994).
(back
to content)
4.19 A Historical Look at Rudolf Steiner,
Anthroposophy, and Waldorf Education w
Author(s): P. Bruce Uhrmacher
udolf Steiner founded the first Waldorf school in Germany in 1919. Unique
elements of Waldorf education include an arts-based curriculum in which
students learn subject matter through a variety of forms of representation, a
pedagogy designed to meet students' developmental growth, an administrative
system in which teachers govern the school, an organization devoted to
sustaining a sense of community, and an integrated conceptual approach to
education generally-a place where the cosmic and the mundane are intertwined.
Rudolf Steiner's life and
writings are the foundations on which Waldorf schools are built. Therefore,
this article is devoted to an overview of his work, which should assist us in
understanding what goes on in contemporary Waldorf schools. Also, because Waldorf
schools in North America are based on the first Waldorf school, I have included
an examination of elements of that school's educational program. However, I do
not present a simple chronological account of Steiner's life or of the origins
of Anthroposophy (an outgrowth of Theosophy and the term used to denote the
path of spiritual development from which Waldorf education springs). Rather in
the last section of this article, I focus on possible reasons why Anthroposophy
has survived and continues to flourish many years after Steiner's death.
The first idea was to provide an
education for children whose parents were working in the Waldorf-Astoria
factory, and as the Director was a member of the Anthroposophical Society, he
asked me to arrange this education. .... And so, in the first place, the
Waldorf School arose as a school for humanity as such, fashioned, it could in
fact be said, out of the working class. ... Here then, we have an educational
institution arising on a social basis, that seeks to found the whole spirit and
method of its teaching upon Anthroposophy.'
-Rudolf Steiner A Modern Art of Education
Because Rudolf Steiner's life and
writings are the foundation on which Waldorf schools are built, this essay is
devoted to an overview of Steiner's work, which should assist us in
understanding what occurs (or perhaps what should occur) in contemporary
Waldorf schools. Rudolf Steiner (1861-1925) is not widely known among American
educators. Perhaps this is because his ideas do not fit neatly into any one
sphere of knowledge. He was neither full-time educator, nor philosopher, nor
artist, nor critic.� In addition, his
pantheistic and angelological outlook rattles many contemporary scholars and
makes him suspect among scientifically oriented communities. His understanding
of human nature, which consists of physical, etheric, astral, and ego bodies,
certainly demands a great deal of open mindedness from students trained in
mainstream academia. Morever, he expounded esoteric ideas, wrote obtusely, and
often lectured with dogmatic conviction. Why is it then that anyone ought to be
familiar with Dr. Steiner?
One reason is that oftentimes the
best way to see one style of education is by examining others. Making the
strange familiar and the familiar strange are two guiding slogans for cultural
anthropologists. My point is that for anyone interested in understanding or
improving public schools, one important place to start is with the
investigation of other types of school systems. This argument is premised on
the observation that alternative schools exist because of some dissatisfaction
with mainstream schooling. In order to remedy the concerns, the alternative
school will develop its own style of education. For example, teachers may teach
differently or offer alternative types of curricula. Educational issues
currently forgotten, dismissed, or simply unexamined may be addressed.
Another reason for examining the
roots of Waldorf education is to understand the undergirding of current Waldorf
schools and teacher training programs.2 There are over 500 Waldorf schools
worldwide and about 200 in North America (Canniff 1990). The United States also
houses four major Waldorf teacher training institutions. The fact that there
are many Waldorf schools spanning the globe from Germany, Scandinavia, and the
United States to Brazil, Argentina, Japan, and India is noteworthy in itself.
Students of education should not
ignore an educational movement that has generated 500 schools worldwide any
more than zoologists should ignore a newly found species-if for no other reason
than parents want to know about them. Yet, little scholarly research has been
conducted on Waldorf schools, in the world at large or in the United States
(Uhrmacher 1991). The topic is unlisted in the Encyclopedia of Educational
Research, and a search for studies on Waldorf education through conventional
resources provides little material.
Thus, educators ought to know
about the impetus of Waldorf education. Where did it begin? For what reasons?
With what methods? To these ends, let us examine Rudolf Steiner's ideas, in
particular his ideas about Anthroposophy. In the last section of this article,
I focus on possible reasons why Anthroposophy, the key to understanding Waldorf
education, has survived seventy years after Steiner's death. My final point is
not an empirical one. That is, I am not suggesting that Waldorf education or
Anthroposophy will become a mass movement. Rather, my claim is that the themes
generated from this movement have relevance for us all.
THE ORIGIN OF WALDORF EDUCATION
On 23 April 1919, Rudolf Steiner
gave a lecture in the tobacco storeroom of the Waldorf-Astoria cigarette
factory in Stuttgart, Germany (Carlgren 1981). Armistice had come into effect
on 11 November 1918. People were tired of war, concerned about social upheaval,
worried about the collapsing economy, and threatened by the possibility of a
German civil war. Crowded on benches and chairs, sitting on large bags of
tobacco, lining the walls in the back of the room, the workers listened as this
philosopher, in his starched white shirt, immense cravat, and black frock coat,
expounded on the themes in his newly published book, The Threefold Commonwealt (h1
966b). Steiner argued that three spheres of social life-the spiritual-cultural,
legal-political, and economic-must be decentralized within the modern state.
Offering hope of a new social/world order, Steiner was suggesting that
education could play an important role in shaping society.
In his view, constitutional
states should limit themselves to the enactment and enforcement of laws to
protect their citizens, and not become involved in economic or cultural
affairs. Economic concerns, he said, should transcend political boundaries by
building a sense of "fraternity" with producer and consumer
associations. Why, he asked rhetorically, should national political concerns
impede or obstruct economic considerations? In effect, Steiner was arguing for
a common European market. Also, by separating the spiritual-cultural sphere
from both government and industry, Steiner hoped to affect the technocratic
order of the day. Rather than sustaining a system of tracking, whereby
individuals were trained in a way that met the needs of the industrial world,
Steiner believed that individuals should be encouraged to develop their own
natural talents. Steiner said, "All of you, as you sit here, from the
sixteen-year-old girl apprentice to the workers in their sixties, suffer from
the fact that your real personality has been buried because from a certain moment
there was only the hard school of life for you, but no longer any real
education" (Carlgren 1981).
The workers were as impressed
with this social philosopher as Emil Molt, the head of the firm, had hoped.
After all, Steiner offered hope for a new society-one liberated from the
powerful modern state. Steiner's views embraced strong antihierarchical
notions. Following the lecture, Molt asked Steiner if he would create a school
for the workers' children. No stranger to the field of education, Steiner said
he would, if several conditions were met: the school should be open to all
children regardless of social or economic background, it should offer a
twelve-year curriculum (Barnes 1980), and it should be nondenominational in
religious orientation. The conditions were agreed on, and the first Waldorf
school, taking its name from the Waldorf-Astoria cigarette factory, opened five
months later, in the fall of 1919.
Before his death in March 1925,
Steiner would live to see the opening of four Waldorf schools, two in Germany
and one each in the Netherlands and Great Britain. By 1938 there were nine
Waldorf schools, but most of these closed during the war (von Baravalle 1967).
The first Waldorf school in the United States opened in 1928 in New York City
through the efforts of Irene Brown, who had heard Steiner lecture at Oxford.
There were four American Waldorf schools in 1947 (Staley 1988), eighteen in
1975 (Ogletree 1979), and seventy-five in 1989. Today there are over 150
Waldorf schools in North America. In fact, in the United States some Waldorf
schools are becoming part of the public school system. Why have Waldorf schools
continued to proliferate long after their founder passed away? Why has a school
that opened at the beginning of the twentieth century in Germany continued to
flourish in the United States as we near the end of the century?
Just who was Rufolf Steiner? What ideas did he have about
education?
STEINER'S EARLY IDEAS
Rudolf Steiner was born in 1861
to Austrian parents in the small town of Kraljevec in Upper Austria. His father
worked for the railroad and before Rudolf was eight the family had moved three
times. Although several works examine the life of Rudolf Steiner (Easton 1980;
Hemleben 1975; Shepherd 1954; Wilson 1985), his autobiography illuminates his
early intellectual development most thoroughly. Clearly, what shaped Steiner's
thinking most radically were numerous "supersensible" experiences.
When Steiner was eight, an apparition is said to have appeared to him and asked
for assistance. Bewildered, Steiner was not sure how to help, but he was
certain of what he had seen. The next day Steiner learned that the woman who
had come to him, one of his cousins, had died. This experience and others like
it pointed Steiner to "undeniable truths." He remarked, "For the
reality of the spiritual world was to me as certain as that of the physical. I
felt the need, however, for a sort of justification of this assumption"
(Steiner [1923] 1951).
As a result of his working-class
origins and his father's desire that he become an engineer, Steiner attended
the Realschule instead of the Gymnasium, and the Vienna Polytechnic (a
working-class college) instead of a university (Hemleben 1975). His inquisitive
nature and desire to make sense out of his uncommon experiences, however, led
him to a passionate study of geometry ("Geometry seemed to me to be a
knowledge which appears to be produced by man, but which, nevertheless, has a
significance quite independent of him" (Steiner [1923] 1951)), of Kant
("In my boyish way, I was striving to understand what human reason might
be able to achieve toward a real insight into the nature of things"), and
of Fichte ("And yet I had my own views. So, I took the Science of
Knowledge and rewrote it, page by page").
At the age of twenty-two Steiner,
through the recommendation of his humanities teacher Karl Julius Schr�er, was
selected to edit and comment on Goethe's scientific works for the popular book
series, Deutsche National-literatur (German National Literature). Goethe's
scientific works were not taken seriously by most scholars; "in effect,
Steiner was being tossed a scrap that no one else wanted" (Wilson 1985).
Goethe's science, however, corresponded quite well with Steiner's viewpoint.
Like Goethe, Steiner believed in understanding a living, whole world rather
than a dead, dissected one. And like Goethe, Steiner believed in a spiritual
world that interpenetrated the physical. In 1886 he published his first book,
Theory and Knowledge in the Light of Goethe's Weltanschauunga, nd in 1890
Steiner moved to Weimar to edit Goethe's natural scientific writings for the
Goethe and Schiller Archives.
Steiner stayed in Weimar for
seven years. In addition to editing Goethe's works, he assisted in organizing
the works of Schopenhauer and of the poet Jean Paul Richter. At the same time,
Steiner received his Ph.D. from the University of Rostock with his
dissertation, "The Fundamental Problem of the Theory of Knowledge, with
Particular Reference to Fichte's Teaching." Also, he published ninety-one
texts (essays, articles, or transcribed lectures) (Hemleben 1975) in addition
to four books, Truth and Science (his dissertation), The Philosophy of Freedom,
Friedrich Nietzsche Battler Against His Time, and Goethe's Conception of the
World each is, in part, a philosophical assault on the materialistic thinking
that pervaded common ideas of the time.
Between 1897, when he left Weimar
for Berlin, and 1919, when he opened the first Waldorf school in Stuttgart,
Steiner's writing began to change. Esoteric theological themes began to pervade
his work. Although he edited literary magazines (Magazin� f�r Litteratur, Dramaturgische Bl�tter),
lectured at the Workers' Educational Institute (1899-1904), and published some
texts that might be read by a general audience (e.g., Riddles of Philosophy,
Haeckel and His Opponents , and The Threefold Commonwealth) he also wrote
mystery plays (The Portal of Initiation, The Soul's Probation, The Guardian of
the Threshold The Soul's Awakening) and books disclosing the travel of the soul
(Theosophy, Occult Science: An Outline), and developed a new spiritual art form
called "eurythmy." Designed to make sound visible with the body,
eurythmy expresses words or musical tones through specific movements.
In addition, Steiner designed and
constructed the first Goetheanum (1913- 1920), in Dornach, Switzerland. The
building was architecturally designed to enhance spiritual awakening through
its seven varieties of wood, its utilization of clay, stone, glass, and other
organic materials, and its overall structural form.
Steiner had probably become
acquainted with Theosophy as early as 1888 (Wilson 1985); by 1900 he was giving
lectures to Theosophical circles. Appealing to the intelligentsia throughout
Europe, Theosophy combined a study of world religions, ancient mysteries,
philosophy, science, and psychic investigation. According to one of the
original founders, Helen Petrovna Blavatsky:
Theosophy is ... the archaic
Wisdom-Religion the esoteric doctrine once known in every ancient country having
claims to civilization. This "Wisdom" all the old writings shows an
emanation of the divine Principle; and the clear comprehension of it is
typified in such names as the Indian Budh (sic), the Babylonian Nebo, the Thoth
of Memphis, The Hermes of Greece ... and finally the Vedas, from the word
"to know." (Cooper 1979)
There was much in Theosophy that Steiner embraced.
In fact, some suggest that he
borrowed more from Theosophy than he was later willing to admit (Clemen 1924;
Wilson 1985). However, others perceive Steiner as a confused, opportunistic
young man who was initially anti-Christian (his work on Nietzsche has an
existential quality to it), but later became religious, in part because he
could capitalize on the German religious revival. Numerous esoteric movements
such as Ariosophy and Theosophy were becoming quite popular in Germany (Berman
1989). Steiner, however, defends his later works by noting:
I had to make a certain position
for myself in the world first. People may say nowadays that my writings are
mad, but my earlier work is there also, and they cannot wholly ignore it. And
moreover, I had to bring things to a certain clarity in myself, to a point
where I could give them form, before it was possible to talk about them. That
was not so easy. And then-I admit it frankly--it needs courage to speak openly
about such things. I had first to acquire this courage. (Clark 1970)
In any case, he became general
secretary with the founding of the German section of the Theosophical Society
in Berlin in 1902, and he participated in the society until 1912. At that time,
when Theosophists declared Krishnamurti their new Christ, Steiner broke with
the group, and took the German chapter with him to form the Anthroposophical
Society.
ANTHROPOSOPHY
Although some critics dismiss
Anthroposophy as "a hodgepodge of 19thcentury romanticism, Christianity,
Eastern mysticism and various perplexing notions" (McGrath 1977), and
others regard it as "a synthetic mixture, a surface barbarization of the
Gospel by means of Indic, gnostic, and mystery elements" (Aulthaus 1962),
adherents suggest that Anthroposophy's credibility should be tested by its
results, and indeed, even the two critics mentioned here (McGrath and Aulthaus)
admit that the results are impressive.
The word itself is derived from "anthropos" (man)
and "sophia" (wisdom).
To delve into all of its tenets
requires a dissertation (see Geoffrey Ahern 1984), but three key points should
be understood. First, according to Steiner, intertwined with the visible world
is a spiritual one. Steiner was arguing not only that a spiritual world exists,
but that the spiritual world interpenetrates the sense world. All attempts to
deny the existence of the spiritual world or to solve problems on a solely
material level were doomed to fail. What was needed was the recognition of the
larger spiritual reality that has an impact on the material world. Like Spinoza
and Goethe, Steiner embraced what philosophers call "psychophysical double
aspectism." That is, the mind and body are inseparable: What affects the
body is experienced in the mind, consciously or unconsciously, through emotions
or thoughts.
Morever, according to Steiner,
"knowing does not consist in a mirroring of something possessing essential
being, but the soul's living entrance into this reality of being" (Steiner
[1923] 1951). The goal of the process of knowledge is to raise one's
consciousness so that one can experience (or inwardly see) ideas in addition to
sense perceptions. In this way, concept and percept become one.
This last point leads to the
second key tenet behind Anthroposophy: human beings have the potential to
perceive and enter into the spiritual world. Here, Steiner was arguing against
Kantians who admit things-in themselves, but suggest that there are limits to
knowledge. Within us, said Steiner, are latent organs of perception that can
penetrate the spiritual world. In order to develop such organs, however, people
must first develop themselves, a difficult and formidable challenge. In
addition to numerous recommended meditation exercises (described in Steiner's
Knowledge of the Higher Worlds and Its Attainment ([first published in German
in 1904] 1947) and An Outline of Occult Science ([first published in German in
1909] 1972)), cultivating one's sense of the beautiful, sympathizing with
fellow beings, thinking (i.e., studying geometry), and developing powers of
observation are important preparatory stages. After years of patience and
practice, one begins to develop spiritual organs that allow entry into the spiritual
world.
In each of three stages, which
Steiner called Imagination, Inspiration, and Intuition, the individual develops
a different aspect of himself and is permitted greater access to the spiritual
(Steiner [1904] 1947).
The third key principle behind
Anthroposophy is that when spiritual investigators achieve the intuitive stage
of apprehension they consciously enter into an objective spirit, the findings
from which, to some degree, can be articulated and tested. Summarizing
Steiner's viewpoint, Robert McDermott writes,
Steiner in effect says: let
future spiritual scientists observe the validity of my spiritual perception,
and let the scientist limited to empirical observation note the extent to which
observable phenomena not only correspond to, but are illumined by, the insights
of Spiritual Science. (McDermott 1984)
By meditating in the way that he did, Steiner suggested that
anyone could see what he saw.
As a result of his spiritual
research, Steiner offered comprehensive, complex, and spiritually based views
of virtually every aspect of life. Several important results of his spiritual
science influence Anthroposophical thoughts even today: Steiner's cosmology,
his understanding of humankind, and his ideas on child development.
STEINER'S COSMOLOGY AND UNDERSTANDING OF HUMANKIND
Steiner suggested that the
universe condensed from spirit into matter through successive stages, and that
it will become spirit again with human assistance. The midpoint in this general
evolution occurred at the mystery of Golgotha. He also referred to this
phenomenon as "the Christ event" and suggested that it represents the
possibility of change in the evolution of the soul. The Christ event, said
Steiner, allows free spiritual activity to be achieved by changing ordinary thinking
into pure thinking: "This pure thinking then raises itself to the direct
experience of the spiritual world and derives from it the impulses to moral
behaviour" (Easton 1980).
For Steiner, to accept Christ within is to open up one's
powers of perception.
The evolution of the soul, as
alluded to above, is a central element of Steiner's cosmology. In fact, Steiner
thought that by explicating the operations of reincarnation to Europe he was
offering a "Copernican revolution." Of course, this idea never reached
revolutionary proportions in the West. Anthroposophists, however, embrace
personal reincarnation as a fundamental truth. Summarizing Steiner's ideas,
Stewart Easton writes:
What Steiner taught was that a
human being brings with him into a subsequent life on earth a frame work of
destiny that has been determined by previous lives on earth.... Man is thus
given the opportunity to compensate for his previous evil deeds, while at the
same time any spiritual progress that he has made in his earlier incarnations
will also be reflected in the karma that he brings with him to his new life on
earth. (P. 143)
Reincarnation allows individuals to develop their souls.
Anthroposophists not only accept
Steiner's cosmology, but they use their esoteric knowledge in numerous ways.
Waldorf teachers, for example, try to create harmony in their classroom by
relating the microcosm to the macrocosm-the curriculum to the cosmos (Uhrmacher
1991). Moreover, many assumptions about education stem from Steiner's ideas
about destiny, For instance, because Anthroposophists believe in reincarnation,
the essence of the individual is preordained in the same way that a rose bush
is. A rose bush will turn into a rose bush and not an apple tree. Still, a rose
bush must be cared for and pruned. A rose bush can turn into a beautiful
foliage or a scraggly shrub. Similarly, the kind of individual one turns into
depends on many factors-especially education. Anthroposophists also believe in
free will.
In addition to apprehending the
workings of the universe at large through spiritual science, Steiner's visions
also revealed to him the nature and development of humankind. He divided the
human being into numerous categories. His full-blown account includes nine
analytical divisions: physical body, ether body, soul body, sentient soul,
intellectual soul, consciousness soul, spirit-self, life-spirit, and spirit-man
(Steiner [originally published in German in 1904] 1971). More often, however,
Steiner wrote about and lectured on the human constitution from triadic
perspectives: body, soul, and spirit; head-man, chest-man, and limb-man; the
organism as thinking, feeling, and willing; consciousness as waking, sleeping,
and dreaming; and the physical constitution as nerve-senses, rhythm, and
metabolism. Regardless of the way Steiner chose to speak about human nature,
three points should be remembered. First, he acknowledged that his analysis is
constructed, and pointed out that one should not confuse of Golgotha. He also
referred to this phenomenon as "the Christ event" and suggested that
it represents the possibility of change in the evolution of the soul. The
Christ event, said Steiner, allows free spiritual activity to be achieved by
changing ordinary thinking into pure thinking: "This pure thinking then raises
itself to the direct experience of the spiritual world and derives from it the
impulses to moral behaviour" (Easton 1980).
For Steiner, to accept Christ within is to open up one's
powers of perception.
The evolution of the soul, as
alluded to above, is a central element of Steiner's cosmology. In fact, Steiner
thought that by explicating the operations of reincarnation to Europe he was
offering a "Copernican revolution." Of course, this idea never
reached revolutionary proportions in the West. Anthroposophists, however,
embrace personal reincarnation as a fundamental truth. Summarizing Steiner's
ideas, Stewart Easton writes:
What Steiner taught was that a
human being brings with him into a subsequent life on earth a framework of
destiny that has been determined by previous lives on earth.... Man is thus
given the opportunity to compensate for his previous evil deeds, while at the
same time any spiritual progress that he has made in his earlier incarnations
will also be reflected in the karma that he brings with him to his new life on
earth.
Reincarnation allows individuals to develop their souls.
Anthroposophists not only accept
Steiner's cosmology, but they use their esoteric knowledge in numerous ways.
Waldorf teachers, for example, try to create harmony in their classroom by
relating the microcosm to the macrocosm-the curriculum to the cosmos (Uhrmacher
1991). Moreover, many assumptions about education stem from Steiner's ideas
about destiny, For instance, because Anthroposophists believe in reincarnation,
the essence of the individual is preordained in the same way that a rose bush
is. A rose bush will turn into a rose bush and not an apple tree. Still, a rose
bush must be cared for and pruned. A rose bush can turn into a beautiful
foliage or a scraggly shrub. Similarly, the kind of individual one turns into
depends on many factors-especially education. Anthroposophists also believe in
free will.
In addition to apprehending the
workings of the universe at large through spiritual science, Steiner's visions
also revealed to him the nature and development of humankind. He divided the
human being into numerous categories. His full-blown account includes nine
analytical divisions: physical body, ether body, soul body, sentient soul,
intellectual soul, consciousness soul, spirit-self, life-spirit, and spirit-man
(Steiner [originally published in German in 1904] 1971). More often, however,
Steiner wrote about and lectured on the human constitution from triadic
perspectives: body, soul, and spirit; head-man, chest-man, and limb-man; the
organism as thinking, feeling, and willing; consciousness as waking, sleeping,
and dreaming; and the physical constitution as nerve-senses, rhythm, and
metabolism. Regardless of the way Steiner chose to speak about human nature,
three points should be remembered. First, he acknowledged that his analysis is
constructed, and pointed out that one should not confuse his constructs for
reality. Second, he recognized the interdependence of categories and stressed
that one should never become too rigid in thinking about the human being.
Third, Steiner was aware that his perspective was unconventional. He commented,
It is all too easy for the world
to laugh at our saying that the human being consists of a physical body,
etheric body, astral body, and ego. As long as one judges these matters only
with the yardstick of customary science, one cannot help laughing.... But
considering the serious tangle in which our civilization finds itself, one
would expect at least some readiness to seek for what cannot be found
elsewhere. (Steiner [1923] 1988a)
(back
to content)
4.20 Music Therapy in Traditional African
Societies: Origin, Basis and Application in Nigeria
Charles O. Aluede
ABSTRACT The use of music in
healing and healing rites in African traditional societies is as old as the
origin of African Continent. This paper attempted a historical origin of this
art, provides a theoretical basis for Music Therapy in Africa and concludes by
specifically highlighting areas where the use of Music Therapy has yielded
fruitful results in Nigeria.
History of Music Therapy | American Music Therapy
Association (AMTA)
�
Concert at Blackwell�s Island/Dr. Corning
The earliest known reference to
music therapy appeared in 1789: an article in Columbian Magazine titled Music
Physically Considered. The first recorded music therapy intervention &
systematic experiments in music therapy were conducted in the 1800s.
ARCHIVES OF THE AMERICAN MUSIC THERAPY ASSOCIATION
The idea of music as a healing
influence which could affect health and behavior is as least as old as the
writings of Aristotle and Plato and in some cultures, long before that. The
20th century profession formally began after World War I and World War II when
community musicians of all types, both amateur and professional, went to
Veterans hospitals around the country to play for the thousands of veterans
suffering both physical and emotional trauma from the wars. The patients'
notable physical and emotional responses to music led the doctors and nurses to
request the hiring of musicians by the hospitals. It was soon evident that the
hospital musicians needed some prior training before entering the facility and
so the demand grew for a college curriculum. A very brief historical glimpse of
this fascinating profession follows, below.
EARLIEST REFERENCES
The earliest known reference to
music therapy appeared in 1789 in an unsigned article in Columbian Magazine
titled "Music Physically Considered." In the early 1800s, writings on
the therapeutic value of music appeared in two medical dissertations, the first
published by Edwin Atlee (1804) and the second by Samuel Mathews (1806). Atlee
and Mathews were both students of Dr. Benjamin Rush, a physician and
psychiatrist who was a strong proponent of using music to treat medical
diseases. T he 1800s also saw the first recorded music therapy intervention in
an institutional setting (Blackwell�s Island in New York) as well as the first
recorded systematic experiment in music therapy (Corning�s use of music to
alter dream states during psychotherapy).
EARLY ASSOCIATIONS
Interest in music therapy
continued to gain support during the early 1900s leading to the formation of
several short-lived associations. In 1903, Eva Augusta Vescelius founded the
National Society of Musical T herapeutics. In 1926, Isa Maud Ilsen founded the
National Association for Music in Hospitals. And in 1941, Harriet Ayer Seymour
founded the National Foundation of Music T herapy. Although these organizations
contributed the first journals, books, and educational courses on music
therapy, they unfortunately were not able to develop an organized clinical
profession.
EARLY EDUCATIONAL PROGRAMS AND ADVOCATES
In the 1940s, three persons began
to emerge as innovators and key players in the development of music therapy as
an organized clinical profession. Psychiatrist and music therapist Ira
Altshuler, MD promoted music therapy in Michigan for three decades. Willem van
de Wall pioneered the use of music therapy in state-funded facilities and wrote
the first "how to" music therapy text, Music in Institutions (1936).
E. T hayer Gaston, known as the "father of music
therapy," was instrumental in moving the profession forward in terms of an
organizational and educational standpoint. The first music therapy college
training programs were also created in the 1940s. Michigan State University
established the first academic program in music therapy (1944) and other
universities followed suit, including the University of Kansas, Chicago Musical
College, College of the Pacific, and Alverno College.
The American Music Therapy Association (AMTA) was formed in
1998 as a merger between the National Association for Music Therapy (NAMT) and
the American Association for Music T herapy (AAMT).
AMTA united the music therapy
profession for the first time since 1971. Currently, AMTA is the intellectual
home for, and it serves member music therapists, students, graduate students
and other supporters. AMTA's mission is to advocate and educate for the music
therapy profession as a whole. AMTA publishes two research journals as well as
a line of publications, serves as an advocate for music therapy on the state
and federal levels, promotes music therapy through social media streams, and
provides research bibliographies, podcasts, scholarships, and newsletters to
its members.
AMTA is the single largest music therapy association in the
United States, representing music therapists in the United States and in over
30 countries around the globe.
The mission of the American Music
Therapy Association is to advance public knowledge of the benefits of music
therapy and to increase access to quality music therapy services in a rapidly
changing world.
CERTIFICATION BOARD FOR MUSIC THERAPISTS
The Certification Board for Music
Therapists (CBMT) is a separate and distinct organization from AMTA, which was
incorporated in 1983 to strengthen the credibility of the music therapy
profession by assuring the competency of credentialed music therapists. The
first music therapy board examination was administered two years later. CBMT
has been fully-accredited by the National Commission for Certifying
Agencies since 1986 and is
committed to maintaining certification and recertification requirements that
reflect current music therapy practice. To date, there are over 8,000
certificants who hold the credential Music Therapist-Board Certified (MT-BC).
Though CBMT and AMTA are separate, independent organizations, they often work
together to achieve recognition for the music therapy profession and the MT-BC
credential.
NATIONAL ASSOCIATION FOR MUSIC THERAPY
The National Association for
Music Therapy (NAMT) was founded at a meeting in New York City on June 2, 1950.
NAMT succeeded where previous music therapy associations previously failed by
creating a constitution and bylaws, developing standards for university-level
educational and clinical training requirements, making research and clinical
training a priority, creating a registry and, later, board certification
requirements, and publishing research and clinical journals. NAMT operated from
1950-1997 and saw the creation of a board-certification program (1985), a
critically-acclaimed Senate Hearing on Aging (1991), and the growth of music
therapy from a few dozen practitioners to thousands. *photo of Hospital Music
Newsletter courtesy of National Music Council.
AMERICAN ASSOCIATION FOR MUSIC THERAPY
Originally called the Urban
Federation of Music Therapists, the American Association for Music Therapy
(AAMT) was established in 1971. Many of the purposes of AAMT were similar to
those of NAMT, but there were differences in philosophy, education and
approach.
Starting in 1980, AAMT published
its own research and clinical journal, Music Therapy and by 1997, AAMT had
grown to 700 members.
HISTORY AND RATIONALE FOR DELINEATING LEVELS OF PRACTICE IN
MUSIC THERAPY
When the Commission on Education
and Clinical Training made its recommendations to the Association, some of the
recommendations in its 2000 report to the Assembly of Delegates were not
adopted in the Standards for Education and Clinical Training and were appended
to that document as �Issues for Future Consideration.� The Commission also
recommended changes in the organizational structure, to include committees on
Program Approval and Internship Roster, as well as an Overview Committee. The
Overview Committee was to be charged with internal and external monitoring of
standards, considering competency requirements, examining trends and needs,
giving advice concerning the Association�s role and responsiveness in the areas
of education and training, and acting as liaison to the Certification Board for
Music Therapists (CBMT) and other outside agencies. The 2001 report of the
Implementation Task Force supported the changes in the organizational structure
recommended by the Commission.
In 2001 the Assembly of Delegates
charged a Task Force on Organizational Restructuring to develop this new
structure. In 2002, the Assembly adopted the proposed new organizational
structure, which included an Education and Training Advisory Board. This board
was created to serve as a visionary body to advise, inform, and make
recommendations to the American Music Therapy Association (AMTA) on issues
related to music therapy education and training. It was charged to analyze
policy issues that focus on standards and professional competencies for
advanced levels of education and training; and more specifically, the
relationship of these standards and competencies to advanced degrees, education
and training requirements, levels of practice, professional titles and
designations, and various state licensures.
In carrying out these charges,
the Education and Training Advisory Board was to address the �Issues for Future
Consideration." Prior to its first meeting in November 2003, the Advisory
Board reviewed a comprehensive packet of published literature, AMTA documents,
and AMTA internal reports related to music therapy education and training from
1960 to the present. At the meeting, the Advisory Board discussed the literature
and then focused on the prioritization of tasks. The Advisory Board determined
that it was necessary to delineate levels of practice in music therapy in order
to provide the foundation for the development of advanced competencies. From
its inception, the Advisory Board worked according to one fundamental
principle: that no recommendation would be forwarded to the Association unless
it was unanimous.
After much discussion, the
Advisory Board agreed that defining levels of practice in music therapy was a
top priority for the profession as well as a foundation for other high priority
tasks. Each Advisory Board member then researched and wrote a paper from
her/his respective area of expertise related to this topic.
Differential levels of music
therapy clinical practice have been described for decades in the music therapy
literature (Bruscia, 1989, 1998; Gfeller & Thaut, 1999; Maranto, 1993;
Scartelli, 1989; Standley, 1989; Wheeler, 1983). Suggested levels have been
based on types of goals, depth and extent of services, and/or independence of
the music therapist. Gfeller and Thaut, Scartelli, and Standley related levels
of practice to educational preparation. The Commission on Education and
Clinical Training (AMTA, 1999) similarly suggested that while the Bachelor's
degree is designed to impart Professional Competencies for music therapy
practice, the Master's degree could prepare the music therapist to work at a
more advanced level, "depending on the clinical components of the degree
program" while the doctoral degree would not only provide competence in
research, teaching, and supervision, but also advanced competency in a
"specialization area in music therapy."
The clinical music therapy
literature describes several music therapy models that require substantial
training and expertise beyond the AMTA Professional Competencies. These models
include Analytical Music Therapy (AMT; Priestly, 1994), the Bonny Method of
Guided Imagery and Music (BMGIM; Grocke & Bruscia, 2002), and
Nordoff-Robbins Music Therapy (NRMT; Nordoff & Robbins, 1977). Several
authors have described other treatment approaches that represent advanced or
highly specialized clinical practice (e.g., Austin, 2001; Gfeller, 2001) or
advanced areas of practice such as supervision (e.g., Forinash, 2001) and
education and training (e.g., Wheeler, 2003; Wigram, Pedersen, & Bonde,
2002). Still others have modeled a level of practice beyond the Professional
Competencies by developing methods of assessment (e.g., Coleman & Brunk,
1999; Wigram, 2000) or by proposing theories of music therapy (e.g., Kenny,
1989; Thaut, 2000).
The urgency of the need for AMTA
to define levels of music therapy practice has increased with recent
legislative and regulatory actions in several states that have specified how
and under what circumstances music therapists may practice. By defining levels
of music therapy practice, AMTA will be prepared proactively to partner with
state legislatures and regulatory bodies in the development of occupational
regulations that affect music therapy services.
Defining levels of practice in music therapy serves as the
foundation toward achieving the following objectives for the Association:
1. Identify advanced competencies, both global and in areas
of specialization, along with analysis of existing professional competencies
2. Develop education and clinical standards for graduate
degree programs
3. Support the Academic Program Approval Committee in
reviewing AMTA approved academic programs that are reapplying for AMTA program
approval, as well as new programs applying for initial approval
4. Provide information for government relations work dealing
with state licensures and employment practices (e.g., job descriptions,
salaries, populations, scope of practice).
5. Support efforts in seeking reimbursement and financing of
MT services
6. Support public relations efforts in professional
recognition and perception of music therapy by other professions and the public
7. Support efforts in continuing education by providing a
framework for defining what constitutes specialized trainings, advanced
trainings, and other types of continuing education opportunities
8. Provide a basis for developing advanced professional
designations and/or credentials
9. Support research efforts in music therapy
10. Stimulate continued growth of music therapists and the
profession
In November 2004 the Advisory
Board began its deliberations on defining levels of practice, which continued
through a mid-year retreat in July 2005. Following the retreat, the Advisory
Board issued the following Advisory on Levels of Practice for consideration by
the AMTA Board of Directors, Assembly of Delegates, Regions, and membership.
(back
to content)
4.21 Alexander Technique Science w
Peer-reviewed Research on Mind, Movement, and Posture
A Short History of AT
THE TEACHING OF F.M. ALEXANDER
The history of the Alexander
Technique extends back more than a century. Frederick Matthias Alexander
(1869�1955) began his teaching career as an elocutionist in Melbourne in the 1890s.
Over the course of several decades, he developed the method that bears his
name�a general approach to changing habits of postural support, muscle tension,
movement, attention, and reactivity. Alexander moved to Sydney in 1900, then
London in 1904. At the onset of World War I, he moved his practice to New York
City, where he taught off-and-on until returning to London full time in 1924.
He opened the first training course for teachers in London in 1931. During
World War II, he moved the training course to America. He resumed training
teachers in London in 1945 and taught until shortly before he died in 1955.
(Evans, 2001; Bloch, 2004; Staring, 2005; Murray, 2015). The Alexander
Technique has continued to evolve in the decades since his death.
ELOCUTION
As a young man, Alexander was a
teacher of elocution�also called voice culture�and a performer of �elocutionary
recitals� involving poetry, soliloquies, and short dramatic scenes (Damousi,
2010). In the days before amplification, elocution lessons were of interest not
only to actors and singers, but to barristers, clergymen, teachers, and
politicians (Kofler, 1889; Kirkpatrick, 2006). Voice culture was considered a
branch of the larger physical culture (physical education) movement (Mullan,
2012), and doctors sent patients to elocutionists for aid in respiratory health
(Leeper, 1909/2015). Alexander�s earliest pamphlets (1894, 1895 & 1900)
lean heavily on the works of nineteenth-century authorities on breath and
voice, including Thomas P. Hill, Nicholas Hartley, Leo Kofler, and Emil Behnke
and Lennox Browne. He taught breath gymnastics (exercises) and voice production
(Alexander, 1900; Anonymous, 1904). Alexander appears to have been quite
successful. As early as 1896, he received referrals and testimonials from a
network of doctors (Staring, 2005; Alexander, 1900). He would attract the
support of doctors throughout his career (Bloch, 2004; Murray, 2015).
DEVELOPMENT OF ALEXANDER�S TECHNIQUE
Alexander�s method changed
gradually over time, through self-study provoked by persistent problems with
his voice in performance (Alexander, 1907/1995; 1932/1985), through working
with his brother, Albert Redden (A.R.) (Staring, 2005, p. 354, fn 343), and
through his teaching experience (Bloch, 2004). He also explored other methods,
such as the Delsarte System of Dramatic Expression (McLeod, 2017) and a variety
of physical culture systems, including Sandow bodybuilding (Alexander,
1925/1995; McLeod, 2017). Though his method likely changed substantially from
his early days as an elocutionist, Alexander retained a lifelong interest in
breath coordination (1923/2004; Rengstorff, 2015).
Alexander�s work likely resembled
modern Alexander Technique teaching by 1914 (Murray). He began using positions
and movements that challenged postural coordination, such as �positions of
mechanical advantage� (for example, a semi-squat) and functional movement such
as sit-to-stand (1918/1995). At the same time, Alexander rejected common
understandings of posture� including the idea of posture as a correct position,
or that exercise was required to improve posture (1923/2004). Just as
importantly, Alexander became focused on how habit challenged self-control and
distorted self-perception. In lessons, a student�s foremost responsibility
became the �inhibition� of habits, not the assumption of a correct position or
the performance of a correct action. An overarching goal of a course of study
was to improve the accuracy of the student�s body awareness�or �sensory
appreciation� (1908/1995). To this end, Alexander developed a sophisticated and
subtle use of his hands in teaching to clarify the intended coordination
through sensory feedback and guided movement (1908/1995; Jones, 1976). For
example, when working with sitting and standing, he would guide the student in
and out of the chair.
By the 1920s, Alexander had
developed a reputation as a remarkable practitioner and students particularly
noted his hands-on skill. James Harvey Robinson, a professor of history at
Columbia University, wrote in 1918 that Alexander �literally remodels the
patient�all quite gently and persuasively� (Alexander, 1918/1996). The minister
and author, Gerald Lee, gave a flowery account of lessons with Alexander in
1920: �When you have removed all obstructions and preconceptions in your own
mind�and will stop preventing him from doing it, he places your body in an
entirely new position and subjects you to a physical experience in sitting,
standing, and walking, you have never dreamed you could have before� (1920).
Andrew Rugg-Gunn, a doctor who supported Alexander�s practice for several
decades starting in 1913, commented on Alexander�s skill in �palpation� and
felt that Alexander�s �insight into the living body had the quality of genius�
(2002). And Moshe Feldenkrais, founder of the Feldenkrais method, told Mia
Segal that Alexander �had the best hands he had ever felt� (Murray, 2011).
INTELLECTUAL INFLUENCES
Alexander�s work shows the
influence of many of the intellectual currents of his day. In his first two
books, Man�s Supreme Inheritance (1910/1918) and Constructive Conscious Control
of the Individual (1923), he places his technique within a larger vision of
mankind�s evolution towards greater consciousness, indebted to Neo-Lamarckian
thinkers like Herbert Spencer (1918/1996; 1923/2004). Such Neo-Lamarckian
ideas�that acquired habits could be passed on to subsequent generations� were
common in educational and physical culture systems of the time (Fallace, 2011;
Singleton, 2010). Alexander was also influenced by the new sciences of psychology
and neuroscience, including William James� writings on volition and �ideomotor
action� (Murray; Lamont, 1959) and Charles Sherrington�s research on reflex
action, kinesthesia, and inhibition in the nervous system (1906/1995;
1908/1995). In New York City during World War I, Alexander taught the prominent
pragmatist philosopher, John Dewey, who became an enthusiastic advocate of
Alexander�s work and a significant influence over the next twenty years,
especially in the writing of Constructive Conscious Control of the Individual
and Alexander�s third book, The Use of the Self (Williamson, 2016; Murray,
2015).
THE PRIMARY CONTROL
In the 1920s, Alexander became
familiar with the German physiologist Rudolf Magnus� research positing reflex
control of posture in animals (Bloch, 2004). Magnus� conclusions about the role
of head position and neck reflexes on posture�or more accurately, Alexander and
his doctor supporters� mistranslation and misappropriation of Magnus� German
text�would influence Alexander�s coinage of the �primary control� (Douglas,
1950/2015; Fischer, 2019). The term primary control is used to describe both a
postural relationship�the head, neck, and back�and also a pedagogical practice:
Alexander taught students to consciously prevent interference with the �primary
control� to bring about uninstructed and unconscious improvements in posture,
movement, and reactivity. The reflex models of posture proposed by Magnus and
Sherrington provided the neurophysiological mechanisms that teachers would use
to explain the Technique for decades to come: one learns to inhibit learned
habits in order to restore reflex control of posture (Jones, 1976/2003; Gelb,
1981/1994; Miller & Langstroth, 2007; Walker, 2008; Dimon, 2014).
TRAINING COURSE FOR TEACHERS
In 1931, Alexander opened the
first training course for teachers (Westfeldt, 1964/1998; Bloch, 2004). �First
generation� teachers are particularly esteemed in the profession for their
direct knowledge of Alexander�s work. The three year model for training Alexander
established is still the basis of traditional teacher training today. Alexander
moved the training course to America during World War II, training teachers
outside Boston, MA, and Philadelphia, PA. Alexander suffered a stroke in fall
1947, and his teaching assistants took over most of the duties of the training
course while he recovered. He resumed teaching by the following spring. His
teaching assistant, Walter Carrington, took on many of the duties of training
around 1952 and continued the training course after Alexander�s death.
(Carrington & Casey, 1986). Two short films were made of Alexander in 1949
and 1950, with footage of him both demonstrating chair work as well as his own
agility in old age.
MID-CENTURY SCIENTIFIC RESEARCH
Two first generation teachers
worked to establish the medical or scientific credentials of the Alexander
Technique at midcentury. Wilfred Barlow was a medical doctor who trained with
Alexander in the 1930s. While he attempted small studies with army cadets
during World War II and vocalists at the Royal College of Music (RCM) in the
early 1950s (Barlow, 2014), his work arguably had its biggest impact in the
performing arts with the inclusion of the Alexander Technique in the curriculum
at the RCM. Frank Pierce Jones trained with Alexander and his brother, A.R., in
the U.S. during World War II and did the first laboratory research on the
Alexander Technique in the 1950s and 1960s at Tufts University. Jones published
a number of papers on the Alexander Technique, including research on postural
set and the first study in the literature on sit-to-stand. (Jones, 1998) For a
variety of reasons, Jones� research was not widely cited. Following Magnus and
Sherrington, Jones posited reflex explanations for AT phenomena. Jones felt constrained
by behaviorism, the dominant model of psychology in the United States during
this period. Strict behaviorism rejected the study of internal mental states
and Jones expressed relief when concepts such as �awareness� become
scientifically respectable again in the 1960s (1998). Study of the Alexander
Technique also pushed against the limits of technology, as many of the most
interesting aspects of the Alexander Technique, such as body schema and
postural tone, were not measurable in the laboratory. This may explain why
there was next to no 12 significant research on the Alexander Technique until
the 1990s.
DECLINE AND RENEWAL
After Alexander�s death in 1955,
interest in his method declined (Bloch, 2004; Gounaris, 2017). Renewal began in
the performing arts, with the Alexander Technique offered at the Royal College
of Music in the 1950s and the Juilliard School in New York City in the 1960s
(Barlow, 1978; Kleinman & Buckoke, 2014; Leibowitz & Connington, 1990).
Since that time, the Alexander Technique has become a regular offering in
performing arts schools internationally, and many performing artists have
trained as Alexander teachers. Interest in the Alexander Technique also grew
with the Human Potential Movement in the 1960s and 1970s, when people turned to
many Eastern and Western practices in the search for personal growth,
awareness, and enlightenment (Caldwell, 1975; Blanc, 2005). Perhaps the most
important single event in the growth of the Alexander Technique after
Alexander�s death was Nikolaas Tinbergen�s unexpected advocacy of the Alexander
Technique in his Nobel Prize speech in 1973. Though his address was
controversial among scientists and even among Alexander teachers, the publicity
led to a surge of interest in the Technique (Bloch, 2004; Lewin, 1974;
Cacciatore, 2000; Murray, 2015).
TRAINING COURSES AND PROFESSIONAL SOCIETIES
The Alexander Technique spread
first to the United States and Europe, with significant interest in Israel
beginning in the 1950s. The most influential of first generation Alexander
teachers were those who ran training courses, notably Walter Carrington,
Patrick Macdonald, Marjory and Bill Barlow, among others. Marjory Barstow was
another influential first generation teacher. Though Barstow did not run a
training course, she did work with a number of teachers in what has been
described as an apprentice-style training beginning in the 1970s (Conable,
1988/2016). The Society for Teachers of the Alexander Technique (STAT) was
founded in 1958. In the 1960s, STAT formally established a three-year training
standard, which by the end of the decade was codified as 1600 hours of
instruction time to qualify as a STAT-certified teacher (Fitzgerald, 2007). By
the 1980s, STAT was overseeing training programs internationally, and so affiliated
societies were formed, now numbering eighteen societies across the world. The
formation of the North American Society for Teachers of the Alexander Technique
in 1987 (now AmSAT�the American Society for the Alexander Technique) led to a
dispute on the membership of students who had trained outside the STAT model.
In 1992, an alternative society, Alexander Technique International was formed
(ATI History, 2019). Mouritz Press has recently begun compiling information
about the history of training courses and has identified approximately 185
teachers worldwide who have run training courses over the past 65 years
(Fischer, 2019a).
DEVELOPMENTS IN PEDAGOGY
Since Alexander�s time, there has
been an expansion in the teaching procedures used in lessons. F.M. Alexander
taught almost exclusively using procedures around sitting and standing
(referred to as chair work) and lying down (called table work). Alexander�s
teaching assistant, Irene Tasker, is often credited with developing what is
sometimes called �application� or �activity� work, in which the lesson is
centered on applying the Technique to an everyday activity (Evans, 2001;
Hunter, 2013). Activity work is widely used by modern Alexander teachers, and
some teachers specialize in particular activities, such as running (Balk &
Shields, 2006), swimming (Shaw & D�Angour, 2001), dance (Nettl-Fiol &
Vanier, 2011), or pregnancy and childbirth (Machover & Drake, 1993). Even
teachers who focus almost exclusively on Alexander�s classic procedures will often
include time in lessons for applying the Technique to a specific activity, for
example, playing a musical instrument (Carrington, 1986).
Other approaches to teaching the
Alexander Technique may be less widespread. Some teachers use developmental
movement to clarify aspects of the Alexander Technique, an approach first
explored in the late 1960s by graduates of Walter Carrington�s training course,
Joan and Alexander Murray, in collaboration with the neuroanatomist and
anthropologist, Raymond Dart (Goldberg, 1996). Traditional AT lessons are
delivered one-to-one, with near-constant interaction and personalized feedback.
Teaching in groups is associated with Marjory Barstow, who began teaching in
groups of 60 or more in the 1970s. While most Alexander technique teachers will
teach AT in group settings such as an introductory workshops, some Alexander
teachers now teach almost exclusively in a group setting. Body mapping, an
anatomy-based retraining of awareness, was developed by William and Barbara
Conable, two students of Marjory Barstow. The most recent teacher
experimentation involves distance learning, such as online lessons, in which
traditional hands-on guidance is impossible. Such experiments have been seen by
some Alexander teachers as a refreshing liberation from perceived Alexander
Technique dogma. Others have seen these practices as a dilution or even a
distortion of the Alexander Technique.
SCIENTIFIC RESEARCH IN THE 21ST-CENTURY
Perhaps the most notable
development in the new century is the growing body of scientific research
establishing some of the benefits of Alexander lessons and investigating
plausible mechanisms for such benefits. Modern scientific models are much more
relevant to the Alexander Technique than the reflex models of posture available
to F.M. Alexander. Research has started to identify some of the
neurophysiological changes associated with Alexander lessons and teacher
training�including increased adaptability of postural tone (Cacciatore, et al,
2011), changes in movement coordination possibly linked to adaptability of
postural control (Cacciatore et al, 2014), reduced muscular co-contraction
(Preece, et al, 2015), and possible changes of coordination from superficial to
deeper musculature (Becker, et al, 2018). There is also intriguing research
linking changes in body schema with functional improvements during movement
learning, or dysfunction, as with chronic pain or focal dystonia (Bray &
Moseley, 2011; Byl et al, 1997). Randomized controlled trials have found
significant benefits of AT for individuals with Parkinson�s disease
(Stallibrass, et al, 2002), low back pain (Little, et al, 2008), and neck pain
(MacPherson, et al, 2015). Such research is likely to make it easier for
Alexander teachers to make connections with the medical profession.� Historically, the Alexander profession has
often struggled to reconcile tradition and innovation and to establish the
boundaries of what practices are acceptable as the Alexander Technique. As the
subtleties of the Technique become measurable outside the lesson, Alexander
teachers may be able to find connections between the different traditions
within the Technique�s long history, as well as finding more ways of connecting
with other professions and the wider public.
Author: Andrew McCann is a regular contributor to Alexander
Technique Science. He teaches the Alexander Technique in Chicago.
(back
to content)
4.22
Apitherapy w
Apitherapy is a branch of
alternative medicine that uses honey bee products, including honey, pollen,
propolis, royal jelly and bee venom. There is no good clinical evidence for the
efficacy or safety of apitherapy treatments.
References to possible medical
properties of bee products can be found in Chinese, Korean, Russian, Egyptian
and Greek traditional medicine practices. Apitherapy has been practiced since
the times of Hippocrates and Galen. Modern use of bee venom appears to have
originated with Austrian physician Philipp Terč and his 1888 article
"About a Peculiar Connection
Bee sting being applied during an apitherapy session.
HISTORY
Between the Bee Stings and
Rheumatism", but his claims were never tested in proper clinical trials.
More recent alternative medicine practice is attributed to the Hungarian
physician Bodog F. Beck who coined the term "bee venom therapy" in
1935, and to beekeeper Charles Mraz (1905�1999) in the latter half of the
twentieth century. In 1957, the USSR Ministry of Health sanctioned use of bee
venom to treat certain ailments by approval of Nikolay Artemov's
"Instruction for Bee Sting Venom Apitherapy".
Humans have historically used bee
products in various ways: beeswax was used in casting metals and making
incendiary weapons, honey was used for food and religious offerings, propolis
was used as an adhesive, and pollen was used for agricultural work such as plant
breeding. Much later, there was an attempt to use bee venom clinically via
injection by J.
Langer at the University of
Prague in late 1890s and in 1930, a firm in south Germany named Mack produced
bee venom solution commercially. Apitherapy is used in traditional medicine in
countries in Europe, Asia, and South America including China, Korea, and
Russia.
Apitherapy is promoted as
alternative medicine for several uses, but its health claims are not supported
by scientific evidence. Bee venom or other honeybee products are ineffective
for the treatment or prevention of cancer. In general, evidence for using honey
in wound treatment is of such low quality that firm conclusions cannot be
drawn.
Adverse reactions to bee venom
therapy are frequent. Frequent exposure to the venom can also lead to
arthropathy. In sensitized persons, venom compounds can act as allergens,
causing a spectrum of allergic reactions that can range from mild, local
swelling to severe systemic reactions, anaphylactic shock, or even death.
In March 2018 it was reported
that a 55-year-old woman died after receiving "live bee acupuncture",
suffering a severe anaphylactic episode which the apitherapy practitioner did
not respond to by administering adrenaline. While stabilized by ambulance
personnel on the way to the hospital, she died a few weeks later from
complications resulting in multiple organ failure.
Live bee acupuncture therapy is
"unsafe and unadvisable", according to researchers who studied the
case.
(back
to content)
Aquatic
therapy w
Aquatic therapy refers to
treatments and exercises performed in water for relaxation, fitness, physical
rehabilitation, and other therapeutic benefit. Typically, a qualified aquatic
therapist gives constant attendance to a person receiving treatment in a heated
therapy pool. Aquatic therapy techniques include Ai Chi, Aqua Running, Bad
Ragaz Ring Method, Burdenko Method, Halliwick, Watsu, and other aquatic
bodywork forms. Therapeutic applications include neurological disorders, spine
pain, musculoskeletal pain, postoperative orthopedic rehabilitation, pediatric
disabilities, and pressure ulcers.
Aquatic therapy refers to
water-based treatments or exercises of therapeutic intent, in particular for
relaxation, fitness, and physical rehabilitation. Treatments and exercises are
performed while floating, partially submerged, or fully submerged in water.
Many aquatic therapy procedures require constant attendance by a trained
therapist, and are performed in a specialized temperature-controlled pool.
Rehabilitation commonly focuses on improving the physical function associated
with illness, injury, or disability.
OVERVIEW
Aquatic therapy encompasses a
broad set of approaches and techniques, including aquatic exercise, physical
therapy, aquatic bodywork, and other movement-based therapy in water
(hydrokinesiotherapy). Treatment may be passive, involving a therapist or giver
and a patient or receiver, or active, involving self-generated body positions,
movement, or exercise. Examples include Halliwick Aquatic Therapy, Bad Ragaz Ring
Method, Watsu, and Ai chi.
For orthopedic rehabilitation,
aquatic therapy is considered to be synonymous with therapeutic aquatic
exercise, aqua therapy, aquatic rehabilitation, water therapy, and pool
therapy. Aquatic therapy can support restoration of function for many areas of
orthopedics, including sports medicine, work conditioning, joint arthroplasty,
and back rehabilitation programs. A strong aquatic component is especially
beneficial for therapy programs where limited or non-weight bearing is
desirable and where normal functioning is limited by inflammation, pain,
guarding, muscle spasm, and limited range of motion (ROM). Water provides a
controllable environment for reeducation of weak muscles and skill development
for neurological and neuromuscular impairment, acute orthopedic or
neuromuscular injury, rheumatological disease, or recovery from recent surgery.
Various properties of water
contribute to therapeutic effects, including the ability to use water for
resistance in place of gravity or weights; thermal stability that permits
maintenance of near constant temperature; hydrostatic pressure that supports
and stabilizes, and that influences heart and lung function; buoyancy that
permits flotation and reduces the effects of gravity; and turbulence and wave
propagation that allow gentle manipulation and movement.
The use of water for therapeutic
purposes first dates back to 2400 B.C. in the form of hydrotherapy, with
records suggesting that ancient Egyptian, Assyrian, and Mohammedan cultures
utilized mineral waters which were thought to have curative properties through
the 18th century.
In 1911, Dr. Charles Leroy Lowman
began to use therapeutic tubs to treat cerebral palsy and spastic patients in
California at Orthopedic Hospital in Los Angeles. Lowman was inspired after a
visit to Spaulding School for Crippled Children in Chicago, where wooden
exercise tanks were used by paralyzed patients. The invention of the Hubbard
Tank, developed by Leroy Hubbard, launched the evolution of modern aquatic
therapy and the development of modern techniques including the Halliwick
Concept and the Bad Ragaz Ring Method (BRRM). Throughout the 1930s, research
and literature on aquatic exercise, pool treatment, and spa therapy began to
History appear in professional journals. Dr. Charles Leroy Lowman's Technique
of Underwater Gymnastics: A Study in Practical Application, published in 1937,
introduced underwater exercises that were used to help restore muscle function
lost by bodily deformities. The National Foundation for Infantile Paralysis
began utilizing corrective swimming pools and Lowman's techniques for treatment
of poliomyelitis in the 1950s.
The American Physical Therapy
Association (APTA) recognized the aquatic therapy section within the APTA in
1992, after a vote within the House of Delegates of the APTA in Denver, CO
after lobbying efforts spearheaded starting in 1989 by Judy Cirullo and Richard
C. Ruoti.
Techniques for aquatic therapy include the following:
Ai Chi: Ai Chi, developed in 1993
by Jun Konno, uses diaphragmatic breathing and active progressive resistance
training in water to relax and strengthen the body, based on elements of qigong
and Tai chi chuan.
Aqua running: Aqua running (Deep
Water Running or Aquajogging) is a form of cardiovascular conditioning,
involving running or jogging in water, useful for injured athletes and those
who desire a low-impact aerobic workout. Aqua running is performed in deep
water using a floatation device (vest or belt) to support the head above water.
Bad Ragaz Ring Method: The Bad
Ragaz Ring Method (BRRM) focuses on rehabilitation of neuromuscular function
using patterns of therapist-assisted exercise performed while the patient lies
horizontal in water, with support provided by rings or floats around the neck,
arms, pelvis, and knees. BRRM is an aquatic version of Proprioceptive
Neuromuscular Facilitation (PNF) developed by physiotherapists at Bad Ragaz,
Switzerland, as a synthesis of aquatic exercises designed by a German physician
in the 1930s and land-based PNF developed by American physiotherapists in the
1950s and 1960s.
Burdenko Method: The Burdenko
Method, originally developed by Soviet professor of sports medicine Igor
Burdenko, is an integrated land-water therapy approach that develops balance,
coordination, flexibility, endurance, speed, and strength using the same
methods as professional athletes. The water-based therapy uses buoyant
equipment to challenge the center of buoyancy in vertical positions, exercising
with movement in multiple directions, and at multiple speeds ranging from slow
to fast.
TECHNIQUES
Halliwick Concept: The Halliwick
Concept, originally developed by fluid mechanics engineer James McMillan in the
late 1940s and 1950s at the Halliwick School for Girls with Disabilities in
London, focuses on biophysical principles of motor control in water, in
particular developing sense of balance (equilibrioception) and core stability.
The Halliwick Ten-Point-Program implements the concept in a progressive program
of mental adjustment, disengagement, and development of motor control, with an
emphasis on rotational control, and applies the program to teach physically
disabled people balance control, swimming, and independence.
Halliwick Aquatic Therapy (also
known as Water Specific Therapy, WST), implements the concept in
patient-specific aquatic therapy.
Watsu: Watsu is a form of aquatic
bodywork, originally developed in the early 1980s by Harold Dull at Harbin Hot
Springs, California, in which an aquatic therapist continuously supports and
guides the person receiving treatment through a series of flowing movements and
stretches that induce deep relaxation and provide therapeutic benefit. In the
late 1980s and early 1990s physiotherapists began to use Watsu for a wide range
of orthopedic and neurologic conditions, and to adapt the techniques for use
with injury and disability.
Applications of aquatic therapy
include neurological disorders, spine pain, musculoskeletal pain, postoperative
orthopedic rehabilitation, pediatric disabilities, and pressure ulcers.
A 2006 systematic review of
effects of aquatic interventions in children with neuromotor impairments found
"substantial lack of evidence-based research evaluating the specific
effects of aquatic interventions in this population".
For musculoskeletal
rehabilitation, aquatic therapy is typically used to treat acute injuries as
well as subjective pain of chronic conditions, such as arthritis. Water
immersion has compressive effects and reflexively regulates blood vessel tone.
Muscle blood flow increases by about 225% during immersion, as increased
cardiac output is distributed to skin and muscle tissue.
Flotation is able to counteract
the effects of gravitational force on joints, creating a low impact environment
for joints to perform within. The temperature changes, increase in systolic
blood pressure to extremities, and overall increase in ambulation are factors
which help immersion to alleviate pain. Aquatic Therapy helps with pain and
stiffness, but can also improve quality of life, tone the muscles in the body,
and can help with movement in the knees and hips. Protocols using a combination
of strengthening, flexibility, and balance exercises resulted in the greatest
improvements in Childhood Health Assessment Questionnaire scores, whereas aerobic
exercise did not result in greater improvements in CHAQ scores compared to a
comparison group
Applications and effectiveness
performing Qigong. Not only does aquatic therapy help with pain, but can
benefit postural stability, meaning it can help to strengthen balance functions
especially with people who have neurological disorders. For people diagnosed
with Parkinson's disease, aquatic exercise has been proven to be more
beneficial than land-based exercise for two important outcome measures. The Berg
Balance Scale and Falls Efficacy Scale score were reported to have significant
improvement when implementing aquatic exercise over land-based exercise. These
results suggest that aquatic exercise can be extremely helpful for Parkinson's
disease patients with specific balance disorders and fear of falling.
Aquatic therapy in warm water has
been shown to have a positive effect on the aerobic apacity of people with
fibromyalgia. It is still inconclusive whether land therapy is better than
aquatic therapy however it has been demonstrated that aquatic therapy is as
effective as land base therapy. There are advantageous outcomes for patients
with fibromyalgia resulting from aquatic therapy such as decrease of articulate
load regarding an individual's biomechanics.
Currently there is no
standardized aquatic therapy protocol for people post stroke however it is safe
to conclude that aquatic therapy can be more effective than land based therapy
for improving balance and mobility. There is insufficient evidence regarding
improvements in functional independence of people post stroke.
From a cardiopulmonary
standpoint, aquatic therapy is often used because its effects mirror land-based
effects but at lower speeds. During immersion, blood is displaced upwards into
heart and there is an increase in pulse pressure due to increased cardiac
filling. Cardiac volume increases 27-30%. Oxygen consumption is increased with
exercise, and heart rate is increased at higher temperatures, and decreased at
lower temperatures. However, immersion can worsen effects in cases of valvular
insufficiency due to this cardiac and stroke volume increase. The aquatic
environment is also not recommended for those who experience severe or
uncontrolled heart failure.
Aquatic therapy is performed by
diverse professionals with specific training and certification requirements. An
aquatic therapy specialization is an add-on certification for healthcare
providers, mainly including physical therapists and athletic trainers.
For medical purposes, aquatic
therapy, as defined by the American Medical Association (AMA), can be performed
by various legally-regulated healthcare professionals who have scopes of Professional
training and certification practice that permit them to offer such services and
who are permitted to use AMA Current Procedural Terminology (CPT) codes.
Currently, aquatic therapy certification is provided by the Aquatic Therapy and
Rehab Institute (ATRI), which aims to further education for therapists and
healthcare professionals working in aquatic environments. The ATRI
prerequisites for certification include 15 hours of Aquatic Therapy, Rehab
and/or Aquatic Therapeutic Exercise education, which can be completed hands-on
or online. Once completing the prerequisites, those pursuing certification can take
the Aquatic Therapy & Rehab Institutes Aquatic Therapeutic Exercise
Certification exam.
(back
to content)
4.24
Bibliotherapy w
Bibliotherapy (also referred to
as book therapy, reading therapy, poetry therapy or therapeutic storytelling)
is a creative arts therapies modality that involves storytelling or the reading
of specific texts. It uses an individual's relationship to the content of books
and poetry and other written words as therapy. Bibliotherapy has some overlap with
writing therapy and is often combined with writing therapy.
Distinct from the creative arts
therapy is bibliotherapy as a supportive psychotherapy, a brief self-help
intervention where through the reading of a chosen standard manual, emotion
regulation skills are acquired through either behavioral therapy or cognitive
therapy techniques. Two popular books used for this are The Feeling Good
Handbook for cognitive therapy and Control Your Depression for behavioral
therapy. The main advantages of this psychotherapy compared to cognitive
behavioral therapy (CBT) is its cost-effectiveness, although, especially for
complex presentations, CBT tends to have more positive treatment outcomes. It
has been shown to be effective in the treatment of mild to moderate depression,
with cognitive bibliotherapy having a long-lasting effect. Modest evidence also
exists to the symptom reduction of alcohol dependence, self-harm and panic
disorder.
BIBLIOTHERAPY
Unstructured and more informal
bibliotherapy fits under creative arts therapies, possibly including reading or
activity recommendations by a librarian or health professional based on
perceived therapeutic value. More structured bibliotherapy can be described as
supportive psychotherapy, where more consideration is placed on the therapist
to the selection of reading material and in including other activities to
facilitate skill acquisition and symptom reduction.
An important difference between
the two is the greater empirical support of symptom reduction in bibliotherapy as
a supportive psychotherapy.
Bibliotherapy is an old concept
in library science. According to the Greek historian Diodorus Siculus, in his
monumental work Bibliotheca historica, there was a phrase above the entrance to
the royal chamber where books were stored by King Ramses II of Egypt.
Considered to be the oldest known library motto in the world, ψῡχῆς
ἰατρεῖον on, is translated: "the
house of healing for the soul". Galen, the extraordinary philosopher and
physician to Marcus Aurelius of Rome, maintained a medical library in the first
century A.D., used not only by himself but by the staff of the Sanctuary
Asclepion, a Roman spa famous for its therapeutic waters and considered to be
one of the first hospital centers in the world. As far back as 1272, the Koran
was prescribed reading in the Al-Mansur Hospital in Cairo as medical treatment.
In the early nineteenth century,
Benjamin Rush favored the use of literature in hospitals for both the
"amusement and instruction of patients". By the middle of the century,
Minson Galt II wrote on the uses of bibliotherapy in mental institutions, and
by 1900 libraries were an important part of European psychiatric institutions.
After the term bibliotherapy was
coined by Samuel McChord Crothers in an August 1916 Atlantic Monthly article,
it eventually found its way into the medical lexicon. During World War I, the
Library War Service stationed librarians in military hospitals, where they
dispensed books to patients and developed the emerging "science" of
bibliotherapy with hospital physicians. When they returned from the war, they
tried to implement these ideas in hospital libraries.
HISTORY
Kathleen Jones, the editor of the
book series Hospital Libraries, was the library administrator for the McLean
Hospital in Massachusetts. This influential work was first published in 1923,
and then updated in 1939, and then 1953. Pioneer librarian Sadie Peterson
Delaney used bibliotherapy in her work at the VA Hospital in Tuskegee, Alabama
from 1924 to her death in 1958. Elizabeth Pomeroy, director of the Veterans
Administration Library Service, published the results of her research in 1937
on the efficacy of bibliotherapy at VA hospitals. The United Kingdom, beginning
in the 1930s, also began to show growth in the use in of reading therapy in
hospital libraries. Charles Hagberg-Wright, librarian of the London Library,
speaking at the 1930 British Empire Red Cross Conference, spoke about the
importance of bibliotherapy as part of "curative medicine" in
hospitals. In addition, reports from the 1930 Public Health Conference about
bibliotherapy were included in the British journal Lancet. By the 1920s, there
were also training programs in bibliotherapy. One of the first to offer such
training was the School of
Library Science at Western Reserve
University followed by a program at the University of Minnesota School of
Medicine.
With hospitals taking the lead,
bibliotherapy principles and practice developed in the United States. In the
United Kingdom some felt that bibliotherapy lagged behind the US and Joyce
Coates, writing in the Library Association Record, felt that "the
possibilities of bibliotherapy have yet to be fully explored". In 1966,
the Association of Hospital and Institution Libraries, a division of the
American Library Association, issued a working definition of bibliotherapy in
recognition of its growing influence. Then, in the 1970s, Arleen McCarty Hynes,
a proponent for the use of bibliotherapy, created the "Bibliotherapy Round
Table" which sponsored lectures and publication dedicated to the practice.
In its most basic form,
bibliotherapy is using books to aid people in solving the issues that they may be
facing at a particular time. It consists of selecting reading material relevant
to a client's life situation. Bibliotherapy has also been explained as "a
process of dynamic interaction between the personality of the reader and
literature - interaction which may be utilized for personal assessment,
adjustment, and growth." Bibliotherapy for adults is a form of
self-administered treatment in which structured materials provide a means to
alleviate distress.
The concept of the treatment is
based on the human inclination to identify with others through their
expressions in literature and art. For instance, a grieving child who reads, or
is read a story about another child who has lost a parent may feel less alone
in the world. The concept of bibliotherapy has widened over time, to include
self-help manuals without therapeutic intervention, or a therapist
"prescribing" a movie that might provide needed catharsis to a
client.
The Online Dictionary for Library and Information Science
(2011) defines bibliotherapy as:
Changing definitions: The use of
books selected on the basis of content in a planned reading program designed to
facilitate the recovery of patients suffering from mental illness or emotional
disturbance. Ideally, the process occurs in three phases: personal
identification of the reader with a particular character in the recommended
work, resulting in psychological catharsis, which leads to rational insight
concerning the relevance of the solution suggested in the text to the reader's
own experience.
Assistance of a trained psychotherapist is advised.
Although the term
"bibliotherapy" was first coined by Samuel Crothers in 1916, the use
of books to change behavior and to reduce distress has a long history, dating
back to the Middle Ages.
When applied in a therapeutic
context, bibliotherapy can comprise both fictional and nonfictional materials.
Fictional bibliotherapy (e.g., novels, poetry) is a dynamic process, where
material is actively interpreted in light of the reader's circumstances. From a
psychodynamic perspective, fictional materials are believed to be effective
through the processes of identification, catharsis and insight. Through
identification with a character in the story the reader gains an alternative
position from which to view their own issues. By empathizing with the character
the client undergoes a form of catharsis through gaining hope and releasing
emotional tension, which consequently leads to insights and behavioral change.
Working with an imaginative journey and a specific selection of metaphors,
proponents claim that a therapeutic story approach has the potential to shift
an out of balance behavior or situation back towards wholeness or balance. A
patient might also find it easier to talk about his issues if he and the
therapist can pretend that they are talking about the character's issues.
Proponents suggest that the story form offers a healing medium that allows the
listener to embark on an imaginative journey, rather than being lectured or
directly addressed about the issue.
In the 1980s and early 1990s,
bibliotherapy was a widely used but poorly researched therapeutic model.
However, numerous randomized controlled trials (RCTs) have documented the
positive effects of bibliotherapy for clinical conditions such as deliberate
self-harm, obsessive�compulsive disorder (OCD) and bulimia nervosa and
insomnia. Research also supports bibliotherapy as an intervention for a wide
array of psychological issues including emotional disorders, alcohol addiction,
and sexual dysfunction. In a recent review of psychotherapeutic treatments for
older depressed people, bibliotherapy emerged as an effective intervention.
CLINICAL USE
The use of bibliotherapy in
mental health programs, including those for substance abuse, has been shown to
be beneficial to patients in the United Kingdom where it is a popular resource.
Researchers have found that
bibliotherapy can successfully complement treatment programs and reduce
recidivism.
In the United States a researcher
from the University of South Florida published a study seeking to revise the
collection development policy for a bibliotherapy library used by the residents
at a women's AOD treatment center in Tampa, Florida. The research was conducted
by Peter Cannon as part of his PhD on rhetoric and reading therapies.
Preliminary findings suggest this new model can offer the residents a new
bibliotherapy track that employs less emotionally triggering texts that will be
useful for treatment.
Bibliotherapy can be performed
using affective treatment techniques, cognitive behavioral therapy (CBT), and
visual-based materials. Affective bibliotherapy relies upon fiction which can
aid participants. By empathizing with a story's character, the client undergoes
a form of catharsis by gaining hope and releasing emotional tension. There can
also be a connection made between the circumstances in a story and the reader's
own personal issues. This, consequently, leads to insights and behavioral
change. Bibliotherapy using CBT relies mainly on self-help books which work to
correct negative behaviors by offering alternative, positive actions.
Visual-based materials, such as graphic novels, utilize both affective and CBT
techniques.
COGNITIVE TREATMENT
The gains achieved in cognitive
bibliotherapy illustrate that the most important element in cognitive
bibliotherapy is content of the program and not the individual interactions
with a therapist. Bibliotherapy using CBT have been empirically tested the most
and directed CBT appears to be the most prevalent methodology in the
literature. The selection of CBT books is important since there are many on the
market that purport to help. Pardeck's analysis on choosing books is quite
instructive and much of his criteria mirror what librarians teach in
information literacy. These include the authority of the author on the topic,
the type of empirical support offered for treatment claims, the existence of
studies testing its clinical efficacy, and a comparative review of other books.
TREATMENT TRACKS
AFFECTIVE TREATMENT
There is not as much research on
using fiction in bibliotherapy when compared to cognitive self-help books. The
recent work of Shechtman has been important in investigating the use of
affective literature for bibliotherapy. In her work on counseling with
aggressive boys, Shechtman discusses the deficits these children exhibit and
describe affect disorders with symptoms of emotional arousal, low levels of
empathy, and difficulties in self-expression. Using integrative treatment
whereby the patient explores the problem, gains insight, and commits to change,
Shechtman found that using affective bibliotherapy techniques achieved
therapeutic change while indicating gains in empathy and insight.
VISUAL TREATMENT AND GRAPHIC NOVELS
In the simplest sense, graphic
novels are long-form comic books, usually 100 pages or more in length.
Application of graphic novels in this context will allow people struggling with
literacy to have better access to materials. Dozens of graphic novels have been
published over the last decade that address public health topics, such as
depression, drug abuse, and PTSD. Public health based comic books originated in
the 1940s. The earliest public health comics averaged around twelve pages and
were aimed at preventive instruction for children. Over the last fifteen years,
however, the genre has evolved and public health graphic novels and are now
commonly 150 pages long and focus more on adult struggles with physical or
mental illness. This change has gotten the attention of medical professionals
who gather and evaluate these materials. Currently, a group of physicians,
professors, artists, and bioethicists run the website Graphic Medicine and hosts
an annual conference to discuss the use of graphic novels and comic books in
health.
There is a wide range of research
that indicates graphic novels are an effective tool for people struggling with
literacy and communication problems. They also have been shown to be effective
with populations that have trouble with traditional literacy instruction.
Resistance to learning can take many forms, some of which can be seen in
populations involved with the criminal justice system. Graphic novels are most
often used to entice the group referred to as "reluctant readers",
people who have abandoned reading for pleasure. While this group may be
literate in the basic sense, research shows that people who read for pleasure
continuously improve vocabulary and language skills, skills that can help
people rehabilitate after incarceration. Research shows graphic novels are of
use to students with traditional learning disabilities, like dyslexia and also
have been shown to be effective when used in a bibliotherapeutic context to
assist people with mental illness in explaining their own struggles to others.
Graphic novels have also been described by professionals in the field as
especially apt for portraying the struggles associated with mental illness.
Bibliotherapy has been studied by
Jennie Bolitho (2011) in relationship to libraries, health and social
connection for the elderly. Bolitho set up a pilot reading program where she
read the text aloud to a group of participants at a local aged care hostel.
(She described "being read to as part of the nurturing experience".)
Her evaluation at the end of the 12-week program described all responses as
positive and participants commented that they "look forward to the group
as it made them think for themselves and gave them something to think about
aside from their ailments and the monotony of the day" (p. 90).
Bibliotherapy has not been vastly researched to ensure that
it will be successful for all students.
It has many drawbacks, that
include unavailable literature on certain topics that students may be
struggling with, many students not being ready to face their issues and read,
and students and parents defensively implementing the therapy. The resistance
of using bibliotherapy is based on a lack of assertiveness, negative attitudes,
anxiety, depression, sexual dysfunctions, and negative behaviors. There has
been advocacy for reading books containing difficult themes in advance, rather
than in response to a parent or teacher identifying a specific issue in a
child's life. The major issue that lies behind bibliotherapy is the lack of
research that has been conducted on this therapy device.
Advantages of bibliotherapy
include teaching students to solve problems, help students cope with teasing,
name calling, mockery, fears, sexuality changes, anxiety, and death. Despite
the limited research on bibliotherapy and its effects, many teachers have shown
improved achievement and self-concept.
Bibliotherapy can consist solely
of reading, or it can be complemented with discussion or play activity. A child
might be asked to draw a scene from the book or asked whether commonality is
felt with a particular character in the book. The book can be used to draw out
a child on a subject (s)he has been hesitant to discuss.
OLDER ADULTS
USE IN
CHILDREN'S THERAPY
IMPLEMENTATION
Of necessity, bibliotherapy
originally used existing texts. Literature that touched on the particular
subject relevant to the child provided the source material. (For example, Romeo
and Juliet is typically read in 8th or 9th grade as Romeo is 15 and Juliet is
13; students at that age can identify with them.) Recently it has become
possible to find texts targeted to the situation; e.g. many of The Berenstain
Bears books target particular behaviors and responses to certain situations.
Two forms of bibliotherapy exist:
clinical and developmental. Clinical bibliotherapy is solely used by qualified
personnel in a therapeutic setting and developmental bibliotherapy is a useful
tool to utilize before a problem arises. Developmental bibliotherapy can be
useful for issues such as nightmares as children age. Developmental
bibliotherapy is often used by teachers or parents, however, if an issue arises
that a teacher or parent cannot handle, clinical bibliotherapy is needed.
Many therapeutic stories are
written for specific individual needs, but practitioners have also used them to
build psychological resilience when group and communities face challenges. For
example, therapeutic storytelling can play a role in creating inclusive
classroom and work communities. Therapeutic stories are also sometimes referred
to as "healing stories". In the US, the National Storytelling Network
has a special interest group called the Healing Story Alliance.
Implementing bibliotherapy in an
elementary classroom can be very beneficial to both the students and the
teacher. Teachers who use bibliotherapy in their classroom also learn much about
the children they teach. Teachers as practitioners of bibliotherapy select
appropriate reading materials and match them to the needs of individual
students to assist them in the development of self-awareness, problem-solving
skills, perspective-taking, and understanding of problems. The materials may
include "any literacy activity, including reading (fiction, nonfiction, or
poetry), creative writing, or storytelling." Teachers that select
appropriate literature for their classroom needs may provide a child with a
"character in a story to help the child understand himself Classroom story
time and a guided discussion allows students to "become aware of problems
of other children and develop empathy".
In the article "Read two
books and write me in the morning", the authors highlight the fact that
teachers are an integral part of a student's therapeutic team. It is the
teacher who may be the first person to notice that something is troubling a
child. They also note that teachers have been In the classroom referred to as
carryover agents, who carry out recommendations from other professionals who
have suggested accommodations necessary to ensure a particular student's
well-being or success in their classroom. In inclusive classrooms the teacher
and the whole class play a role in meeting directly or indirectly, the needs of
students with exceptionalities. Bibliotherapy can help the students in the
class to learn coping skills that will help them deal with the social and
emotional challenges that may occur. Books and reading are an integral part of
classroom life. Through books, "children are able to see reflections of
themselves, their times, their country, their concerns... well-written
realistic fiction will always help readers gain a deeper understanding of
themselves and others."
Bibliotherapy has three recognized stages: (1)
identification, (2) catharsis, and (3) insight.
Identification is when a reader
associates themselves with the character or situation in the literary work.
Catharsis is when the reader shares many of the same thoughts and feelings of
the characters in the literary work, and insight is when the reader realizes
that they relate to the character or situation and learn to deal more
effectively with their own personal issues.
Literary pieces allow teachers to
identify for their class, or an individual student, a particular issue which
they are dealing with directly or indirectly. In a class with a special needs
student, for example, books featuring a character with the same needs will help
students experience living with a chronic condition; through a guided
discussion, they will able to verbalize their thoughts and concerns. This
exercise will offer insight into the issue of how to help their classmate
effectively. Bibliotherapy "does not prescribe meanings, nor is it a form
of direct teaching; it is more an invitation and permission giving to children
to unveil wisdom and insight that might otherwise be squelched."
Teachers who practice or need to
use bibliotherapy can find connections to their state or provincial guidelines.
A common challenge for classroom teachers is finding the right book, and
although some annotated bibliographies are available online and in curriculum
publications, not all issues are touched upon. A teacher may have to find their
book. The following evaluation framework is suggested:
"Is the story simple, clear,
brief, non repetitious, and believable? Is it at an appropriate reading level
and developmental level? Does the story fit with relevant feelings, needs,
interests, and goals? Does it demonstrate cultural diversity, gender
inclusivity, and sensitivity to aggression?
Do characters show coping skills and does the problem
situation show resolution?"
STAGES FOR TEACHERS
There are steps that make
bibliotherapy a more effective solution for dealing with the issues that a
student may be facing, including developing support, trust, and confidence with
the student with an issue, identifying other school personnel that could aid in
implementing the therapy, seeking support from the student's parents or
guardians, defining the issue that the student is facing and why the teacher
wants to help solve it, creating goals that may help the student overcome the
issue, researching books that may help with the specific problem, introducing
the book to all the people that will be involved, incorporating reading
activities, and evaluating the effects and successes that the book may have had
on the student.
(back
to content)
4.25 Chelation therapy w
Chelation therapy is a medical
procedure that involves the administration of chelating agents to remove heavy
metals from the body. Chelation therapy has a long history of use in clinical
toxicology and remains in use for some very specific medical treatments,
although it is administered under very careful medical supervision due to
various inherent risks, including the mobilization of mercury and other metals
through the brain and other parts of the body by the use of weak chelating
agents that unbind with metals before elimination, exacerbating existing damage.
To avoid mobilization, some practitioners of chelation use strong chelators,
such as selenium, taken at low doses over a long period of time.
CHELATION THERAPY
Chelation therapy must be
administered with care as it has a number of possible side effects, including
death. In response to increasing use of chelation therapy as alternative
medicine and in circumstances in which the therapy should not be used in
conventional medicine, various health organizations have confirmed that medical
evidence does not support the effectiveness of chelation therapy for any
purpose other than the treatment of heavy metal poisoning. Over-the-counter
chelation products are not approved for sale in the United States.
Chelation therapy is the
preferred medical treatment for metal poisoning, including acute mercury, iron
(including in cases of sickle-cell disease and thalassemia), arsenic, lead,
uranium, plutonium and other forms of toxic metal poisoning. The chelating
agent may be administered intravenously, intramuscularly, or orally, depending
on the agent and the type of poisoning.
CHELATING AGENTS
There are a variety of common
chelating agents with differing affinities for different metals, physical
characteristics, and biological mechanism of action. For the most common forms
of heavy metal intoxication � lead, arsenic, or mercury � a number of chelating
agents are available. Dimercaptosuccinic acid (DMSA) has been recommended for the
treatment of lead poisoning in children by poison control centers around the
world. Other chelating agents, such as 2,3-dimercaptopropanesulfonic acid
(DMPS) and alpha lipoic acid (ALA), are used in conventional and alternative
medicine. Some common chelating agents are ethylenediaminetetraacetic acid
(EDTA), 2,3-dimercaptopropanesulfonic acid (DMPS), and thiamine
tetrahydrofurfuryl disulfide (TTFD). Calcium-disodium EDTA and DMSA are only
approved for the removal of lead by the Food and Drug Administration while DMPS
and TTFD are not approved by the FDA. These drugs bind to heavy metals in the
body and prevent them from binding to other agents. They are then excreted from
the body. The chelating process also removes vital nutrients such as vitamins C
and E, therefore these must be supplemented.
The German Environmental Agency (Umweltbundesamt) listed
DMSA and DMPS as the two most useful and safe chelating agents available.
MEDICAL USES
Chelator Used in Dimercaprol
(British anti-Lewisite; BAL) acute arsenic poisoning acute mercury poisoning
lead poisoning (in addition to EDTA)
Lewisite poisoning (for which it was developed as an
antidote)
Dimercaptosuccinic acid (DMSA) lead poisoning arsenic poisoning
mercury poisoning
Dimercapto-propane sulfonate (DMPS) severe acute arsenic
poisoning severe acute mercury poisoning
Penicillamine
Mainly in: copper toxicity
Occasionally adjunctive therapy in: gold toxicity arsenic
poisoning lead poisoning rheumatoid arthritis
Ethylenediamine tetraacetic acid (calcium disodium versenate)
(CaNa2-EDTA) lead poisoning
Deferoxamine, Deferasirox and Deferiprone acute iron
poisoning iron overload
When used properly in response to
a diagnosis of harm from metal toxicity, side effects of chelation therapy
include dehydration, low blood calcium, harm to kidneys, increased enzymes as
would be detected in liver function tests, allergic reactions, and lowered
levels of dietary Side effects elements. When administered inappropriately,
there are the additional risks of hypocalcaemia (low calcium levels),
neurodevelopmental disorders, and death.
Chelation therapy can be traced
back to the early 1930s, when Ferdinand M�nz, a German chemist working for I.G.
Farben, first synthesized ethylenediaminetetraacetic acid (EDTA).
Munz was looking for a replacement
for citric acid as a water softener. Chelation therapy itself began during
World War II when chemists at the University of Oxford searched for an antidote
for lewisite, an arsenic-based chemical weapon. The chemists learned that EDTA
was particularly effective in treating lead poisoning.
Following World War II, chelation
therapy was used to treat workers who had painted United States naval vessels
with lead-based paints. In the 1950s, Norman Clarke, Sr. was treating workers
at a battery factory for lead poisoning when he noticed that some of his
patients had improved angina pectoris following chelation therapy. Clarke
subsequently administered chelation therapy to patients with angina pectoris
and other occlusive vascular disease and published his findings in The American
Journal of the Medical Sciences in December 1956. He hypothesized that
"EDTA could dissolve disease-causing plaques in the coronary systems of
human beings." In a series of 283 patients treated by Clarke et al. From
1956 to 1960, 87% showed improvement in their symptomatology. Other early
medical investigators made similar observations of EDTA's role in the treatment
of cardiovascular disease (Bechtel, 1956; Bessman, 1957; Perry, 1961; Szekely,
1963; Wenig, 1958: and Wilder, 1962).
In 1973, a group of practicing
physicians created the Academy of Medical Preventics (now the American College
for Advancement in Medicine). The academy trains and certifies physicians in
the safe administration of chelation therapy. Members of the academy continued
to use EDTA therapy for the treatment of vascular disease and developed safer
administration protocols.
In the 1960s, BAL was modified
into DMSA, a related dithiol with far fewer side effects. DMSA quickly replaced
both BAL and EDTA as the primary treatment for lead, arsenic and mercury
poisoning in the United States. Esters of DMSA have been developed which are
reportedly more effective; for example, the monoisoamyl ester (MiADMSA) is
reportedly more effective than DMSA at clearing mercury and cadmium. Research
in the former Soviet Union led to the introduction of DMPS, another dithiol, as
a mercury-chelating agent. The Soviets also introduced ALA, which is
transformed by the body into the dithiol dihydrolipoic acid, a mercury- and
arsenic- History chelating agent. DMPS has experimental status in the United
States, while ALA is a common nutritional supplement.
Since the 1970s, iron chelation
therapy has been used as an alternative to regular phlebotomy to treat excess
iron stores in people with haemochromatosis. Other chelating agents have been
discovered. They all function by making several chemical bonds with metal ions,
thus rendering them much less chemically reactive. The resulting complex is
water-soluble, allowing it to enter the bloodstream and be excreted harmlessly.
Calcium-disodium EDTA chelation
has been studied by the U.S. National Center for Complementary and Alternative
Medicine for treating coronary disease. In 1998, the U.S. Federal Trade
Commission (FTC) pursued the American College for Advancement in Medicine
(ACAM), an organization that promotes "complementary, alternative and
integrative medicine" over the claims made regarding the treatment of
atherosclerosis in advertisements for EDTA chelation therapy. The FTC concluded
that there was a lack of scientific studies to support these claims and that
the statements by the ACAM were false. In 1999, the ACAM agreed to stop
presenting chelation therapy as effective in treating heart disease, avoiding
legal proceedings.
In 2010 the U.S. Food and Drug
Administration (FDA) warned companies who sold over-the-counter (OTC) chelation
products and stated that such "products are unapproved drugs and devices
and that it is a violation of federal law to make unproven claims about these products.
There are no FDA-approved OTC chelation products."
In 1998, the U.S. Federal Trade
Commission (FTC) charged that the web site of the American College for
Advancement in Medicine (ACAM) and a brochure they published had made false or
unsubstantiated claims. In December 1998, the FTC announced that it had secured
a consent agreement barring ACAM from making unsubstantiated advertising claims
that chelation therapy is effective against atherosclerosis or any other
disease of the circulatory system.
In August 2005, doctor error led
to the death of a five-year-old autistic boy who was undergoing chelation
therapy. Others, including a three-year-old nonautistic girl and a nonautistic
adult, have died while undergoing chelation therapy. These deaths were due to cardiac
arrest caused by hypocalcemia during chelation therapy. In two of the cases
hypocalcemia appears to have been caused by the administration of Na2EDTA
(disodium EDTA) and in the third case the type of EDTA was unknown. Only the
3-year-old girl had found to have an elevated blood lead level and resulting
low iron levels and anemia, which is the conventional medical cause for Society
and culture administration of chelation therapy. According to protocol, EDTA
should not be used in the treatment of children. More than 30 deaths have been
recorded in association with IV-administered disodium EDTA since the 1970s.
USE IN ALTERNATIVE MEDICINE
In alternative medicine, some
practitioners claim chelation therapy can treat a variety of ailments,
including heart disease and autism. The use of chelation therapy by alternative
medicine practitioners for behavioral and other disorders is considered
pseudoscientific; there is no proof that it is effective. Chelation therapy
prior to heavy metal testing can artificially raise urinary heavy metal
concentrations (�provoked� urine testing) and lead to inappropriate and unnecessary
treatment. The American College of Medical Toxicology and the American Academy
of Clinical Toxicology warn the public that chelating drugs used in chelation
therapy may have serious side effects, including liver and kidney damage, blood
pressure changes, allergies and in some cases even death of the patient.
CANCER
The American Cancer Society says
of chelation therapy: "Available scientific evidence does not support
claims that it is effective for treating other conditions such as cancer.
Chelation therapy can be toxic and has the potential to cause kidney damage,
irregular heartbeat, and even death."
CARDIOVASCULAR DISEASE
According to the findings of a
1997 systematic review, EDTA chelation therapy is not effective as a treatment
for coronary artery disease and this use is not approved in the United States
by the US Food and Drug Administration (FDA).
The American Heart Association
stated in 1997 that there is "no scientific evidence to demonstrate any
benefit from this form of therapy." The United States Food and Drug
Administration (FDA), the National Institutes of Health (NIH) and the American
College of Cardiology "all agree with the American Heart Association"
that "there have been no adequate, controlled, published scientific
studies using currently approved scientific methodology to support this therapy
for cardiovascular disease." They speculate that any improvement among
heart patients undergoing chelation therapy can be attributed to the placebo
effect and generally recommended lifestyle changes such as "quitting
smoking, losing weight, eating more fruits and vegetables, avoiding foods high
in saturated fats and exercising regularly." They also are concerned that
patients could put off proven treatments for heart disease like drugs or
surgery.
A systematic review published in
2005 found that controlled scientific studies did not support chelation therapy
for heart disease. It found that very small trials and uncontrolled descriptive
studies have reported benefits while larger controlled studies have found
results no better than placebo.
In 2009, the Montana Board of
Medical Examiners issued a position paper concluding that "chelation
therapy has no proven efficacy in the treatment of cardiovascular disease, and
in some patients could be injurious."
The U.S. National Center for
Complementary and Alternative Medicine (NCCAM) conducted a trial on the
chelation therapy's safety and efficacy for patients with coronary artery
disease.
NCCAM Director Stephen E. Straus
cited the "widespread use of chelation therapy in lieu of established
therapies, the lack of adequate prior research to verify its safety and
effectiveness, and the overall impact of coronary artery disease" as factors
motivating the trial. The study has been criticized by some who said it was
unethical, unnecessary and dangerous, and that multiple studies conducted prior
to it demonstrated that the treatment provides no benefit.
The US National Center for
Complementary and Alternative Medicine began the Trial to Assess Chelation
Therapy (TACT) in 2003. Patient enrollment was to be completed around July 2009
with final completion around July 2010, but enrollment in the trial was
voluntarily suspended by organizers in September 2008 after the Office for
Human Research Protections began investigating complaints such as inadequate
informed consent. Additionally, the trial was criticized for lacking prior
Phase I and II studies, and critics summarized previous controlled trials as
having "found no evidence that chelation is superior to placebo for
treatment of CAD or PVD." The same critics argued that methodological
flaws and lack of prior probability made the trial "unethical, dangerous,
pointless, and wasteful." The American College of Cardiology supported the
trial and research to explore whether chelation therapy was effective in
treating heart disease. Evidence of insurance fraud and other felony
convictions among (chelation proponent) investigators further undermined the credibility
of the trial.
The final results of TACT were
published in November 2012. The authors concluded that disodium EDTA chelation
"modestly" reduced the risk of adverse cardiovascular outcomes among
stable patients with a history of myocardial infarction. The study also showed
a "marked" reduction in cardiovascular events in diabetic patients treated
with EDTA chelation.
An editorial published in the
Journal of the American Medical Association said that "the study findings
may provide novel hypotheses that merit further evaluation to help understand
the pathophysiology of secondary prevention of vascular disease." Critics
of the study characterized the study as showing no support for the use of
chelation therapy in coronary heart disease, particularly the claims to reduce
the need for coronary artery bypass grafting (CABG, pronounced
"cabbage").
AUTISM
Quackwatch says that autism is
one of the conditions for which chelation therapy has been falsely promoted as
effective, and practitioners falsify diagnoses of metal poisoning to trick
parents into having their children undergo the risky process. As of 2008, up to
7% of autistic children worldwide had been subjected to chelation therapy. The
death of two children in 2005 was caused by the administration of chelation
treatments, according to the American Center for Disease Control. One of them
was autistic. Parents either have a doctor use a treatment for lead poisoning,
or buy unregulated supplements, in particular DMSA and lipoic acid. Aspies For
Freedom, an autism rights organization, considers this use of chelation therapy
unethical and potentially dangerous. There is little to no credible scientific
research that supports the use of chelation therapy for the effective treatment
of autism.
(back
to content)
4.26
Chromotherapy w
Chromotherapy, sometimes called
color therapy, colorology or cromatherapy, is an alternative medicine method
that is considered pseudoscience and quackery. Chromotherapists claim to be
able to use light in the form of color to balance "energy" lacking
from a person's body, whether it be on physical, emotional, spiritual, or
mental levels. For example, they thought that shining a colored light on a
person would cure constipation.
Color therapy is unrelated to
photomedicine, such as phototherapy and blood irradiation therapy, which are
scientifically accepted medical treatments for a number of conditions, as well
as being unrelated to photobiology, which is the scientific study of the
effects of light on living organisms.
Avicenna (980�1037), seeing color
as of vital importance both in diagnosis and in treatment, discussed
chromotherapy in The Canon of Medicine. He wrote that "color is an
observable
CHROMOTHERAPY ALTERNATIVE MEDICINE
|
�
|
Edwin Dwight Babbitt, an early proponent of Chromotherapy
Claims������������������������������������������������������������������ Colored
light can balance "energy" in a human body.
Year ��������������������������������������������������������������������� proposed
1876
Original proponents �������������������������������������� Augustus
Pleasonton
Subsequent proponents ����������������������������� Seth
Pancoast, Edwin Dwight Babbitt
HISTORY
Avicenna (980�1037), seeing color
as of vital importance both in diagnosis and in treatment, discussed
chromotherapy in The Canon of Medicine. He wrote that "color is an
observable symptom of disease" and also developed a chart that related
color to the temperature and physical condition of the body. His view was that
red moved the blood, blue or white cooled it, and yellow reduced muscular pain
and inflammation.
American Civil War General
Augustus Pleasonton (1801�1894) conducted his own experiments and in 1876
published his book The Influence Of The Blue Ray Of The Sunlight And Of The
Blue Color Of The Sky about how the color blue can improve the growth of crops
and livestock and can help heal diseases in humans. This led to modern
chromotherapy, influencing scientist Dr. Seth Pancoast (1823�1889) and Edwin
Dwight Babbitt (1828�1905) to conduct experiments and to publish, respectively,
Blue and Red Light; or, Light and Its Rays as Medicine (1877) and The
Principles of Light and Color.
In 1933, Indian-born
American-citizen scientist Dinshah P. Ghadiali (1873�1966) published The
Spectro Chromemetry Encyclopaedia, a work on color therapy. Ghadiali claimed to
have discovered why and how the different colored rays have various therapeutic
effects on organisms. He believed that colors represent chemical potencies in
higher octaves of vibration, and for each organism and system of the body there
is a particular color that stimulates and another that inhibits the work of
that organ or system. Ghadiali also thought that, by knowing the action of the different
colors upon the different organs and systems of the body, one can apply the
correct color that will tend to balance the action of any organ or system that
has become abnormal in its function or condition. Dinshah P. Ghadiali's son,
Darius Dinshah, continues to provide information about color therapy via his
Dinshah Health Society, a nonprofit organization dedicated to advancing
non-pharmaceutical home color therapy, and his book Let There Be Light.
Science writer Martin Gardner had
described Ghadiali as "perhaps the greatest quack of them all".
According to Gardner, photographs of Ghadiali at work in his laboratory are
"indistinguishable from stills of a grade D movie about a mad scientist".
Throughout the 19th century
"color healers" claimed colored glass filters could treat many
diseases, including constipation and meningitis.
COLORED CHAKRAS
Practitioners of ayurvedic
medicine believe the body has seven "chakras", which some claim are
'spiritual centers', and are thought to be located along the spine. New Age
thought associates each of the chakras with a single color of the visible light
spectrum, along with a function and organ or bodily system. According to this
view, the chakras can become imbalanced and result in physical and mental
diseases, but application of the appropriate color can allegedly correct such
imbalances.
Chromotherapy is regarded by health experts as quackery.
According to a book published by
the American Cancer Society, "available scientific evidence does not
support claims that alternative uses of light or color therapy are effective in
treating cancer or other illnesses".
Photobiology, the term for the
scientific study of the effects of light on living tissue, has sometimes been
used instead of the term chromotherapy in an effort to distance it from its
roots in Victorian mysticism and to strip it of its associations with symbolism
and magic.
Light therapy is a specific
treatment approach using high intensity light to treat specific sleep, skin and
mood disorders.
A review of the existing research
on chromotherapy found that there is no evidence to support a causal link
between specific colors to health outcomes, there is not enough evidence to
support A New Age conceptualisation of the chakras of Indian body culture and
their positions in the human body Scientific rejection a causal link between
specific colors and emotional or mental states, and there is no research to
suggest there exists one-to-one relationships between specific colors and
emotions.
Chromotherapy has been accused of
oversimplifying psychological responses to colors, making sweeping statements
based on myths or beliefs that lack empirical support. Guidelines for
chromotherapy lack consistency and appear to be subjective judgements that have
inconclusive and nonspecific applicability in healthcare systems. While twelve
colors have been reported as beneficial for health and well-being, a rigorous
definition of each of these colors has yet to be provided, making it impossible
to know if all color therapists are using the same wavelengths for these
colors.
Chromotherapy has also been
criticized for its lack of falsifiability and verifiability. Critics have
further suggested that some positive results from the therapy are actually
placebo effects, where the mere introduction of a treatment led to health
improvements unrelated to the colors.
More recently, concern regarding
the theory has questioned the risks associated with the emergence of
light-emitting diode (LED) based lamps that have been created for use in chromotherapy,
these lamps are classified as low risk for exposure and do not require any
warnings to accompany the products. However, certain chromotherapy procedures
require the individual to place the lamps near their eyes, which is not the
recommended use for these lights and may alter the exposure duration to a level
that can cause risk of retinal damage. With no consensus or regulation
regarding how these products are to be used and whether eyewear is required,
this treatment puts participants at risk for serious eye damage.
(back
to content)
Energy
medicine w
Energy medicine is a branch of
alternative medicine based on a pseudo-scientific belief that healers can
channel "healing energy" into a patient and effect positive results.
Practitioners use a number of names including various synonyms for medicine
(e.g., energy healing) and sometimes use the word vibrational instead of or in
concert with energy. In most cases there is no empirically measurable energy
involved: the term refers instead to so-called subtle energy.
Practitioners may classify
practice as hands-on, hands-off, and distant (or absent) where the patient and
healer are in different locations. Many schools of energy healing exist using
many names: for example, biofield energy healing, spiritual healing, contact
healing, distant healing, therapeutic touch, Reiki or Qigong.
Reviews of the scientific
literature on energy healing have concluded that there is no evidence
supporting clinical efficacy. The theoretical basis of healing has been
criticised as implausible; research and reviews supportive of energy medicine
have been faulted for containing methodological flaws and selection bias, and
positive therapeutic results have been determined to result from known
psychological mechanisms. Some claims of those purveying "energy
medicine" devices are known to be fraudulent and their marketing practices
have drawn law-enforcement action in the US.
History records the repeated
association or exploitation of scientific inventions by individuals claiming
that newly discovered science could help people to heal. In the 19th century,
electricity History and magnetism were in the "borderlands" of
science and electrical quackery became rife.
These concepts continue to
inspire writers in the New Age movement. In the early-20th century health
claims for radio-active materials put lives at risk, and recently quantum
mechanics and grand unification theory have provided similar opportunities for
commercial exploitation. Thousands of devices claiming to heal via putative or
veritable energy are used worldwide. Many of them are illegal or dangerous and
are marketed with false or unproven claims. Several of these devices have been
banned.
Reliance on spiritual and
energetic healing is associated with serious harm or death when patients delay or
forego medical treatment.
The term "energy
medicine" has been in general use since the founding of the non-profit
International Society for the Study of Subtle Energies and Energy Medicine in
the 1980s. Guides are available for practitioners, and other books aim to
provide a theoretical basis and evidence for the practice. Energy medicine
often proposes that imbalances in the body's "energy field" result in
illness, and that by re-balancing the body's energy-field health can be
restored. Some modalities describe treatments as ridding the body of negative
energies or blockages in 'mind'; illness or episodes of ill health after a
treatment are referred to as a 'release' or letting go of a 'contraction' in
the body-mind. Usually, a practitioner will then recommend further treatments
for complete healing.
The US-based National Center for
Complementary and Integrative Health (NCCIH) distinguishes between health care
involving scientifically observable energy, which it calls "Veritable
Energy Medicine", and health care methods that invoke physically
undetectable or unverifiable "energies", which it calls
"Putative Energy Medicine":
Types of "veritable energy medicine" include
magnet therapy, colorpuncture, and light therapy. Medical techniques involving
the use of electromagnetic radiation (e.g. radiation therapy or magnetic
resonance imaging) are not considered "energy medicine" in the terms
of alternative medicine.
Types of "putative energy
medicine" include biofield energy healing therapies that are claimed to
direct or modulate "energies" to allow healing in the patient. This
includes spiritual healing, psychic healing, Therapeutic touch, Healing Touch,
Hands of light, Esoteric healing, Magnetic healing (now a historical term not
to be confused with magnet therapy), Qigong healing, Reiki, crystal healing,
Tong Ren therapy, distant healing, intercessory prayer, and Classification
similar modalities. Concepts such as Qi (Chi), Prana, Innate Intelligence,
Mana, Pneuma, vital fluid, Odic force, and orgone are among the many terms that
have been used to describe these putative energy fields. This category does not
include Acupuncture, Ayurvedic medicine, Chiropractic, Moxibustion and other
modalities where a physical intervention is used to manipulate a putative
energy.
Polarity therapy founded by Randolph
Stone is a kind of energy medicine based on the belief that a person's health
is subject to positive and negative charges in their electromagnetic field. It
has been promoted as capable of curing a number of human ailments ranging from
muscular tightness to cancer; however, according to the American Cancer Society
"available scientific evidence does not support claims that polarity
therapy is effective in treating cancer or any other disease".
There are various schools of energy healing, including biofield
energy healing, spiritual healing, contact healing, distant healing, Pranic
Healing, therapeutic touch, Reiki, and Qigong among others.
Spiritual healing occurs largely
among practitioners who do not see traditional religious faith as a
prerequisite for effecting cures. Faith healing by contrast takes place within
a traditional or non-denominational religious context such as with some
televangelists. The Buddha is often quoted by practitioners of energy medicine,
but he did not practise "hands on or off" healing.
BELIEFS
A REIKI
PRACTITIONER
Energy healing techniques such as
Therapeutic touch have found recognition in the nursing profession. In
2005�2006, the North American Nursing Diagnosis Association approved the
diagnosis of "energy field disturbance" in patients, reflective of
what has been variously called a "postmodern" or
"anti-scientific" approach to nursing care. This approach has been
strongly criticised.
Believers in these techniques
have proposed quantum mystical invocations of non-locality to try to explain
distant healing. They have also proposed that healers act as a channel passing
on a kind of bioelectromagnetism which shares similarities to vitalistic
pseudosciences such as orgone or qi. Writing in the Journal of Bodywork and
Movement Therapies, James Oschman introduced the concept of healer-sourced
electromagnetic fields which change in frequency. Oschman believes that
"healing energy" derives from electromagnetic frequencies generated
by a medical device, projected from the hands of the healer, or by electrons
acting as antioxidants. Beverly Rubik, in an article in the Journal of
Alternative and Complementary Medicine, justified her belief with references to
biophysical systems theory, bioelectromagnetics, and chaos theory that provide her
with a "...scientific foundation for the biofield..." Drew Leder
remarked in a paper in the same journal that such ideas were attempts to
"make sense of, interpret, and explore 'psi' and distant healing."
and that "such physics-based models are not presented as explanatory but
rather as suggestive."
Physicists and sceptics criticise these explanations as
pseudophysics � a branch of pseudoscience which explains magical thinking by
using irrelevant jargon from modern physics to exploit scientific illiteracy
and to impress the unsophisticated.
Indeed, even enthusiastic supporters of energy healing say
that "there are only very tenuous theoretical foundations underlying
[spiritual] healing".
DISTANT HEALING
A systematic review of 23 trials
of distant healing published in 2000 did not draw definitive conclusions
because of the methodological limitations among the studies. In 2001 the lead
author of that study, Edzard Ernst, published a primer on complementary
therapies in cancer care in which he explained that though "about half of
these trials suggested that healing is effective", the evidence was
"highly conflicting" and that "methodological shortcomings
prevented firm conclusions." He concluded that "as long as it is not used
as an alternative to Scientific investigations effective therapies, spiritual
healing should be virtually devoid of risks." A 2001 randomised clinical
trial by the same group found no statistically significant difference on
chronic pain between distance healers and "simulated healers". A 2003
review by Ernst updating previous work concluded that the weight of evidence
had shifted against the use of distant healing, and that it can be associated
with adverse effects.
CONTACT HEALING
A 2001 randomised clinical trial
randomly assigned 120 patients with chronic pain to either healers or
"simulated healers", but could not demonstrate efficacy for either
distance or face-to face healing. A systematic review in 2008 concluded that
the evidence for a specific effect of spiritual healing on relieving
neuropathic or neuralgic pain was not convincing. In their 2008 book Trick or
Treatment, Simon Singh and Edzard Ernst concluded that "spiritual healing
is biologically implausible and its effects rely on a placebo response. At best
it may offer comfort; at worst it can result in charlatans taking money from
patients with serious conditions who require urgent conventional
medicine."
EVIDENCE BASE
Alternative medicine researcher
Edzard Ernst has said that although an initial review of pre-1999 distant healing
trials had highlighted 57% of trials as showing positive results, later reviews
of non-randomised and randomised clinical trials conducted between 2000 and
2002 led to the conclusion that "the majority of the rigorous trials do
not support the hypothesis that distant healing has specific therapeutic
effects." Ernst described the evidence base for healing practices to be
"increasingly negative". Many of the reviews were also under
suspicion for fabricated data, lack of transparency, and scientific misconduct.
He concluded that "[s]piritual healing continues to be promoted despite
the absence of biological plausibility or convincing clinical evidence ... that
these methods work therapeutically and plenty to demonstrate that they do
not." A 2014 study of energy healing for colorectal cancer patients showed
no improvement in quality of life, depressive symptoms, mood, or sleep quality.
The Earthing Institute gathers researchers
and therapists who believe that to maintain or regain good health it is
necessary to restore direct contact with Earth by removing floors, carpets and
Earthing especially shoes. Walking barefoot and sleeping on the ground are
conceived as useful tools for achieving the �earthing� (or
"grounding") of our body. It is claimed that thanks to earthing one
would benefit from the �extraordinary healing power� of Nature by means of the
transferral of electrons from the Earth's surface to the body: �a primordial
and naturally stabilized electric reference point for all body biological
circuits is created.� According to its practitioners, Earthing has preventive
and curative effects on chronic inflammation, aging-related disorders,
cardiovascular diseases, diabetes, arthritis, autoimmune disorders, cancer, and
even depression and autism.
The concept of earthing has been
criticized as pseudoscience by skeptics and the medical community. A review of
the available literature on the subject was written by several people that are
financially tied to the company espousing the practice of earthing. Steven
Novella referred to the work as "typical of the kind of worthless studies
designed to generate false positives�the kind of in-house studies that
companies sometimes use so that they can claim their products are clinically
proven."
Bioresonance therapy (including
MORA therapy) is a pseudoscientific medical practice in which it is proposed
that electromagnetic waves can be used to diagnose and treat human illness.
History and method
Bioresonance therapy was invented (in Germany) in 1977 by
Franz Morell and his son-in-law, engineer Erich Rasche. Initially they marketed
it as "MORA-Therapie", for MOrell and RAsche.
Some of the machines contain an
electronic circuit measuring skin-resistance, akin to the Emeter used by
Scientology, which the bioresonance creators sought to improve; Franz Morell
had links with Scientology.
Practitioners claim to be able to
detect a variety of diseases and addictions. Some practitioners also claim they
can treat diseases using this therapy without drugs, by stimulating a change of
"bioresonance" in the cells, and reversing the change caused by the
disease. The devices would need to be able to isolate and pinpoint pathogens'
responses from the mixture of responses the device receives via the electrodes.
Transmitting these transformed signals over the same electrodes is claimed by
practitioners to generate healing signals that have the curative effect.
BIORESONANCE THERAPY
SCIENTIFIC EVALUATION
Lacking any scientific explanation of how bioresonance
therapy might work, researchers have classified bioresonance therapy as
pseudoscience.
Some studies did not show effects
above that of the placebo effect. WebMD states: "There is no reliable
scientific evidence that bioresonance is an accurate indicator of medical
conditions or disease or an effective treatment for any condition."
Proven cases of online fraud have
occurred, with a practitioner making false claims that he had the ability to
cure cancer, and that his clients did not need to follow the chemotherapy or
surgery recommended by medical doctors, which can be life-saving. Ben Goldacre
ridiculed the BBC when it reported as fact a clinic's claim that the treatment
had the ability to stop 70% of clients smoking, a better result than any
conventional therapy.
In the United States of America, the U.S. Food and Drug
Administration (FDA) classifies "devices that use resistance measurements
to diagnose and treat various diseases" as Class III devices, which
require FDA approval prior to marketing. The FDA has banned some of these
devices from the US market, and has prosecuted many sellers of electrical
devices for making false claims of health benefits.
According to Quackwatch, the
therapy is completely nonsensical and the proposed mechanism of action
impossible.
There are several, primarily
psychological, explanations for positive reports after energy herapy, including
placebo effects, spontaneous remission, and cognitive dissonance. A 2009 review
found that the "small successes" reported for two therapies
collectively marketed as "energy psychology" (Emotional Freedom
Techniques and Tapas Acupressure Technique) "are potentially attributable
to well-known cognitive and behavioral techniques that are included with the
energy manipulation." The report concluded that "[p]sychologists and
researchers should be wary of using such techniques, and make efforts to inform
the public about the ill effects of therapies that advertise miraculous
claims."
There are primarily two
explanations for anecdotes of cures or improvements, relieving any need to
appeal to the supernatural. The first is post hoc ergo propter hoc, meaning
that a genuine improvement or spontaneous remission may have been experienced
coincidental with but Explanations for positive reports independent from
anything the healer or patient did or said. These patients would have improved
just as well even had they done nothing. The second is the placebo effect,
through which a person may experience genuine pain relief and other symptomatic
alleviation. In this case, the patient genuinely has been helped by the healer
� not through any mysterious or numinous function, but by the power of their
own belief that they would be healed. In both cases the patient may experience
a real reduction in symptoms, though in neither case has anything miraculous or
inexplicable occurred. Both cases are strictly limited to the body's natural
abilities.
Positive findings from research
studies can also result from such psychological mechanisms, or as a result of
experimenter bias, methodological flaws such as lack of blinding, or
publication bias; positive reviews of the scientific literature may show
selection bias, in that they omit key studies that do not agree with the
author's position. All of these factors must be considered when evaluating
claims.
(back
to content)
4.27 Feldenkrais Method w
The Feldenkrais Method is a type
of exercise therapy devised by Israeli Mosh� Feldenkrais (1904�1984) during the
mid-20th century. The method is claimed to reorganize connections between the
brain and body and so improve body movement and psychological state.
There is no good medical evidence
that the Feldenkrais method confers any health benefits. It is not known if it
is safe or cost-effective, but researchers do not believe it poses serious
risks.
The Feldenkrais Method is a type
of alternative exercise therapy that proponents claim can repair impaired
connections between the motor cortex and the body, so benefiting the quality of
body movement and improving wellbeing. The Feldenkrais Guild of North America
claims that the Feldenkrais method allows people to "rediscover [their]
innate capacity for graceful, efficient movement" and that "These improvements
will often generalize to enhance functioning in other aspects of [their]
life". Proponents claim that the Feldenkrais Method can benefit people
with a number of medical conditions, including children with autism, and people
with multiple sclerosis. However, no studies in which participants were clearly
identified as having an autism spectrum disorder or developmental disabilities
have been presented to back this claims.
In a session, a Feldenkrais
practitioner directs attention to habitual movement patterns that are thought
to be inefficient or strained, and attempts to teach new patterns using gentle,
slow, repeated movements. Slow repetition is believed to be necessary to impart
a new habit and Description allow it to begin to feel normal. These movements
may be passive (performed by the practitioner on the recipient's body) or
active (performed by the recipient). The recipient is fully clothed.
In 2015, the Australian
Government's Department of Health published the results of a review of
alternative therapies that sought to determine if any were suitable for being
covered by health insurance; the Feldenkrais Method was one of 17 therapies
evaluated for which no clear evidence of effectiveness was found. Accordingly,
in 2017 the Australian government identified the Feldenkrais Method as a
practice that would not qualify for insurance subsidy, saying this step would
"ensure taxpayer funds are expended appropriately and not directed to
therapies lacking evidence".
The Feldenkrais Method is
promoted with anecdotal claims it can help children with autism and other
developmental disorders, but such claims are not backed by reputable supporting
evidence.
There is limited evidence that
workplace-based use of the Feldenkrais Method may help aid rehabilitation of
people with upper limb complaints.
David Gorski has written that the
Method bears similarities to faith healing, is like "glorified yoga",
and that it "borders on quackery". Quackwatch places the Feldenkrais
Method on its list of "Unnaturalistic methods".
Students at the San Francisco
Feldenkrais Practitioner Training doing an Awareness Through Movement lesson
(1975)
EFFECTIVENESS AND RECEPTION
HISTORY
Similar to some other somatic
methods, such as those started by F. Matthias Alexander, Elsa Gindler, and
Gerda Alexander, the Feldenkrais Method originated in the efforts of its
founder to work with his own bodily problem. In the case of Mosh� Feldenkrais,
it was a chronically injured knee.
Feldenkrais first injured his
knee while playing soccer in British-controlled Palestine in the 1920s. He
reinjured it while negotiating the slippery decks of submarines while working
as a scientist at the British Naval station at Fairlie, Scotland during the
Second World War.
By that time Feldenkrais was a
judo teacher and had mostly completed the work toward a D.Sc. under the
guidance of Nobel laureate Fr�d�ric Joliot-Curie. Facing the prospect of a
surgery that could leave him with a life-long limp, Feldenkrais decided to
apply the knowledge gained from his study of physics, engineering, and martial
arts to an intensive self-study of his own movement habits. When his work
provided him with relief, allowing him to avoid the knee surgery, he began
exploring the methods he developed on himself with a small group of people at
Fairlie, including scientific colleague John Desmond Bernal and John Boyd-Orr,
Nobel laureate and first president of the World Academy of Art and Science.
After serving as head of
electronic engineering for the Israeli Army in newly formed Israel from 1951 to
1953, Feldenkrais devoted the rest of his life, from age 50 onward, to
developing and teaching self-awareness through movement lessons.
From the 1950s till his death in 1984, he taught
continuously in his home city of Tel Aviv.
Feldenkrais gained recognition in
part through media accounts of his work with prominent individuals, including
Israeli Prime Minister David Ben-Gurion. Beginning in the late 1950s,
Feldenkrais made trips to teach in Europe and America. Several hundred people
became certified Feldenkrais practitioners through trainings he held in San
Francisco from 1975 to 1978 and in Amherst, Massachusetts, from 1980 to 1984.
Anticipating the need for an institutional structure to carry on his teaching,
he helped found the Feldenkrais Guild of North America in 1977.
Feldenkrais developed the conceptual framework of his method
in part through the publication of six books, beginning with Body and Mature
Behavior (1949) and ending with the posthumously published The Potent Self
(1985).
Since Feldenkrais' death, the
international Feldenkrais community has used a guild structure to regulate its
activity, with training accreditation boards in the Americas, Europe, and
Australasia overseeing guilds and associations in eighteen member countries.
The Feldenkrais Journal, the annual publication of the Feldenkrais Guild of
North America, serves as a forum for the Feldenkrais community to discuss the method
and its applications.
The development of the
Feldenkrais Method was influenced by Moshe Feldenkrais's involvement in the
martial arts. After meeting Kano Jigoro, the founder of Judo, while living in
Paris in the 1930s, Feldenkrais transitioned to that practice. One of the main
influences of judo on the Feldenkrais Method is the differentiation between
rote exercise and attentive movement: "the methods of physical exercise in
vogue ... exert only the muscles without any other goal, and one needs much
will to bind oneself unfailingly to one of these methods", wrote
Feldenkrais in 1952.
"Judo is very different,
each movement has a specific goal which is reached after a precise and supple
execution." Before he focused on the creation of his own method, Feldenkrais
influenced the teaching of martial arts in Western Europe through the
publication of five books on jiujitsu and judo, as well as teaching at practice
centers in France and Great Britain.
Feldenkrais was born into an
Hasidic family and community, and he acknowledged the influence of Hasidic
Judaism on his method. In David Kaetz's biography, Making Connections: Roots
and Resonance in the Life of Moshe Feldenkrais (2007), he argues many lines of
influence can be found between the Judaism of Feldenkrais's upbringing and the
Feldenkrais Method � for instance, the use of paradox as a pedagogical tool.
Feldenkrais also acknowledged the influence of the Russian spiritualist George
Gurdjieff on his work, in particular Gurdjieff's teachings on automatism and
freedom in embodiment. Feldenkrais earned his doctorate in a program at the
Sorbonne intended to bridge theoretical physics and industrial engineering.
Mark Reese, another biographer of the teacher, says that Feldenkrais brought
this emphasis on practical scientific inquiry to the understanding of
embodiment expressed through his method: Feldenkrais was critical of the
appropriation of the term 'energy' to express immeasurable phenomena or to
label experiences that people had trouble describing ... He was impatient when
someone invoked energy in pseudoscientific 'explanations' that masked a lack of
understanding. In such cases he urged skepticism and scientific discourse. He
encouraged empirical and phenomenological narratives that could lead to
insights.
INFLUENCES
Feldenkrais incorporated the
views of other scientists into his teaching; for instance, he asked questions
of both the neurosurgeon Karl H. Pribram and the cyberneticist Heinz von
Foerster at trainings in San Francisco in the mid-1970s. Cybernetics, also
known as dynamic systems theory, continued to influence the Feldenkrais Method
in the 1990s through the work of human development researcher Esther Thelen.
(back
to content)
4.29 Horticultural therapy
w
Horticultural therapy (also known
as garden therapy or social and therapeutic horticulture or STH) is defined by
the American Horticultural Therapy Association (AHTA) as the engagement of a
person in gardening and plant-based activities, facilitated by a trained
therapist, to achieve specific therapeutic treatment goals. Direct contact with
plants is believed to guide a person's focus away from stress enhancing their
overall quality of life. The AHTA believes that horticultural therapy is an
active process which occurs in the context of an established treatment plan.
Horticultural therapists are specially educated and trained members of
rehabilitation teams (with doctors, psychiatrists, psychologists, occupational
therapists and others) who involve the client in all phases of gardening, from
propagation to selling products, as a means of bringing about improvement in
their life.
The use of horticulture to calm
the senses dates as far back as 2000 BC in ancient Mesopotamia, and around 500
BC, ancient Persians created gardens to soothe the senses by involving beauty,
fragrance, flowing water, and cool temperatures. According to the American
Horticultural Therapy Association, Ancient Egyptian physicians prescribed walks
around a garden for patients with mental illness; which makes the first sign of
the therapeutic process in Alexandria and Ancient Egypt through Renaissance
Europe. During the Middle Ages, on the grounds of a monastery hospital, plants
were used to express purpose of cheering up melancholy patients. Also, the
gardens were used to treat both physical and mental ailments of sickness who
visited them. The first modern documentation of horticulture being used as a
treatment for mental health purposes was in the 1800s. Dr. Benjamin Rush was
the first to suggest that field labor in a farm setting helped attain positive
outcomes for clients with mental illness. This discovery led many hospitals in
the western world to begin using horticulture as a means to start
therapeutically treating patients with mental health and developmental
disabilities. In 1817, the Asylum for Persons Deprived of Their Reason, now
known as Friends Hospital, constructed an environment with landscaping, paths
and a park atmosphere in effort to assist patients in their recovery. In 1879
Friends Hospital built the first greenhouse that was used for therapy. Post
World War 1 horticultural therapy was used to help servicemen rehabilitate, in
the 1940s garden club members brought garden activities to the servicemen and
in 1960 the first published book on horticultural therapy was written. The
first degree in horticultural therapy was established in 1972.
VETERANS PARTICIPATING IN HORTICULTURAL THERAPY
HISTORY
In 1973 the Council for Therapy
and Rehabilitation through Horticulture (NCTRH) was established by a group of
horticulture therapy professionals. In 1988, they changed their name to the
American Horticulture Therapy Association (AHTA) which they are still called
today. AHTA is a non-profit organization with about 25% off their members being
professionally registered.
Today, horticultural therapy is
practiced in many countries and area in the world, such as in Japan, Korea,
Hong Kong, the United Kingdom, Germany, Italy, India and Sweden. Many
universities in these countries have education programs and research in
horticultural therapy.
Special laboratories have also
been built, such as Alnarp Rehabilitation Garden at the Swedish University of
Agricultural Sciences campus area in Alnarp. In India Horticultural Therapy
Healing center, founded by Karthikeyan V, one of the pioneer in Horticultural
Therapy in India, has conducting sessions for various populations in Horticultural
Therapy.
Goals and types of treatment vary depending on the facility
using horticultural therapy.
Institutions from schools and
nursing homes to prisons utilize horticultural therapy to meet therapeutic
needs. Each one of these facilities have different types of horticultural
therapy, each with their own individual forms of treatment. Fundamentally
horticultural therapy can be divided into three types of programming: Vocational,
therapeutic, and social.
VOCATIONAL HORTICULTURAL THERAPY
Vocational Horticultural Therapy
is intended to teach skill and enhance behaviors that can be used in a job or
workplace. People undergoing vocational therapy can learn skills involving
greenhouses, vegetable gardening, tree and shrub care, as well as learn about plant
production, sales and services. Activities vocational therapy teaches consists
of how to repot, water, and move plants within their space. Learning the basic
knowledge of their plants root system and the care different plants need is
taught at their own pace. Ultimately aimed at employment, vocational
horticulture therapy teaches people how to grow and work with plants while also
learning the benefits of supporting themselves mentally and financially.
TYPES OF TREATMENT
THERAPEUTIC HORTICULTURAL THERAPY
Therapeutic Horticultural Therapy
has its focus on medical and illness recovery. The central belief that
therapeutic horticulture therapy revolves around is that being in nature has
restorative properties. Therapeutic horticulture might be used to try and
improve physical activity, social skills and engagement. Activities encompassed
by therapeutic horticulture vary widely, some activities include: repetitive
actions such as digging and watering, making observations about plant growth
and change, relating plant life cycle to human life, and starting seeds. It has
been suggested that things such as new growth on their plants can excite the
caretaker, building up their confidence and increasing enthusiasm towards
horticultural activities. The impact that therapeutic horticulture has on both
mind and body, as well as its ability to be undertaken in small spaces makes
therapeutic horticulture an attractive option for smaller facilities. An
extensive systematic review with meta-analysis examined the effectiveness of horticultural
therapy. A significant positive association with gardening was observed for a
wide range of health outcomes, such as reductions in depression and anxiety
symptoms, stress, mood disturbance, and BMI, as well as increases in quality of
life, sense of community, physical activity levels, and cognitive function.
SOCIAL HORTICULTURAL THERAPY
Social Horticultural Therapy is focused on leisure activity
and enhancement of life quality.
Unlike therapeutic horticultural
therapy, social horticultural therapy is more likely to be activity based.
Social Horticulture therapy works to create a community that focuses on plant
growth and teaches self-reliance all while providing a support system.
Another element of social
horticultural knowledge and expertise is to advise patients and the general
public how different herbs and spices can be added to their meals to give
flavour and to Gardening greenhouse cure minor ailments. If the varies herbs
and edible food crops and plants are planted in their gardens. The patient and
or their family can go and pick the varies herbs to add to their meals.
Carers with horticultural
knowledge and expertise can advise their patients and their families which
herbs can be used for different dishes, and advise what other ingredients would
work well with these dishes.
(back
to content)
4.30
Hydrotherapy w
Hydrotherapy, formerly called
hydropathy and also called water cure, is a branch of alternative medicine
(particularly naturopathy), occupational therapy, and physiotherapy, that
involves the use of water for pain relief and treatment. The term encompasses a
broad range of approaches and therapeutic methods that take advantage of the
physical properties of water, such as temperature and pressure, to stimulate
blood circulation, and treat the symptoms of certain diseases.
Various therapies used in the
present-day hydrotherapy employ water jets, underwater massage and mineral
baths (e.g. balneotherapy, Iodine-Grine therapy, Kneipp treatments, Scotch
hose, Swiss shower, thalassotherapy) or whirlpool bath, hot Roman bath, hot
tub, Jacuzzi, and cold plunge.
HYDROTHERAPY
USES
Water therapy may be restricted
to use as aquatic therapy, a form of physical therapy, and as a cleansing
agent. However, it is also used as a medium for delivery of heat and cold to
the body, which has long been the basis for its application. Hydrotherapy
involves a range of methods and techniques, many of which use water as a medium
to facilitate thermoregulatory reactions for therapeutic benefit.
Hydrotherapy is used as an
adjunct to therapy, including in nursing, where its use is now long
established. It continues to be widely used for burn treatment, although
shower-based hydrotherapy techniques have been increasingly used in preference
to full-immersion methods, partly for the ease of cleaning the equipment and
reducing infections due to contamination.
When removal of tissue is
necessary for the treatment of wounds, hydrotherapy which performs selective
mechanical debridement can be used. Examples of this include directed wound
irrigation and therapeutic irrigation with suction.
The appliances and arrangements
by means of which heat and cold are brought to bear are: Packings, general and
local (i.e. IcyHot);
Hot air and steam baths;
General baths;
Sitz (sitting), spinal, head, and foot baths;
Bandages or compresses, wet and dry; also;
Fomentations and poultices, sinapisms, stupes, rubbings, and
water potations.
Opening of the new Hydrotherapy Pool, Manchester Royal
Infirmary, 2009
TECHNIQUE
Hydrotherapy which involves submerging all or part of the
body in water can involve several types of equipment:
Full body immersion tanks (a "Hubbard tank" is a
large size)
Arm, hip, and leg whirlpool
Whirling water movement, provided
by mechanical pumps, has been used in water tanks since at least the 1940s.
Similar technologies have been marketed for recreational use under the terms
"hot tub" or "spa".
In some cases, baths with
whirlpool water flow are not used to manage wounds, as a whirlpool will not
selectively target the tissue to be removed, and can damage all tissue.
Whirlpools also create an unwanted risk of bacterial infection, can damage
fragile body tissue, and in the case of treating arms and legs, bring risk of
complications from edema.
The therapeutic use of water has
been recorded in ancient Egyptian, Greek and Roman civilizations. Egyptian
royalty bathed with essential oils and flowers, while Romans had communal
public baths for their citizens. Hippocrates prescribed bathing in spring water
for sickness. Other cultures noted for a long history of hydrotherapy include
China and Japan, the latter being centred primarily around Japanese hot
springs. Many such histories predate the Roman thermae.
MODERN REVIVAL
HISTORY
Hydrotherapy became more
prominent following the growth and development of modern medical practices in
the 18th and 19th century. As traditional medical practice became increasingly
professional in terms of how doctors operated, it was felt that medical
treatment became increasingly less personalized, the development of
hydrotherapy was believed to be a more personal form of medical treatment that
did not necessarily present to patients the alienating scientific language that
modern developments of medical treatment entailed.
1700�1810
Two English works on the medical
uses of water were published in the 18th century that inaugurated the new
fashion for hydrotherapy. One of these was by Sir John Floyer, a physician of
Lichfield, who, struck by the remedial use of certain springs by the
neighbouring peasantry, investigated the history of cold bathing and published
a book on the subject in 1702. The book ran through six editions within a few
years and the translation of this book into German was largely drawn upon by Dr
J. S. Hahn of Silesia as the basis for his book called On the Healing Virtues
of Cold Water, Inwardly and Outwardly Applied, as Proved by Experience,
published in 1738.
The other work was a 1797
publication by Dr James Currie of Liverpool on the use of hot and cold water in
the treatment of fever and other illness, with a fourth edition published in
1805, not long before his death. It was also translated into German by
Michaelis (1801) and Hegewisch (1807). It was highly popular and first placed
the subject on a scientific basis. Hahn's writings had meanwhile created much
enthusiasm among his countrymen, societies having been formed everywhere to
promote the medicinal and dietetic use of water; and in 1804 Professor E.F.C.
Oertel of Anspach republished
them and quickened the popular movement by unqualified commendation of water
drinking as a remedy for all diseases.
The general idea behind
hydropathy during the 1800s was to be able to induce something called a crisis.
The thinking was that water invaded any cracks, wounds, or imperfections in the
skin, which were filled with impure fluids. Health was considered to be the
natural state of the body, and filling these spaces with pure water, would
flush the impurities out, which would rise to the surface of the skin, producing
pus. The event of this pus emerging was called a crisis, and was achieved
through a multitude of methods. These methods included techniques such as James
Currie, who, according to Captain R. T. Claridge, discovered "...the merit
of settling the use of cold water...[and who established] the scientific base
of Hydropathy" sweating, the plunging bath, the half bath, the head bath,
the sitting bath, and the douche bath.
All of these were ways to gently expose the patient to cold
water in different ways.
Vincenz Priessnitz (1799�1851)
Vincenz Priessnitz was the son of
a peasant farmer who, as a young child, observed a wounded deer bathing a wound
in a pond near his home. Over the course of several days, he would see this
deer return and eventually the wound was healed. Later as a teenager,
Priessnitz was attending to a horse cart, when the cart ran him over, breaking
three of his ribs. A physician told him that they would never heal. Priessnitz
decided to try his own hand at healing himself, and wrapped his wounds with damp
bandages. By daily changing his bandages and drinking large quantities of
water, after about a year, his broken ribs had been cured. Priessnitz quickly
gained fame in his hometown and became the consulted physician.
Later in life, Priessnitz became
the head of a hydropathy clinic in Gr�fenberg in 1826. He was extremely
successful and by 1840, he had 1600 patients in his clinic including many
fellow physicians, as well as important political figures such as nobles and
prominent military officials.
Treatment length at Priessnitz's
clinic varied. Much of his theory was about inducing the abovementioned crisis,
which could happen quickly, or could occur after three to four years. In
accordance with the simplistic nature of hydropathy, a large part of the treatment
was based on living a simple lifestyle. These lifestyle adjustments included
dietary changes such as eating only very coarse food, such as jerky and bread,
and of course drinking large quantities of Vincenz Priessnitz, who initiated
the popular revival of hydrotherapy at Gr�fenberg water. Priessnitz's
treatments also included a great deal of less strenuous exercise, mostly
including walking. Ultimately, Priessnitz's clinic was extremely successful,
and he gained fame across the western world. His practice even influenced the
hydropathy that took root overseas in America.
Sebastian Kneipp (1821�1897)
Sebastian Kneipp was born in
Germany and he considered his own role in hydropathy to be that of continuing
Priessnitz's work. Kneipp's own practice of hydropathy was even gentler than
the norm. He believed that typical hydropathic practices deployed were
"too violent or too frequent" and he expressed concern that such
techniques would cause emotional or physical trauma to the patient. Kneipp's practice
was more all encompassing than Priessnitz's, and his practice involved not only
curing the patients' physical woes, but emotional and mental as well.
Kneipp introduced four additional
principles to the therapy: medicinal herbs, massages, balanced nutrition, and
"regulative therapy to seek inner balance". Kneipp had a very simple
view of an already simple practice. For him, hydropathy's primary goals were
strengthening the constitution and removing poisons and toxins in the body.
These basic interpretations of how hydropathy worked hinted at his complete
lack of medical training. Kneipp did have, however, a very successful medical
practice in spite of, perhaps even because of, his lack of medical training. As
mentioned above, some patients were beginning to feel uncomfortable with
traditional doctors because of the elitism of the medical profession. The new
terms and techniques that doctors were using were difficult for the average
person to understand. Having no formal training, all of his instructions and
published works are described in easy to understand language and would have
seemed very appealing to a patient who was displeased with the direction
traditional medicine was taking.
A significant factor in the
popular revival of hydrotherapy was that it could be practised relatively
cheaply at home. The growth of hydrotherapy (or 'hydropathy' to use the name of
the time), was thus partly derived from two interacting spheres: "the
hydro and the home".
Hydrotherapy as a formal medical
tool dates from about 1829 when Vincenz Priessnitz (1799�1851), a farmer of
Gr�fenberg in Silesia, then part of the Austrian Empire, began his public
career in the paternal homestead, extended so as to accommodate the increasing
numbers attracted by the fame of his cures.
At Gr�fenberg, to which the fame
of Priessnitz drew people of every rank and many countries, medical men were
conspicuous by their numbers, some being attracted by curiosity, others by the
desire of knowledge, but the majority by the hope of cure for ailments which had
as yet proved incurable. Many records of experiences at Gr�fenberg were
published, all more or less favorable to the claims of Priessnitz, and some
enthusiastic in their estimate of his genius and penetration.
SPREAD OF HYDROTHERAPY
Captain R. T. Claridge was
responsible for introducing and promoting hydropathy in Britain, first in
London in 1842, then with lecture tours in Ireland and Scotland in 1843. His
10-week tour in Ireland included Limerick, Cork, Wexford, Dublin and Belfast,
over June, July and August 1843, with two subsequent lectures in Glasgow.
Some other Englishmen preceded
Claridge to Graefenberg, although not many. One of these was Dr. James Wilson,
who himself, along with Dr James Manby Gully, established and operated a water
cure establishment at Malvern in 1842. In 1843, Wilson and Gully published a
comparison of the efficacy of the water-cure with drug treatments, including
accounts of some cases treated at Malvern, combined with a prospectus of their
Water Cure Establishment.
Then in 1846 Gully published The
Water Cure in Chronic Disease, further describing the treatments available at
the clinic.
Hydropathic applications according to Claridge's Hydropathy
book
The fame of the water-cure
establishment grew, and Gully and Wilson became well-known national figures.
Two more clinics were opened at Malvern. Famous patients included Charles
Darwin, Charles Dickens, Thomas Carlyle, Florence Nightingale, Lord Tennyson
and Samuel Wilberforce. With his fame he also attracted criticism:
Sir Charles Hastings, a physician and founder of the British
Medical Association, was a forthright critic of hydropathy, and Gully in
particular.
From the 1840s, hydropathics were
established across Britain. Initially, many of these were small institutions,
catering to at most dozens of patients. By the later nineteenth century the
typical hydropathic establishment had evolved into a more substantial
undertaking, with thousands of patients treated annually for weeks at a time in
a large purpose-built building with lavish facilities � baths, recreation rooms
and the like � under the supervision of fully trained and qualified medical
practitioners and staff.
In Germany, France and America,
and in Malvern, England, hydropathic establishments multiplied with great
rapidity. Antagonism ran high between the old practice and the new. Unsparing
condemnation was heaped by each on the other; and a legal prosecution, leading
to a royal commission of inquiry, served but to make Priessnitz and his system
stand higher in public estimation.
Increasing popularity soon
diminished caution whether the new method would help minor ailments and be of
benefit to the more seriously injured. Hydropathists occupied themselves mainly
with studying chronic invalids well able to bear a rigorous regimen and the
severities of unrestricted crisis. The need of a radical adaptation to the
former class was first adequately recognized by John Smedley, a manufacturer of
Derbyshire, who, impressed in his own person with the severities as well as the
benefits of the cold water cure, practised among his workpeople a milder form
of hydropathy, and began about 1852 a new era in its history, founding at
Matlock a counterpart of the establishment at Gr�fenberg.
Ernst Brand (1827�1897) of
Berlin, Raljen and Theodor von J�rgensen of Kiel, and Karl Liebermeister of
Basel, between 1860 and 1870, employed the cooling bath in abdominal typhus
with striking results, and led to its introduction to England by Dr Wilson Fox.
In the Franco-German War the cooling bath was largely employed, in conjunction
frequently with quinine; and it was used in the treatment of hyperpyrexia.
HOT BATHS
Hydrotherapy, especially as
promoted during the height of its Victorian revival, has often been associated
with the use of cold water, as evidenced by many titles from that era. However,
not all therapists limited their practice of hydrotherapy to cold water, even
during the height of this popular revival.
The specific use of heat was
however often associated with the Turkish bath. This was introduced by David
Urquhart into England on his return from the East in the 1850s, and ardently
adopted by Richard Barter. The Turkish bath became a public institution, and,
with the morning tub and the general practice of water drinking, is the most
noteworthy of the many contributions by hydropathy to public health.
SPREAD TO THE UNITED STATES
The first U.S. hydropathic
facilities were established by Joel Shew and Russell Thacher Trall in the
1840s. Dr Charles Munde also established early hydrotherapy facilities in the
1850s. Trall also co-edited the Water Cure Journal.
By 1850, it was said that
"there are probably more than one hundred" facilities, along with
numerous books and periodicals, including the New York Water Cure Journal,
which had Baigneuses, oil on canvas, Jean-L�on G�r�me (1824�1904)
"attained an extent of circulation equaled by few monthlies in the
world". By 1855, there were attempts by some to weigh the evidence of
treatments in vogue at that time.
Following the introduction of
hydrotherapy to the U.S., John Harvey Kellogg employed it at Battle Creek
Sanitarium, which opened in 1866, where he strove to improve the scientific
foundation for hydrotherapy. Other notable hydropathic centers of the era
included the Cleveland Water Cure Establishment, founded in 1848, which
operated successfully for two decades, before being sold to an organization
which transformed it into an orphanage.
At its height, there were over
200 water-cure establishments in the United States, most located in the
northeast. Few of these lasted into the postbellum years, although some
survived into the 20th century including institutions in Scott (Cortland
County), Elmira, Clifton Springs and Dansville. While none were located in
Jefferson County, the Oswego Water Cure operated in the city of Oswego.
SUBSEQUENT DEVELOPMENTS
In November 1881, the British
Medical Journal noted that hydropathy was a specific instance, or
"particular case", of general principles of thermodynamics. That is,
"the application of heat and cold in general", as it applies to
physiology, mediated by hydropathy. In 1883, another writer stated "Not,
be it observed, that hydropathy is a water treatment after all, but that water
is the medium for the application of heat and cold to the body".
Hydrotherapy was used to treat
people with mental illness in the 19th and 20th centuries and before World War
II, various forms of hydrotherapy were used to treat alcoholism.
The basic text of the Alcoholics
Anonymous fellowship, Alcoholics Anonymous, reports that A.A. co-founder Bill
Wilson was treated by hydrotherapy for his alcoholism in the early 1930s.
RECENT TECHNIQUES
A subset of cryotherapy involves
cold water immersion or ice baths, used by physical therapists, sports medicine
facilities and rehab clinics. Proponents assert that it results in improved
return of blood flow and byproducts of cellular breakdown to the lymphatic
system and more efficient recycling.
Alternating the temperatures,
either in a shower or complementary tanks, combines the use of hot and cold in
the same session. Proponents claim improvement in circulatory system and
lymphatic drainage. Experimental evidence suggests that contrast hydrotherapy
helps to reduce injury in the acute stages by stimulating blood flow and
reducing swelling.
The growth of hydrotherapy, and
various forms of hydropathic establishments, resulted in a form of tourism,
both in the UK, and in Europe. At least one book listed English, Scottish,
Irish and European establishments suitable for each specific malady, while
another focused primarily on German spas and hydropathic establishments, but
including other areas. While many bathing establishments were open all year
round, doctors advised patients not to go before May, "nor to remain after
October. English visitors rather prefer cold weather, and they often arrive for
the baths in May, and return again in September. Americans come during the
whole season, but prefer summer. The most fashionable and crowded time is
during July and August". In Europe, interest in various forms of
hydrotherapy and spa tourism continued unabated through the 19th century and
into the 20th century, where "in France, Italy and Germany, several
million people spend time each year at a spa." In 1891, when Mark Twain
toured Europe and discovered that a bath of spring water at Aix-les-Bains
soothed his rheumatism, he described the experience as "so enjoyable that
if I hadn't had a disease I would have borrowed one just to have a pretext for
going on".
This was not the first time such forms of spa tourism had
been popular in Europe and the U.K.
Indeed, in Europe, the
application of water in the treatment of fevers and other maladies had, since
the seventeenth century, been consistently promoted by a number of medical
writers. In the eighteenth century, taking to the waters became a fashionable
pastime for the wealthy classes who decamped to resorts around Britain and
Europe to cure the ills of overconsumption.
In the main, treatment in the heyday of the British spa
consisted of sense and sociability: promenading, bathing, and the repetitive
quaffing of foul-tasting mineral waters.
A hydropathic establishment is a
place where people receive hydropathic treatment. They are commonly built in
spa towns, where mineral-rich or hot water occurs naturally.
SOCIETY AND CULTURE
Several hydropathic institutions
wholly transferred their operations away from therapeutic purposes to become
tourist hotels in the late 20th century whilst retaining the name 'Hydro'.
There are several prominent examples in Scotland at Crieff,
Peebles and Seamill amongst others.
Canine hydrotherapy is a form of
hydrotherapy directed at the treatment of chronic conditions, post-operative
recovery, and pre-operative or general fitness in dogs.
(back
to content)
4.31 Myofascial release w
Myofascial release (MFR,
self-myofascial release) is an alternative medicine therapy claimed to be
useful for treating skeletal muscle immobility and pain by relaxing contracted
muscles, improving blood and lymphatic circulation, and stimulating the stretch
reflex in muscles.
Fascia is a thin, tough, elastic
type of connective tissue that wraps most structures within the human body,
including muscle. Fascia supports and protects these structures. Osteopathic
practice holds that this soft tissue can become restricted due to psychogenic
disease, overuse, trauma, infectious agents, or inactivity, often resulting in
pain, muscle tension, and corresponding diminished blood flow.
The use of myofascial release as
a treatment is not supported by good evidence; as a replacement for
conventional treatment for cancer, it risks causing harm.
Writing for Science-Based
Medicine, Harriet Hall described myofascial release as an umbrella term for
several types of physical manipulation, and it might more simply be described
as a kind of massage based on vaguely-defined scientific notions.
The American Cancer Society
states that "There is little scientific evidence available to support
proponents' claims that myofascial release relieves pain or restores flexibility"
and cautions Effectiveness against using it as a substitute for conventional
cancer treatment. The poor quality of research into the use of myofascial
release for orthopaedic conditions precludes any conclusions being drawn about
its usefulness for this purpose.
DESCRIPTION AND CONCEPTUAL BASIS
In 2011, the UK Advertising
Standards Authority (ASA) upheld a complaint regarding the effectiveness claims
published in an advertising leaflet produced by the Myofascial Release UK
health care service. The ASA Council ruled that materials presented by
Myofascial Release UK in support of the claims made in their ad were inadequate
to establish a "body of robust scientific evidence" to substantiate
Myofascial Release UK's range of claims. In addition, the ASA determined that
the ad breached advertising rules by introducing a risk that readers might be
discouraged from seeking other essential medical treatments.
Reviews published in 2013 and
2015 evaluating evidence for MFR efficacy found that clinical trials that had
been conducted varied in quality, technique, outcome measurements, and had
mixed outcomes; the 2015 review noted: "it is time for scientific
evidences on MFR to support its clinical use." Another review concluded
that the use of foam rollers or a roller massager before or after exercise for
self-myofascial release has been observed to decrease soreness due to DOMS and
that self-myofascial release appears to have no negative effect on performance.
However, the optimal timing and duration of use requires
further study.
The approach was promulgated as
an alternative medicine concept by Andrew Taylor Still, inventor of osteopathy,
and his early students. The exact phrase "myofascial release" was
coined in the 1960s by Robert Ward, an osteopath who studied with Ida Rolf, the
originator of Rolfing. Ward, along with physical therapist John Barnes, are
considered the two primary founders of Myofascial Release.
(back
to content)
4.32
Numerology w
Numerology is the
pseudoscientific belief in a divine or mystical relationship between a number
and one or more coinciding events. It is also the study of the numerical value
of the letters in words, names, and ideas. It is often associated with the
paranormal, alongside astrology and similar to divinatory arts.
Numerorum mysteria (1591), a treatise on numerology by
Pietro Bongo and his most influential work in Europe.
Despite the long history of
numerological ideas, the word "numerology" is not recorded in English
before c. 1907.
The term numerologist can be used
for those who place faith in numerical patterns and draw pseudoscientific
inferences from them, even if those people do not practice traditional
numerology. For example, in his 1997 book Numerology: Or What Pythagoras
Wrought, mathematician Underwood Dudley uses the term to discuss practitioners
of the Elliott wave principle of stock market analysis.
The practice of gematria,
assigning numerical values to words and names and imputing those values with
religious meaning, dates back to antiquity. An Assyrian inscription from the
8th century BC, commissioned by Sargon II. declares "the king built the
wall of Khorsabad 16,283 cubits long to correspond with the numerical value of
his name." Rabbinic literature used gematria to interpret passages in the
Hebrew Bible.
In 325 AD, following the First
Council of Nicaea, departures from the beliefs of the state church were
classified as civil violations within the Roman Empire. Numerology, referred to
as isopsephy, remained in use in conservative Greek Orthodox circles. Despite
the church's resistance to numerology, there have been arguments made for the
presence of numerology in the Bible and religious architecture.
Some alchemical theories were
closely related to numerology. For example, Persian-Arab alchemist Jabir ibn
Hayyan framed his experiments in an elaborate numerology based on the names of
substances in the Arabic language.
Numerology is prominent in Sir Thomas Browne's 1658 literary
Discourse The Garden of Cyrus.
Throughout its pages, the author attempts to demonstrate
that the number five and the related Quincunx pattern can be found throughout
the arts, in design, and in nature � particularly botany.
ALPHABETIC SYSTEMS
There are various numerology
systems which assign numerical value to the letters of an alphabet. Examples
include the Abjad numerals in Arabic, Hebrew numerals, Armenian numerals,
History Methods and Greek numerals. The practice within Jewish tradition of
assigning mystical meaning to words based on their numerical values, and on
connections between words of equal value, is known as gematria.
LATIN ALPHABET SYSTEMS
There are various systems of
numerology that use the Latin alphabet. Different methods of interpretation
exist, including Chaldean, Pythagorean, Hebraic, Helyn Hitchcock's method,
Phonetic, Japanese, Arabic and Indian.
ENGLISH QABALLA
English Qaballa (EQ) refers to a
system of Hermetic Qabalah that interprets the letters of the English alphabet
via an assigned set of values developed by James Lees in 1976. Like most of the
systems developed since the death of Aleister Crowley (1875-1947), it was
created with the intent of gaining a better understanding of the mysteries
elaborated in his inspired works, especially those in Liber AL vel Legis, the
Book of the Law. According to Jake Stratton-Kent, "the English Qaballa is
a qabalah and not a system of numerology. A qabalah is specifically related to
three factors: one, a language; two, a 'holy' text or texts; three,
mathematical laws at work in these two."
ABJAD SYSTEM
The Arabic system of numerology
is known as Abjad notation or Abjad numerals. In this system each letter of
Arabic alphabet has a numerical value. This system is the foundation of
ilm-ulcipher, the Science of Cipher, and ilm-ul-huroof, the Science of Alphabet:
ط= 9
ح= 8
ز= 7
و= 6
ه= 5
د= 4
ج= 3
ب= 2
أ= 1
ص= 90
ف= 80
ع= 70
س= 60
ن= 50
م= 40
ل= 30
ك= 20
ي= 10
ظ= 900
ض= 800
ذ= 700
خ= 600
ث= 500
ت= 400
ش= 300
ر= 200
ق= 100
غ= 1000
ARAB NUMEROLOGY
Some Chinese assign a different
set of meanings to the numbers and certain number combinations are considered
luckier than others. In general, even numbers are considered lucky, since it is
believed that good luck comes in pairs.
Traditional Chinese Medicine
(TCM), and its associated fields such as acupuncture, base their system on
mystical numerical associations, such as the "12 vessels circulating blood
and air corresponding to the 12 rivers flowing toward the Central Kingdom; and
365 parts of the body, one for each day of the year" being the basis of
locating acupuncture points.
CHINESE NUMBER DEFINITIONS
Cantonese frequently associate
numbers with the following connotations (based on its sound), which may differ
in other varieties of Chinese:
1. 一
[jɐ́t] � sure
2. 二
[ji̭ː] � easy 易 [ji̭ː]
3. 三
[s�ːm] � live 生 [s�ːŋ] but it
can also be seen as a halved eight when using Arabic numerals and so considered
unlucky.
4. 四
[sēi] � considered unlucky since 4 is a homophone with the word for death
or suffering
死
[sěi] (see tetraphobia), yet only in the Shanghainese, it is a homophone
of water (水) and is considered lucky because water is
associated with money.
5. 五
[ŋ̬] � the self, me, myself 吾 [ŋ̭], nothing,
never 唔 [ŋ, m] in the Shanghainese, it is a
homophone of fish (鱼)
6. 六
[l�ːk] � easy and smooth, all the way
7. 七
[tsʰɐ́t] � a slang/vulgar word in Cantonese.
8. 八
[pāːt] � sudden fortune, prosperity 發 [fāːt]
9. 九
[kɐ̌u] � long in time 久 [kɐ̌u], enough 夠
[kɐ̄u] or a slang/vulgar word derived from dog 狗
[kɐ̌u] in Cantonese
Some "lucky number" combinations include:
CHINESE NUMEROLOGY
99 � doubly long in time, hence eternal; used in the name of
a popular Chinese American supermarket chain, 99 Ranch Market.
168 � many premium-pay telephone numbers in China begin with
this number, which is considered lucky. It is also the name of a motel chain in
China (Motel 168).
888 � Three times the prosperity, means "wealthy
wealthy wealthy".
6 = U, V, 9
369 - 369=love
There is no assignment for the number 9. Numerologists
analyze double-digit numbers from 10 to 99.
In southern India, mostly Tamil Nadu, the numbers assigned
to English alphabets are the same as in the Chaldean system. The list is shown
below:
1 = A, I, J,
Q, Y
2 = B, K, R
3 = C, G, L,
S
4 = D, M, T
5 = E, H, N,
X
6 = U, V, W
7 = O, Z
8 = F, P
There is no assignment for the number 9. Numerologists
analyze double-digit numbers from 10 to 99.�
Ex: Number 29 is supposed to be the worst numbered-name a person can
have.
In Science
INDIAN NUMEROLOGY
Other uses of the term
Scientific theories are sometimes
labeled "numerology" if their primary inspiration appears to be a set
of patterns rather than scientific observations. This colloquial use of the
term is quite common within the scientific community and it is mostly used to
dismiss a theory as questionable science.
The best known example of
"numerology" in science involves the coincidental resemblance of
certain large numbers that intrigued such eminent men as mathematical physicist
Paul Dirac, mathematician Hermann Weyl and astronomer Arthur Stanley Eddington.
These numerical coincidences refer to such quantities as the ratio of the age
of the universe to the atomic unit of time, the number of electrons in the
universe, and the difference in strengths between gravity and the electric
force for the electron and proton. ("Is the Universe Fine Tuned for
Us?", Stenger, V.J.).
The discovery of atomic triads,
an early attempt to sort the elements into some logical order by their physical
properties, was once considered a form of numerology, and yet ultimately led to
the construction of the periodic table. Here the atomic weight of the lightest
element and the heaviest are summed, and averaged, and the average is found to
be very close to that of the intermediate weight element. This did not work
with every triplet in the same group, but worked often enough to allow later
workers to create generalizations.
Large number co-incidences continue to fascinate many
mathematical physicists.
Wolfgang Pauli was also fascinated by the appearance of
certain numbers, including 137, in physics
British mathematician I. J. Good wrote:
There have been a few examples of
numerology that have led to theories that transformed society: see the mention
of Kirchhoff and Balmer in Good (1962) ... and one can well include Kepler on
account of his third law. It would be fair enough to say that numerology was
the origin of the theories of electromagnetism, quantum mechanics,
gravitation.... So I intend no disparagement when I describe a formula as
numerological.
When a numerological formula is
proposed, then we may ask whether it is correct. ... I think an appropriate
definition of correctness is that the formula has a good explanation, in a
Platonic sense, that is, the explanation could be based on a good theory that
is not yet known but 'exists' in the universe of possible reasonable ideas.
(back
to content)
4.33
Orthopathy w
Orthopathy (from the Greek ὀρθός
orthos "right" and πάθος pathos
"suffering") or natural hygiene (NH) is a set of alternative medical
beliefs and practices originating from the Nature Cure movement. Proponents
claim that fasting, dieting, and other lifestyle measures are all that is
necessary to prevent and treat disease.
Natural hygiene is an offshoot of
naturopathy that advocates a philosophy of "natural living" that was
developed in the early nineteenth century. Natural hygienists oppose drugs,
fluoridation, immunization, most medical treatments and endorse fasting, food
combining and raw food or vegetarian diets.
19th century
The orthopathy movement
originated with Isaac Jennings in the 1820s, who practiced conventional
medicine for many years but became discouraged with its results. Jennings'
system was firmly opposed to all medicine and was known as the
"no-medicine plan". He prescribed bathing, rest and a vegetarian diet
as part of his system.
In 1837, Colonel John Benson,
Sylvester Graham and William Alcott founded the American Physiological Society
(APS) in Boston to promote Grahamism, which lasted just three years.
The APS was the first natural
hygiene organization in the United States. Mary Gove Nichols lectured for the
Ladies Physiological Society, an off-shoot of the APS. In the 1840s, Joel Shew
History and practice was influenced by the dieting ideas of Sylvester Graham
and promoted natural hygiene practices such as bathing, exercise and massage as
well as the elimination of alcohol and tobacco.
Isaac Jennings in his 1867 book
The Tree of Life, defined orthopathy as "from orthos, right, true, erect;
and pathos, affection. Nature is always upright�moving in the right
direction." George H. Taylor who introduced Swedish massage to the United
States in the 1860s was known to promote natural hygiene and physical culture.
Taylor believed that correct breathing and diet, gymnastics and mechanical
massage could replace medical intervention and restore health.
Natural hygiene was often associated with vegetarianism
during the nineteenth century.
However, not all natural
hygienists are vegetarians. Russell T. Trall was a notable early proponent of
natural hygiene and vegetarianism. Trall established his own version called
"hygeiotherapy", a mixture of hydrotherapy with diet and exercise
treatment regimes.
In 1887, Susanna Way Dodds and
her sister Mary established the Hygienic College of Physicians and Surgeons in
St. Louis, Missouri. They focused on "natural methods of treatment: diet,
exercise, massage, electricity and hydrotherapy in all of its manifold
applications".
During the 1880s, Thomas Allinson
developed his theory of medicine, which he called 'Hygienic Medicine.'
20th century
Natural hygienist George S. Weger managed Weger Health
School in Redlands, California (1923�1935).
Herbert M. Shelton who has been
described as "the twentieth century's premier natural hygienist", was
influenced by Sylvester Graham and Russell T. Trall. Shelton wrote much on the
topic, beginning with The Hygienic System: Orthopathy in 1939, which renamed
orthopathy as 'Natural Hygiene.'
Consumption of 'incompatible' foods
in one meal is said to lead to ill health, and consumption of 'compatible'
foods is said to maintain it: Shelton defined food combining and seven groups
of food, sorted by function as: supplying energy (carbohydrates, fats, and
proteins) needed to build the body (proteins, salts, and water) and regulating
bodily processes (minerals, vitamins, and water.)
White supremacist Ben Klassen was
influenced by Shelton and natural hygienic principles and promoted his own
"racial health" regimen known as Salubrious Living. However, Klassen
emphasised there were differences between his doctrine and the natural hygiene
movement as the latter did not focus on perpetuating the white race like his
regimen did. Klassen coauthored the book Salubrious Living with Arnold DeVries
in 1982.
Interest in natural hygiene was renewed in the 1980s
following publication of Fit for Life and Living Health by Harvey and Marilyn
Diamond.
ORGANIZATIONS
In 1948, the American Natural
Hygiene Society (ANHS) was founded by Herbert Shelton, William Esser, Gerald
Benesh, Christopher Gian-Cursio, Jesse Mercer Gehman, Irving Davidson, Jack
Dunn Trop and Symon Gould. In 1998, the ANHS became the National Health
Association.
In 1956, Keki Sidhwa established the British Natural Hygiene
Society (BNHS).
The International Association of
Hygienic Physicians was founded in 1978. The International Natural Hygiene
Society was founded in 2003 and has reported over 800 members.
CRITICISM
Medical experts consider natural
hygiene practices such as anti-vaccination, fasting and food combining to be
quackery. There is no scientific evidence that prolonged fasting provides any
significant health benefits. A prolonged fast may cause "anemia,
impairment of liver function, kidney stones, postural hypotension, mineral
imbalances, and other undesirable side effects."
Claims from natural hygienists
about fasting curing cancer are not supported by scientific evidence. According
to the American Cancer Society, "available scientific evidence does not
support claims that fasting is effective for preventing or treating cancer in
humans."
Founders
Isaac Jennings
�
Sylvester Graham
Joel Shew
�
George H. Taylor
Mary Gove Nichols
�Susanna Way Dodds
�
George S. Weger
(back
to content)
4.34
Radionics w
Radionics�also called
electromagnetic therapy (EMT) and the Abrams Method�is a form of alternative
medicine that claims that disease can be diagnosed and treated by applying
electromagnetic radiation (EMR), such as radio waves, to the body from an
electrically powered device. It is similar to magnet therapy, which also
applies EMR to the body but uses a magnet that generates a static
electromagnetic field.
Albert Abrams
|
�
|
The concept behind radionics originated with two books published
by American physician Albert
Abrams in 1909 and 1910. Over the
next decade, Abrams became a millionaire by leasing EMT machines, which he
designed himself. This so-called treatment contradicts the principles of
physics and biology and therefore is widely considered pseudoscientific. The
United States Food and Drug Administration does not recognize any legitimate
medical use for radionics devices.
Several systematic reviews have
shown radionics is no more effective than placebo and falls into the category
of pseudoscience.
Beginning around 1909, Albert
Abrams (1864�1924) began to claim that he could detect "energy
frequencies" in his patient's bodies. The idea was that a healthy person
will have certain energy frequencies moving through their body that define health,
while an unhealthy person will exhibit other, different energy frequencies that
define disorders. He said he could cure people by "balancing" their
discordant frequencies and claimed that his devices are sensitive enough that
he could tell someone's religion by looking at a drop of blood. He developed
thirteen devices and became a millionaire leasing his devices, and the American
Medical Association described him as the "dean of gadget quacks". His
devices were definitively proven useless by an independent investigation
commissioned by Scientific American in 1924. He used "frequency" not
in its standard meaning, but to describe an imputed energy type, which does not
correspond to any property of energy in the scientific sense.
RADIONIC INSTRUMENTS
HISTORY
In one form of radionics
popularised by Abrams, some blood on a bit of filter paper is attached to a
device Abrams called a "dynamizer", which is attached by wires to a
string of other devices and then to the forehead of a healthy volunteer, facing
west in a dim light. By tapping on his abdomen and searching for areas of
"dullness", disease in the donor of the blood is diagnosed by proxy.
Handwriting analysis is also used to diagnose disease under this scheme. Having
done this, the practitioner may use a special device known as an oscilloclast
or any of a range of other devices to broadcast vibrations at the patient in order
to attempt to heal them.
Other notable quack devices in radionics have included the
Ionaco and the Hieronymus machine.
Some people claim to have the
paranormal or parapsychological ability to detect "radiation" within
the human body, which they call radiesthesia. According to the theory, all
human bodies give off unique or characteristic "radiations" as do all
other physical bodies or objects. Such radiations are often termed an
"aura". Radiesthesia is cited as the explanation of such phenomena as
dowsing by rods and pendulums in order to locate buried substances, diagnose
illnesses, and the like. Radiesthesia has been described as a mixture of occultism
and pseudoscience by critics.
Modern practitioners
conceptualize these devices merely as a focusing aid to the practitioner's
proclaimed dowsing abilities, and claim that there is no longer any need for
the device to have any demonstrable function. Indeed, Abrams' black boxes had
no purpose of their own, being merely obfuscated collections of wires and
electronic parts.
Contemporary proponents of
radionics or EMT claim that where there is an imbalance of electromagnetic
fields or frequencies, within the body, that it causes diseases or other
illnesses by disrupting the body's chemical makeup. These practitioners believe
that applications of electromagnetic energy from outside the body can correct
these imbalances. Like magnet therapy, electromagnetic therapy has been
proposed by practitioners of alternative medicine for a variety of purposes,
including, according to the American Cancer Society, "ulcers, headaches,
burns, chronic pain, nerve disorders, spinal cord injuries, diabetes, gum
infections, asthma, bronchitis, arthritis, cerebral palsy, heart disease, and
cancer".
Another variant of radionics or EMT is magnetic resonance
therapy.
�
An original Rife machine from 1922
�An
"Electro-metabograph", an apparatus which supposedly diagnosed and
cured diseases by using radio waves
The claims for radionic devices
contradict the accepted principles of biology and physics. No scientifically
verifiable mechanisms of function for these devices has been posited, and they
are often described as "magical" in operation. No plausible
biophysical basis for the "putative energy fields" has been proposed,
and neither the fields themselves nor their purported therapeutic effects have
been convincingly demonstrated.
No radionic device has been found
efficacious in the diagnosis or treatment of any disease, and the U.S. Food and
Drug Administration does not recognize any legitimate medical uses of any
Scientific assessment such device. According to David Helwig in The Gale
Encyclopedia of Alternative Medicine, "most physicians dismiss radionics
as quackery".
Internally, a radionic device is
very simple, and may not even form a functional electrical circuit. The wiring
in the analysis device is simply used as a mystical conduit. A radionics device
does not use or need electric power, though a power cord may be provided,
ostensibly to determine a "base rate" on which the device operates to
attempt to heal a subject. Typically, little attempt is made to define or
describe what, if anything, is flowing along the wires and being measured.
Energy in the physical sense, i.e., energy that can be sensed and measured, is
viewed as subordinate to intent and "creative action".
Claims about contemporary EMT
devices are similar to those made by the older generation of
"radionics" devices, and are also not supported by evidence and are
also pseudoscientific. Even though some of the early works in
bioelectromagnetics have been applied in clinical medicine, there is no
relationship between alternative devices or methods that use externally applied
electrical forces and the use of electromagnetic energy in mainstream medicine.
The American Cancer Society says
that "relying on electromagnetic treatment alone and avoiding conventional
medical care may have serious health consequences". In some cases, the
devices may be ineffective and harmful.
REVIEWS
Several systematic reviews have shown EMT is not a useful
therapy:
In 2009 no significant difference
from control was found for management of pain or stiffness for osteoarthritis.
In 2011 a systematic literature
review on the use of pulsed electromagnetic field (PEMT) body mats used in a
wide range of conditions found insufficient evidence for them to be recommended
and recommended further high‐quality, double‐blind trials.
In 2014 insufficient for the efficacy of EMT as a therapy
for urinary incontinence.
In 2014 EMT was found to have no
difference from control for stimulation of bone growth in acute fractures.
In 2015 Cochrane Database of
Systematic Reviews found no evidence that EMT was useful in healing pressure
ulcers or venous stasis ulcers.
A 2016 guideline, in addition to
reviews in 2016, 2013 and 2022, did not find EMT useful for various forms of
pain.
The FDA has banned some
commercially available EMT devices. In 2008 the VIBE machine from Vibe
Technologies had a Class I recall that was completed in 2012.
Other ineffectual EMT therapy devices that have been
marketed include:
"BioResonance Tumor
Therapy", developed by Martin Keymer and purported to stimulate the P53
gene to cure cancer.
"Cell Com System", a
device created by Hugo Nielsen that is used on hands and feet to regulate
communications between cells in the body.
"Rife machine", a
device created by Royal Rife, which is also known as frequency therapy or
frequency generator and marketed as treating cancer.
"Zapping Machine", a
device created by Hulda Regehr Clark, claimed to cure cancer by using low-level
electrical current to kill parasites within the body that are supposed to cause
cancer.
"EMP Pad", a device
manufactured by EMPPad, advertised by Noel Edmonds, that is claimed to slow
ageing, reduce pain, lift depression and stress and tackles cancer.
"UVLrx", a device manufactured
by UVLrx Therapeutics that provides ultraviolet treatment of blood to treat
HIV/AIDS, Hepatitis C, Dengue fever and Lyme disease, as well as many other
conditions.
"ReBuilder", a device
manufactured by Rebuilder, is claimed to reverse neuropathy (nerve damage) by
using tiny electrical signals to wake up nerves.
"Electro Physiological
Feedback Xrroid (EPFX)", a device manufactured by Desir� Dubounet that is
claimed to cure cancer, as well as other serious conditions by sending
electromagnetic frequencies into the body.
(back
to content)
4.35 Urine therapy w
Urine therapy or urotherapy, (also urinotherapy, Shivambu,
uropathy, or auto-urine therapy) in alternative medicine is the application of
human urine for medicinal or cosmetic purposes, including drinking of one's own
urine and massaging one's skin, or gums, with one's own urine.
Drinking or local application of human or animal urine for
medicinal purposes has been practiced all over the world for millennia.
Urine therapy
Alternative
medicine
Claims ������������������������������������������������� Various
therapeutic uses of urine.
Related fields ����������������������������������� Naturopathy
HISTORY
Though urine has been believed
useful for diagnostic and therapeutic purposes in several traditional systems,
and mentioned in some medical texts, auto-urine therapy as a system of
alternative medicine was popularized by British naturopath John W. Armstrong in
the early 20th century. Armstrong was inspired by his family's practice of
using urine to treat minor stings and toothaches, by a metaphorical reading of
the Biblical Proverb 5:15 "Drink waters out of thine own cistern, and
running waters out of thine own well", and his own experience with
ill-health that he treated with a 45-day fast "on nothing but urine and
tap water". Starting in 1918, Armstrong prescribed urine-therapy regimens
that he devised to many thousands of patients, and in 1944 he published The
Water of Life: A treatise on urine therapy, which became a founding document of
the field.
Armstrong's book sold widely, and in India inspired the
writing of Manav mootra (Gujarati: Urine therapy; 1959) by Gandhian social
reformer Raojibhai Manibhai Patel, and many later works.
These works often reference
Shivambu Kalpa, a treatise on the pharmaceutical value of urine, as a source of
the practice in the East. They also cite passing references to properties and
uses of urine in Yogic-texts such as Vayavaharasutra by Bhadrabahu and Hatha
Yoga Pradapika by Svatmarama; and Ayurvedic texts such as Sushruta Samhita,
Bhava Prakasha and Harit. However, according to medical anthropologist Joseph
Atler, the practices of sivambu (drinking one's own urine) and amaroli
recommended by modern Indian practitioners of urine therapy are closer to the
ones propounded by Armstrong than traditional ayurveda or yoga, or even the
practices described in Shivambu Kalpa.
Urine-therapy has also been combined with other forms of
alternative medicine including Ayurveda
MODERN CLAIMS AND FINDINGS
An exhaustive description of the composition of human urine
was prepared for NASA in 1971.
Urine is an aqueous solution of
greater than 95% water. The remaining constituents are, in order of decreasing
concentration: urea 9.3 g/L, chloride 1.87 g/L, sodium 1.17 g/L, potassium
0.750 g/L, creatinine 0.670 g/L and other dissolved ions, inorganic and organic
compounds.
In China there is a Urine Therapy Association which claims
thousands of members.
According to a BBC report, a Thai
doctor promoting urine therapy said that Thai people had been practicing
urophagia for a long time, but according to the Department of Thai Traditional
and Alternative Medicine, there was no record of the practice.
Urinating on jellyfish, wasp or
bee stings, sunburns, cuts, and blood vessel bursts is a common "folk
remedy", however Scientific American reports that it may be
counterproductive, as it can activate nematocysts remaining at the site of the
sting, making the pain worse.
Urine and urea have been claimed
by some practitioners to have an anti-cancer effect, and urotherapy has been
offered along with other forms of alternative therapy in some cancer clinics in
Mexico.
In the Arabian Peninsula, bottled
camel urine is sold by vendors, as prophetic medicine with its claimed urine
therapy, health benefits. Saudi police arrested a man, "because the urine in
the bottles was his own".
In January 2022, Christopher Key,
a spreader of COVID-19 misinformation, claimed that urine therapy is the
antidote to the COVID-19 pandemic. Key also falsely claims that a 9-month
research trial on urine therapy has been conducted. There is no actual
scientific evidence supporting urine therapy as a cure to the COVID-19 disease.
HEALTH CONCERNS
According to the American Cancer
Society, "available scientific evidence does not support claims that urine
or urea given in any form is helpful for cancer patients".
In 2016 the Chinese Urine therapy
Association was included on a list of illegal organizations by the Ministry of
Civil Affairs. However, the Municipal Bureau of Civil Affairs in Wuhan, said
they had no jurisdiction over the association.
A study on bacterial isolates
contained in the urine of Nigerian children and cows found a significant
presence of antibiotic-resistant pathogen strains, including E. coli, Shigella,
and Salmonella. The study concluded that these pathogens may be introduced into
the body through urine consumption, most notably through the traditional urine
therapy treatments conducted by some local individuals.
(back
to content)
4.36
Wellness (alternative
medicine) w
Wellness is a state beyond absence of illness but rather
aims to optimize well-being.
THE EIGHT DIMENSIONS OF WELLNESS
The notions behind the term share
the same roots as the alternative medicine movement, in 19th-century movements
in the US and Europe that sought to optimize health and to consider the whole
person, like New Thought, Christian Science, and Lebensreform. Ayurveda
mentions the concept and also has dedicated a whole speciality for the concept
of wellness and maintenance of health.
The term wellness has also been misused for pseudoscientific
health interventions.
HISTORY
The term was partly inspired by
the preamble to the World Health Organization�s 1948 constitution which said:
�Health is a state of complete physical, mental and social well-being and not
merely the absence of disease or infirmity.� It was initially brought to use in
the US by Halbert L. Dunn, M.D. in the 1950s; Dunn was the chief of the
National Office of Vital Statistics and discussed �high-level wellness,� which
he defined as �an integrated method of functioning, which is oriented toward
maximizing the potential of which the individual is capable.� The term
"wellness" was then adopted by John Travis who opened a
"Wellness Resource Center" in Mill Valley, California in the
mid-1970s, which was seen by mainstream culture as part of the hedonistic
culture of Northern California at that time and typical of the Me generation.
Travis marketed the center as alternative medicine, opposed to what he said was
the disease-oriented approach of medicine. The concept was further popularized
by Robert Rodale through Prevention magazine, Bill Hetler, a doctor at
University of Wisconsin�Stevens Point, who set up an annual academic conference
on wellness, and Tom Dickey, who established the Berkeley Wellness Letter in
the 1980s. The term had become accepted as standard usage in the 1990s.
In recent decades, it was noted
that mainstream news sources had begun to devote more page space to "health
and wellness themes".
The US Substance Abuse and Mental
Health Services Administration uses the concept of wellness in its programs,
defining it as having eight aspects: emotional, environmental, financial,
intellectual, occupational, physical, social, and spiritual.
CORPORATE WELLNESS PROGRAMS
By the late 2000s, the concept
had become widely used in employee assistance programs in workplaces, and
funding for development of such programs in small business was included in the
Affordable Care Act. The use of corporate wellness programs has been criticized
as being discriminatory to people with disabilities. Additionally, while there
is some evidence to suggest that wellness programs can save money for
employers, such evidence is generally based on observational studies that are
prone to selection bias. Randomized trials provide less positive results and
often suffer from methodological flaws.
The discrimination of disabled
people in corporate wellness programs was one of the many reasons that prompted
the creation of the Americans with Disabilities Act of 1990. Under the newly
proposed Americans with Disabilities Act rule, an employee-wellness program
consists of programs that relates to health promotion or disease prevention
that includes disability-related inquiries or medical examinations. There are
two types of wellness programs that are under the Americans with Disabilities
Act: Participatory and Health-contingent. This newly proposed rule no longer
contains the requirement that such programs be reasonably designed to promote
health or prevent disease.
CRITICISM
PROMOTION OF
PSEUDOSCIENCE
Wellness is a particularly broad
term, but it is often used by promoters of unproven medical therapies, such as
the Food Babe or Goop. Jennifer Gunter has criticized what she views as a
promotion of over-diagnoses by the wellness community. Goop's stance is that it
is "skeptical of the status quo" and "offer[s] open-minded
alternatives." Michael D. Gordin writes that pseudoscience is a bad
category for analysis because it exists entirely as a negative attribution that
scientists and non-scientists hurl at others but never apply themselves.
Pseudoscience is typically used to describe something that looks like science,
but is somehow false, misleading, or unproven. Things that fall under the
pseudoscience umbrella consists of: astrology, phrenology, UFOlogy,
creationism, and eugenics.
HEALTHISM
Wellness has also been criticized
for its focus on lifestyle changes over a more general focus on harm prevention
that would include more establishment-driven approaches to health improvement
such as accident prevention. Petr Skrabanek has also criticized the wellness
movement for creating an environment of social pressure to follow its lifestyle
changes without having the evidence to support such changes. Some critics also
draw an analogy to Lebensreform, and suggest that an ideological consequence of
the wellness movement is the belief that "outward appearance" is
"an indication of physical, spiritual, and mental health."
The wellness trend has been criticized as a form of
conspicuous consumption.
(back
to content)
4.37 History of Reflexology w
1.1. The very beginning of
reflexology history according to ancient Chinese records, Buddhist monks
brought early reflexology from India to China about 5000 years ago.
1.2. Just under 5000 years ago
many ancient Chinese books talk about techniques that are similar and sometimes
identical to modern reflexology eg. they practiced the "examining foot
method".
1.3. There are also many
references in a treasured ancient text called �The Great Yellow Emperors
Medical Book� (The Inner Cannon, The Classic of Internal Medicine).
1.4. The information in this text
is still used by Traditional Chinese Medicine Practitioners all over the world
today.
1.5. 4000 years ago there is
evidence of some form of foot and hand therapy being practiced in Egypt as
depicted in the tomb of Ankmahor. Found in the tomb of Egyptian Vizier (second
in charge after the king) Ankhmahor, were many pictures of different
tradespeople, people making jewelry and craftsman.
1.6. In the room dedicated to
medical pictures they found one of the people practicing something that looks a
lot like reflexology.
1.7. One man having his feet
receiving reflexology, another his finger. Underneath the picture is this
writing, (rough translation) the patient is saying "do not cause
pain" and the physician replies "I will give you only pleasure"
1.8. The North American tribes of
the First Nation People are known to have practiced a form of foot therapy for
hundreds of years.
1.9. The dictionary definition of
a �Reflex� is �an involuntary or instinctive movement in response to a
stimulus� or in the sense of reflection or mirror image.
1.10. The reflexes on our feet
and hands act as mirror images of the body�s � a microcosm of the whole body.
1.11. Zone Therapy was used as
far back as 1500 AD. The re-discovery of some form of systemised foot treatment
is accredited to Dr William Fitzgerald who called it Zone Therapy and drew it
to the attention of the medical world between 1915 and 1917.
1.12. During the 16th Century a
number of books were published on Zone Therapy, one was written by Dr Adamus
and Dr A�tatis and another by Dr Ball in Leipzig.
1.13. The first use of the word
�reflex� with reference to motor reactions was used by the German physiologist
Johann August Unzer in 1771. In 1883 Marshall Hall, an English physiologist
introduced the concept and term �reflex action�.
1.14. In the late 1880s,
neurology as a branch of science became a field of its own. Often articles
regarding the most up-to-date research on reflex action were published in
England in �Brain� - a Journal of Neurology. One article �Reflex Action as a
Cause of Disease and Means of Cure� by Dr. T. Lauter Brunton discussed the
beneficial use of inducing a blister on the skin for the healing of internal
problems.
1.15. Sir Henry Head (an English
physiologist) was able to chart areas according to the spinal segment to which
they belonged. After years of research he established the Head zones, which are
labeled in anatomy books today as dermatomes. Head�s work conclusively proved
the neurological relationship that exists between the skin and the internal
organs.
1.16. The Russians pursued the
study of reflexology both from the psychological and physiological point of
view. Russian work with reflexes began with Ivan Pavlov�s (1849-1936) theory of
conditioned reflex response which earned him the Nobel Prize in 1904. His
famous theory was a reflex action was a simple and direct relationship between
a stimulus and a response (the ringing of a bell and a dog salivating).
1.17. It was in 1915 that an
article entitled �To stop that toothache, squeeze your toe� was published in
�Everybody�s Magazine�, written by Edwin Bowers, which first brought Dr
Fitzgerald�s work on Zone Therapy before the public.
1.18. In 1917, Dr Fitzgerald
wrote �Zone Therapy or Relieving Pain in the Home�. Two years later, they
enlarged this book and published it under a second title �Zone Therapy or
Curing Pain and Disease�.
1.19. Dr William Fitzgerald (1872
� 1942) received his medical degree from the University of Vermont in 1895. He
practiced in Boston City Hospital for two and a half years before going to
London where he spent two years at the Central London Nose and Throat hospital
before taking up a position in Vienna as Assistant to Professors Politzer and
Chiari, who were highly respected doctors.
1.20. Dr Ada Politzer (1835 �
1920) of the University of Vienna, was a wellLEARN 1.21. Dr Fitzgerald never
published the original sources for his own therapy, but it is likely that he
was influenced during this time in Vienna, by the work of Dr d�Arsonval. In
�Zone Therapy is Scientific� by Dr W D Chesney, it is stated that in Germany,
Dr d�Arsonval was using physiotherapy and getting relief following the use of
reflex knowledge, which, in effect, was what was later termed Zone Therapy by
Drs Fitzgerald and Bowers.
1.22. When Dr Fitzgerald returned
to the United States, he became head of the Nose and Throat Department at St
Francis Hospital, Hartford, Connecticut. Around 1909, Dr Fitzgerald discovered,
or re-discovered Zone Therapy. Almost ten years later.
1.23. Dr Fitzgerald wrote his
book, about how he had stumbled upon the concept of Zone Therapy: �Six years
ago I accidentally discovered that pressure with a cotton tipped probe on the
muco-cutinous margin (where the skin joins the mucous membrane) of the nose
gave an anesthetic result as though a cocaine solution had been applied. I
further found that there were many spots in the nose, mouth, throat and on both
surfaces of the tongue, which, when pressed firmly, deadened definite areas of
sensation. Also, that pressure exerted over any bony eminence of the hands,
feet or over the joints, produces the same characteristic results in pain
relief. I found also that when pain was relieved, the condition that produced
the pain was most generally relieved. This led to my �mapping out� these
various areas and their associated connections and also to noting the
conditions influenced through them. This science I have named �Zone Therapy�.
1.24. It is worth noting that the
Chinese had, in Acupuncture, divided the body into longitudinal Meridians by
approximately 2,500 B.C.
1.25. The physiotherapist working
with Dr Riley at St Petersburg, was Eunice Ingham (1889 � 1974). Eunice Ingham
extended the work of Dr Fitzgerald and painstakingly mapped the feet with all
the corresponding organs and glands of the body. She was a real pioneer who was
determined to help people to help themselves, if their doctor was not using
reflexology. In the early years, she worked with doctors to prove her findings
and to demonstrate to them that reflexology was a useful diagnostic tool.
1.26. She lectured at a medical
clinic headed by Dr Charles Epstein in May 1939. In his report, he acknowledged
that reflexology worked. However, while they knew it worked, doctors were not
interested in using it, because reflexology was too time consuming and they
could not make as much money.
1.27. Eunice Ingham is still
known as the pioneer of modern reflexology and she authored two well-known
books �Stories the Feet Can Tell� and �Stories the Feet Have Told�. They have
since been combined into one volume. In addition to her writing and lecturing,
she, along with her nephew, Dwight Byers, founded the International Institute
so that her work could be continued in perpetuity.
1.28. Throughout her forty years
of experience treating many thousands of people, Eunice Ingham devised a system
of techniques which enable the practitioner to contact the reflexes in the most
effective and economic way. This system is known as the �Original Ingham
Method�
1.29. Eunice Ingham died in 1974,
having devoted forty years of her life to reflexology.
(back
to content)
5.0 History of Natural Medicine z
The Universe is the matter part
of Existence, which is divided into realms, where angels were in charge of
taking care of spirits and spirits were in charge of direct care of nature,
which was what Devil revolted against to control what spirits were in charge of
because he was already in charge of spirits. That caused the fall, as sprits
were cut off, so the body will be in charge of the physical. Before the fall of
humankind from paradise to good and evil where nakedness was not knowing
anything about emotions, where the part of evil connected to the darkness seen
in the Universe without the Sun shining that brought in sickness, humanity were
kept pure without the contaminations of the Universe that were from
micro-organisms that were only surviving in the Universe. Humans lived in
spirit, where they Willed whatever they wanted and did not die but instead
translated when their spirit mission was completed; the problem with the spirit
cutoff after the fall of humankind was that the mission of the person that is
born to earth is not known to the person as the person is only of emotions and
carnal form, which made the person vulnerable to the activities of the Universe
that the soul and physical body were from.
The spirit is not from the
Universe, but the spirit force is what was used to create the Universe that is
dark and harbours darkness, which is always related to a spirit part; no part
of darkness is not connected to or from a spirit part that is light. It is
because of the choice of good and evil that the spirit was cut off, which
without the spirit, the darkness or evil part of a human or animal or plant
will not be regulated. Good and evil are respectively, the back brain and the
front brain; the front brain is for matter to do materialism, while the back
brain is for the spirit, and the mid brain connects the soul with the endocrine
system to give emotions. The highest being in a planet chose the path of this
world, even though the Carnal form of the Devil was not from this planet. The
Devil�s descendants have spread around the planet as the dominant race, who have
redefined the way of the earth to what made their ancestors world collapse; the
flood only reduced them from being a thousand times the descendants of Adam,
there are different flood stories of survival that shows it is not Noah alone
in the Bible that survived. They bruise their head by speculating, and the rest
of humanity bruise their heal by activity for the system. Light does not mean
white, light means bright. �
|

|
The ancient dark skinned before
the aliens intervention that caused God to cut off spirit activity, was that
they feel their environment from their spirit via their soul; the military
feeling of environment now is only by soul, but the traditional black Chiefs
and Chief priests still feel from their spirit because of the prayers of the
people and himself before his coronation that allows God to let his ancestors
spirit guide him, unless he prays for his own way as was intended by God, then
his spirit opens to let him read by download of information into his brain.
That was why the moors that Sub-Saharan Africa of West-Central Africa were
known by the half-breed half-caste were known where the people who had to teach
the ancestors of the future colonialists how to bathe regularly, cook the
different species of the edible plants etc. they were not used to, but because
of inferiority complex and the will to dominate the earth as their alien patenal
ancestors did materially in their own star system that made them carnal, which
annoyed God to curse the original point of the land of the Garden of Eden that
anyone can see how the indigenes in those places in Nigeria into the Cameron do
not agree to solve anything which is what lets migration occur and allowed
colonialists who came in and siezed the land as the inhabitants princes etc.
were fighting over power that left thier land unprotected. So for the
colonialists to dominate in leadership and in resources control, they had to
divide and conquer by going after the system Sub-Saharan Africans relied on
most that was their traditional medicines which kept them alive and going after
the fall; although most of the dark skinned never knew that it was because of
the white skinned that paradise that was their spiritual way of doing things
was lost, as they embraced them to like foreign goods because of the moors who
went there and exchanged or did trade by batter to look more advanced. But the
colonialists stigmatized their medicines to sell theirs by imposing it on the
colonial African doctors they brought up using the mistakes of some traditional
medicines practitioners to look like the norm for Sub-Saharan Africans
medicinal practice, which those who believed them paid with their lives because
Medicine is best with the addition of the indigenous medicine in addition to
the better practice, and not discarding herbs that are indigenous to your body
formation to use herbal or synthetic products from lands that are different
from your genetical structure that treatment will not last for long like the
one from your area.
There was a super continent
called Pangea that had all the continents as one with four different species of
humanoid, then the continents broke up and the homo sapiens were left in
Gondwana-land, then South America and India broke up from it with the homo
sapiens that mingled with the races they met when their land joined the other
lands that broke from Pangea to produce the natives of the Americas and Asia
(that left separating religion as spirituality from medicine since it was
cursed). But Africa remained as the Garden of Eden and original point of
humanoid origin when it was Pangea. It was when Gondwana-land existed that the
aliens that were shining because of their active being had coitus with the
Indian that was the first of the Asian human races, but not the first of what
remained as Africa. So the first man to know his spirit had other helpers that
were humans before he was the first person to have a woman that was formed with
his own spirit and soul, which the rest of the world was made to copy to make
them human beings, as his alien-half-cast son from his wife's sin killed the
full human brother and fled to the east of Asia to form present day Georgia
where Greece came from, and Rome came from Greece until they became nine
countries that came from Cain, which the ninth Country called Britain formed
the tenth Country called USA that its systems was different from every other,
but the three systems that came out of it dominated the world as democracy,
judiciary and the financial system.
The real forbidden fruit was Eve
producing her first descendant from a man from Andromeda Galaxy that had older
stars from Galaxies that collapsed to form it as the galaxy is younger than
Earth, yet a little bigger than our Milky Way. It should have been strange to
any scientific mind, why the calendar of human civilization was forced to the
period from the beginning of the fall of humans to good and evil, which is
about seven thousand years, rather than the period of the origin of Eden, which
is millions of years. The reason for this is that half of their genes came from
around the Sirus star system in Andromeda Galaxy. Aliens and humans pray to the
same God. It was the sin that is fornication of the alien that was the Devil
that made God curse stop the interaction of aliens and humans because the
aliens that come to Earth see the curse of God on the disobedient, where
earthlings are carnal now, without true spirituality as it is by only emotional
excitement of the spirit in prayer that they live as worship rather than full
activity of the spirit because God cut the way to the spirit with an angel
guiding every way to it in everyone, but anyone can reach and connect with
their spirit by praying to God in truth that they want to be as God and that
person agreed before his/ her spirit descended into the soul that descended
into the foetus in the form that meets it's conditional needs to achieve it's
divine purpose. Which most stray from because their mind is more on material
things and needs than their spiritual purpose that they are supposed to bring
to harmony in practice on Earth. It is the sense of posture as professionals,
which they learnt from the moors of west-Africa that the colonialists imbibed
in their colonialists trained that made them appear feeling academically
professionals, when the whites kept reading to become true academic doctors and
not just remaining with the professional courtesy of doctor in waiting as
resident that was allowed as a bachelor degree holder to use the final training
title status. Getting the world from the Devil is getting the world back to the
original descendants of the earth, by having all systems, especially Medicine
to be taken by the original pure species.
The fall of humankind cursed the
Garden of Eden with the centre now called Nigeria that triggered the Sahara Desert
to erase all vegetation, which caused humans to migrate to the Middle East
where the Sumerian civilization began learning how to do things physically
without spirit. As religion grew, those that could tap into the metaphysical
more than others were deemed heretic and persecuted, even though those who did
the persecution were led by metaphysicians that belonged to a religion, who
were actually persecuting those who were not subject to their doctrine. The
melanin recessive were easily moved by their Andromeda galaxy force to be
hostile to those of the Milky Way as both galaxies were on a path of collision
to become one, so it was all a good and evil of two galaxies becoming one, where
the dominant specie dictates the system of the union of both galaxies. I write
about period and time, because there was a period before time measurement of
life or activity that has to do with spiritual activity of beings using the
garment of skin and a later time where good and evil caused an elapse of time.
The allopathic belief is that the traits of a child are from the parents alone
and the parents are from different persons that are different families; the
truth is that genuine divine husband and wife have bodies from different
parents, but with seperated soul and same spirit; but the children are only
related to the parents by their physical body, as their soul and spirit are for
another person for them to do what God sent them to do.
In the period of good and evil
that the colonial medicine established itself by force, they introduced a
scientific system based on the garment of skin that was against the origin of
mankind that had to do with the spirit of humankind that was like God and was
the only part that could communicate directly with God, which was what the
early black skinned Africans as the origin of the human race were partly
connected to as humankind were cutoff. That was where they were able to
spiritually see the herbal, animal, or material products with the dosage of
herbal and chemical prescriptions they prescribed. At the time of the
renaissance of the occidentals, they had alchemists who had learnt this system
from Africans like Amunotep that when their carnal nature could not pass than
the spiritual and emotional connectivity to natural healing, they formed
scientific bodies to change the meaning of science from spiritual, emotional
and physical knowledge to only physical knowledge that they chose to replace
the original science that encompassed all forms of the human being with the
carnal form of knowledge perfected in wars by cadaver study as anatomy.
���������������
|
|
The spiritual rise of the spirit of mankind, is
not in circles about a particular thing or way on earth, but a spirial rise
of the spiritual person in the mind to his point of spiritual origin, because
it is the spirit that keeps the body alive that has a purpose and not the
body that learnt the way of the world to work for the world to be as good and
evil was designed by the Devil to upgrade into more materialism but, to
upgrade into more spirituality.
|
The old ways of medicine was that
the intending applicant to be a doctor must be spiritual for the native doctor
to pass down his knowledge to, if he or she was not spiritual to develop
telepathy, the native doctor rejects the intending student; that was why the
Occidental medical practice dumped spirituality since many who could study
medicine were not spiritual or metaphysical to be alchemist. Since then,
medicine became only carnal and the emotional and spiritual side of it that
makes it holistic disappeared and medical practice remained colonial, which
rejected indigenous medicine to make medical doctors marketers of foreign drugs
they prescribe, while their council constitution tells them not to do so. What
hypocrisy. After Lucifer deception on humans to choose good and evil to be
wise, it took over 6,000 years for generational change for humans to become
wise carnally. That does not mean we should abandon the spirit, but we should
seek it for God to make us from image to be like gods as He said before
creating humans. We are supposed to live by our intuition assisted by our
intellect and not the reverse that the present scientific teaching portrays on
students to take them away from their spirit that knows the truth of science
more than the body and emotions can ever understand to do. That is the only way
to have technology beyond any species on Earth but equal or more than the most
civilized aliens in the Universe that commune by telepathy of the soul.
�
|

|
The old ways of knowing before
writing was needed to transfer information because the human had lost its
�being� nature to be using its intellect alone that made them not to be truly
human beings, was like the internet cloud of the mind where information can
only be tapped by the celeberum of the brain through the solar plexus
connection of the spirit. The intellect is the front and mid brain use alone
without the hind brain that makes the human being because of the use of the
spirit. To connect to the spirit is to ask God by your intention to be as your
spirit came to be in the/ your body from inception of the formation of the
foetus that will allow God remove the angel blocking everywhere to the tree of
life that is your spirit, for you to be of charisma and absolute intelligence
and knowledge that is like gods. In colonal conventional medicine, the pons has
no meaning because they threw away the way of the spirit, but in holistic
medicine where the spirit is also involed, the pons is the main bridge holding
the soul to the brain for the interaction of the spirit via the medulla obonglata.
The healing of any patient cannot be complete without the complete use of the
full potential of the person that includes the body, soul and spirit. The
spirit is housed by the soul to be able to operate in materialism, while the
body houses the soul to operate in matter.
(back
to content)
6.0
Physicians c
Physicians diagnose diseases and
injuries, administer treatment, and advise patients on good diet and other ways
to stay healthy. The United States has two kinds of physicians, the Doctor of
Medicine (MD) and the Doctor of Osteopathy (DO). Both use medicines, surgery,
and other standard methods of treating disease. DOs place special emphasis on
problems involving the musculoskeletal system, which includes muscles, ligaments,
bones, and joints.
Patients receive medical care
from primary care doctors and specialists. Primary care doctors include general
practitioners, family physicians, general internists, and general
pediatricians. Many women also use obstetricians-gynecologists as primary care
doctors. Patients usually consult a primary care doctor when they first become
ill or injured. Primary care physicians can treat most common disorders, and
provide comprehensive, lifelong care for individuals and families.
But medical knowledge has
advanced so far that no physician can master an entire field of medicine.
Primary care doctors may refer patients with unusually complicated problems to
specialists with advanced training in a particular disease or field of
medicine. Specialists may even concentrate in one particular area, and become
subspecialists. Each specialist in internal medicine, for instance, is an
expert in diagnosis and nonsurgical treatment of adult diseases. But some
internists take advanced training to become subspecialists in treating
adolescents, heart disease, elderly people, cancer, or arthritis. For more
information about the areas that specialists treat, see the table on Medical
Specialties.
OTHER HEALTH
PROFESSIONALS c
Medicine is not restricted to physicians. A wide variety of health care
practitioners work in this exciting field. By far the largest professional
group is nurses. Registered nurses help physicians during examinations,
treatment, and surgery. They observe, evaluate, and record patients� symptoms,
administer medications, and provide other care (see Nursing). Nurse
practitioners perform basic duties once reserved for physicians, such as
diagnosing and treating common illnesses and prescribing medication. Certified
nurse-midwives care for mothers during pregnancy and deliver babies (see
Midwifery). Nurse-anesthetists administer anesthesia to patients during
surgery. Licensed practical nurses provide basic bedside care for sick patients
under the supervision of registered nurses and physicians.
Physician assistants deliver
basic health services under the general supervision of a physician. They
examine patients, order X rays and laboratory tests, and prescribe drugs or
other treatment. In some rural areas, physician assistants provide all basic health
care for patients, consulting with a supervising physician by telephone or
electronic mail.
Dentists diagnose, treat, and
help prevent diseases of the teeth, gums, and other tissues in the mouth and
jaws (see Dentistry). Most are general practitioners, but many specialize in a
particular area of dental health. Orthodontists treat teeth that are poorly
aligned; oral surgeons operate on the jaw and mouth; periodontists specialize
in gum disease; pediatric dentists care for children; endodontists perform root
canals; prosthodontists make and insert artificial teeth and dentures. Other
dental professionals include dental hygienists who assist dentists in surgery,
clean teeth, and provide fluoride treatments. They advise patients on proper
oral hygiene techniques to prevent tooth and gum disease.
For more information about other health care practitioners,
see the table on Allied Health Professionals.
HEALTH CARE
FACILITIES c
A sick or injured person can obtain medical care in several different
places. These include provider practices such as medical offices and clinics,
hospitals, nursing homes, and home care.
There are about 200,000 medical
offices, clinics, and other provider practices in the United States. Earlier in
the 20th century most physicians were solo practitioners working in their own
offices or in partnership with another doctor. Patients visited the office,
received an examination or other service, and paid a fee. This traditional
solo, fee-for-service medicine has been declining. Many physicians now practice
in groups where they share the same offices and equipment with other doctors.
Group practices may combine primary care physicians, several kinds of
specialists, laboratories, and equipment for diagnosing disease. Physicians who
practice in a group reduce their own expenses and provide patients with a wider
range of services.
Many doctors are joining with
hospitals, insurance companies, and industrial employers to provide managed
care for groups of patients. Physicians may work as employees of health
maintenance organizations (HMOs) or other health care alliances. These plans
oversee, or manage, care for patients, to avoid unnecessary services and reduce
costs. Rather than taking a fee from each patient, managed care physicians may
receive an annual salary from the HMO or a fixed sum for each patient.
Patients who are too sick for
care in a doctor's office go to a hospital. Hospitals offer patients 24-hour
care from a staff of health professionals. They provide services not available
elsewhere, such as major surgery, child birth, and intensive care for the
critically ill. The United States has about 6,020 hospitals including more than
1 million beds. Several kinds of hospitals exist, including general hospitals,
specialized hospitals that care for specific diseases, small community
hospitals, and large academic medical centers that train new doctors. Hospitals
also provide many outpatient services to patients being treated in doctors'
offices and clinics. These include laboratory tests, computerized imaging
scans, X rays, and other diagnostic tests for people who do not require
admission to the hospital.
Hospital care is the most
expensive form of health care. Efforts to control health care costs have
emphasized reducing the number of patients admitted to hospitals and their
length of stay. During the 1980s and 1990s, these efforts led to the closing of
more than 600 hospitals, which eliminated almost 200,000 beds. Physicians also
try to treat more people on a nonhospital, or outpatient, basis, and these
cost-control efforts have led to fast growth in outpatient treatment centers.
These include ambulatory surgery centers, where patients undergo operations
once available only in hospitals and return home the same day.
Patients who need long-term medical
care because of advanced age or chronic illness may stay in a nursing home. The
United States has about 17,000 nursing homes with about 1.8 million patients.
The number of nursing homes has doubled since 1960 because there are more older
people in the population. Changing lifestyles, in which adult children and
parents often live far apart, also contributed to the need for more nursing
homes. About 85 percent of nursing home patients are age 65 and over. Many stay
for a few weeks while recovering from an acute illness. They receive medical
care and help with everyday activities like eating, bathing, and using the
bathroom. Then they return home and care for themselves, often with the help of
family or other caregivers. Other patients stay longer.
Some patients need regular
medical care and other assistance, but are not sick enough for a hospital or
nursing home. Home health care allows them to receive skilled nursing and other
care in their own homes. Home care services are the fastest-growing sector of the
health care industry, increasing about 30 percent per year in the 1990s. This
growth is largely because home care is less expensive than hospital or nursing
home care. Home care also is very popular with patients because most people
prefer staying at home, rather than entering a hospital or nursing home. About
15,000 home health agencies provide most home care services in the United
States. Many agencies are privately owned. Hospitals, public health
departments, and other organizations also offer home care.
Hospices are special health care
facilities that provide care for dying patients in the final stages of a
terminal illness. A hospice staff is focused on making the last days of a dying
patient pain free and comfortable. Many patients choose hospice services in
their homes.
Research is one of the most important fields of medicine. It
provides health care professionals with new knowledge and technology for better
diagnosis, treatment, and prevention of disease.
Medical research often combines
medicine with related fields of biology, and is called biomedical research.
Research can be basic or applied. Basic, or fundamental, research has no
immediate practical application. Basic cancer research, for instance, may try
to identify gene mutations that turn a healthy cell malignant. While this
information does not have immediate clinical value, it generates knowledge that
often leads to better care for patients. Applied research has a specific
practical goal, such as development of a better drug for breast cancer. The
early stages of biomedical research usually occur in a laboratory. As
scientists gain more knowledge in a particular area, they begin studies on
humans. These studies often take place in hospitals or clinics and are called
clinical research.
Clinical research usually is
performed by multidisciplinary teams, rather than by individual scientists
working alone. These groups of men and women have knowledge and skills in
different areas, or disciplines, of science. A multidisciplinary biomedical
research team may include biochemists, geneticists, physiologists, and
physicians. Each team member approaches the problem from a different side and
shares knowledge with the group. This multidisciplinary approach increases the
chances of solving a problem or developing a new treatment.
(back
to content)
6.1
Clinical Trials C
One of the greatest advances in
medicine was the introduction of a new research technique in the mid-1950s
called the controlled clinical trial, which is used to determine if new drugs
and other treatments are safe and effective. In the controlled clinical trial,
one group of patients, the treatment group, receives the new drug or new
treatment. Another group, the control group, is given an inactive pill (a
placebo) or the best standard treatment. Researchers then compare the two
groups over a period of time. The data collected is put through rigorous
statistical techniques to determine whether the new treatment is safer and more
effective than standard therapy or no treatment.
Most clinical trials are
conducted on a blind or double-blind basis. In a blind trial, patients do not
know whether they receive the new drug or a placebo. In a double-blind trial,
neither patients nor physicians know who is receiving the new treatment. This
secrecy is important because patients who know they are taking a powerful new
drug may expect to feel better and report improvement to doctors. Researchers
who know that a patient is receiving the test treatment may also see
improvements that really do not exist.
Clinical trials usually are
randomized. Researchers put patients into the treatment group or control group
at random. This helps to assure that neither group contains an excess of
patients with severe disease. A drug may appear more effective if the treatment
group were packed with patients who had only mild symptoms.
The results of clinical trials
are subjected to peer review. Researchers publish their results in scientific
journals or present them to an audience of other scientists, who are their
peers. This gives scientists not involved in the research a chance to spot
potential errors.
6.2 Medical Ethics c
INTRODUCTION
Medical Ethics or Bioethics,
study and application of moral values, rights, and duties in the fields of
medical treatment and research. Medical decisions involving moral issues are
made every day in diverse situations such as the relationship between patient
and physician, the treatment of human and animal subjects in biomedical
experimentation, the allocation of scarce medical resources, the complex
questions that surround the beginning and the end of a human life, and the
conduct of clinical medicine and life-sciences research.
Medical ethics traces its roots
back as far as ancient Greece, but the field gained particular prominence in
the late 20th century. Many of the current issues in medical ethics are the
product of advances in scientific knowledge and biomedical technology. These
advances have presented humanity not only with great progress in treating and
preventing disease but also with new questions and uncertainties about the
basic nature of life and death. As people have grappled with issues on the
frontier of medical science and research, medical ethics has grown into a
separate profession and field of study. Professional medical ethicists bring
expertise from fields such as philosophy, social sciences, medicine, research
science, law, and theology.
Medical ethicists serve as
advisors to hospitals and other health-care institutions. They have also served
as advisors to government at various levels. For example, experts in medical
ethics assisted the United States government from 1974 to 1978 as members of
the National Commission for the Protection of Human Subjects of Medical
Research. The commission was formed in response to several large-scale
experiments that used human subjects who were tricked into participating. In
the late 1990s the National Bioethics Advisory Commission, at the direction of
President Bill Clinton, studied issues related to the cloning of human beings.
Ethicists also serve as advisors to state legislatures in the writing of laws
concerning the decision to end life support, the use of genetic testing,
physician-assisted suicide, and other matters. Medical ethics has even become
part of the landscape in the commercial world of science. An increasing number
of firms involved in biotechnology (the business of applying biological and
genetic research to the development of new drugs and other products) regularly
consult with medical ethicists about business and research practices.
The field of medical ethics is
also an international discipline. The World Health Organization founded the
Council for International Organizations of Medical Sciences in 1949 to collect
worldwide data on the use of human subjects in research. In 1993 the United
Nations Educational, Scientific, and Cultural Organization (UNESCO) established
an International Bioethics Committee to examine and monitor worldwide issues in
medicine and life-sciences research. The UNESCO directory lists more than 500
centers outside the United States. The International Association of Bioethics
was founded in 1997 to facilitate the exchange of information in medical ethics
issues and to encourage research and teaching in the field.
In the United States and Canada
more than 25 universities offer degrees in medical ethics. In many instances,
the subject is also part of the curriculum in the education of physicians and
other health-care professionals. Many medical schools include ethics courses
that examine topics such as theories of moral decision-making and the
responsible conduct of medical research.
HISTORY
|
 �������� C �������� C
|
Hippocrates
Greek physician and philosopher Hippocrates (460?-377? bc),
regarded as the father of medicine, is considered the first to formally address
the ethical issues associated with medical practices.
CULVER PICTURES
The examination of moral issues
in medicine largely began with the Greeks in the 4th century BC. The Greek
physician Hippocrates is associated with more than 70 works pertaining to
medicine. However, modern scholars are not certain how many of these works can
be attributed to Hippocrates himself, as some may have been written by his
followers. One work that is generally credited to Hippocrates contains one of
the first statements on medical ethics. In Epidemics I, in the midst of
instructions on how to diagnose various illnesses, Hippocrates offers the
following, �As to diseases, make a habit of two things�to help and not to
harm.�
The most famous ethical
work�although the exact origin of the text is unknown�is the Hippocratic Oath.
In eight paragraphs, those swearing the oath pledge to �keep [patients] from
harm and injustice.� The oath also requires physicians to give their loyalty
and support to their fellow physicians, promise to apply dietetic measures for
the benefit of the sick, refuse to provide abortion or euthanasia (the act of
assisting a chronically ill person to die), and swear not to make improper
sexual advances against any members of the household. �In purity and holiness I
will guard my life and my art,� concludes one section of the oath. For most of
the 20th century, it was common for modified versions of the Hippocratic Oath
to be recited by medical students upon the awarding of their degrees. For many
people, the oath still symbolizes a physician�s duties and obligations.
The idea of ethical conduct is
common in many early texts, including those from ancient India and
China�cultures in which medical knowledge was viewed as divine or magical in
origin. Echoing the Hippocratic Oath, the Caraka Samhita, a Sanskrit text
written in India roughly 2,000 years ago, urges the following commandment to
physicians, �Day and night, however you may be engaged, you shall strive for
the relief of the patient with all your heart and soul. You shall not desert
the patient even for the sake of your life or living.� Similar sentiments can
be found in the Chinese text Nei Jing (The Yellow Emperor's Classic of Inner
Medicine), dating from the 2nd century BC. This work stressed the connection
between virtue and health. Three centuries later, the work of the Chinese
physician Sun Simiao emphasized compassion and humility, �...a Great Physician
should not pay attention to status, wealth, or age.... He should meet everyone
on equal ground....�
In Europe during the Middle Ages,
the ethical standards of physicians were put to the test by the bubonic plague,
the highly contagious Black Death that arrived around the mid-1300s and
remained a threat for centuries. When plague broke out, physicians had a
choice: They could stay and treat the sick�risking death in the process�or
flee. The bubonic plague and other epidemics provide an early example of the
challenges that still exist today when doctors must decide whether they are
willing to face personal risks when caring for their patients.
By the 18th century, particularly
in Britain, the emphasis in medical ethics centered on proper, honorable
behavior. One of the best-known works from the period is Medical Ethics; or, a
Code of Institutes and Precepts, Adapted to the Professional Conduct of
Physicians and Surgeons, published in 1803 by the British physician Thomas
Percival. In his 72 precepts, Percival urged a level of care and attention such
that doctors would �inspire the minds of their patients with gratitude,
respect, and confidence.� His ethics, however, also permitted withholding the
truth from a patient if the truth might be �deeply injurious to himself, to his
family, and to the public.� At roughly the same time American physician Benjamin
Rush, a signer of the Declaration of Independence, was promoting American
medical ethics. His lectures to medical students at the University of
Pennsylvania in Philadelphia, spoke of the virtues of generosity, honesty,
piety, and service to the poor.
By the early 19th century, it
seemed that such virtues were in short supply, and the public generally held
physicians in North America in low esteem. Complicating the problem was the
existence of a variety of faith healers and other unconventional practitioners
who flourished in an almost entirely unregulated medical marketplace. In part
to remedy this situation, physicians convened in 1847 to form a national
association devoted to the improvement of standards in medical education and
practice. The American Medical Association (AMA), as the group called itself,
issued its own code of ethics, stating, �A physician shall be dedicated to
providing competent medical service with compassion and respect for human
dignity. A physician shall recognize a responsibility to participate in
activities contributing to an improved community.� This text was largely
modeled on the British code written by Percival, but it added the idea of
mutually shared responsibilities and obligations among doctor, patient, and
society. Since its creation, the AMA Code has been updated as challenging
ethical issues have arisen in science and medicine. The code now consists of
seven principles centered on compassionate service along with respect for
patients, colleagues, and the law. The Canadian Medical Association (CMA),
established in 1867, also developed a Code of Ethics as a guide for physicians.
Today the CMA code provides over 40 guidelines about physician responsibilities
to patients, society, and the medical profession.
In recent years, however, the
field of medical ethics has struggled to keep pace with the many complex issues
raised by new technologies for creating and sustaining life.
Artificial-respiration devices, kidney dialysis, and other machines can keep
patients alive who previously would have succumbed to their illnesses or
injuries. Advances in organ transplantation have brought new hope to those
afflicted with diseased organs. New techniques have enabled prospective parents
to conquer infertility. Progress in molecular biology and genetics has placed
scientists in control of the most basic biochemical processes of life. With the
advent of these new technologies, codes of medical ethics have become
inadequate or obsolete as new questions and issues continue to confront medical
ethicists.
HOW ARE ETHICAL DECISIONS MADE IN MEDICINE?
Throughout history the practice
of medical ethics has drawn on a variety of philosophical concepts. One such
concept is deontology, a branch of ethical teaching centered on the idea that
actions must be guided above all by adherence to clear principles, such as
respect for free will. In contemporary bioethics, the idea of autonomy has been
of central importance in this tradition. Autonomy is the right of individuals
to determine their own fates and live their lives the way they choose, as long
as they do not interfere with the rights of others. Other medical ethicists
have championed a principle known as utilitarianism, a moral framework in which
actions are judged primarily by their results. Utilitarianism holds that
actions or policies that achieve good results�particularly the greatest good
for the greatest number of people�are judged to be moral. Still another
philosophical idea that has been central to medical ethics is virtue ethics,
which holds that those who are taught to be good will do what is right.
Many medical ethicists find that
these general philosophical principles are abstract and difficult to apply to
complex ethical issues in medicine. To better evaluate medical cases and make
decisions, medical ethicists have tried to establish specific ethical
frameworks and procedures. One system, developed in the late 1970s by the
American philosopher Tom Beauchamp and the American theologian James Childress,
is known as principlism, or the Four Principles Approach. In this system
ethical decisions pertaining to biomedicine are made by weighing the importance
of four separate elements: respecting each person�s autonomy and their right to
their own decisions and beliefs; the principle of beneficence, helping people
as the primary goal; the related principle of nonmalificence, refraining from
harming people; and justice, distributing burdens and benefits fairly.
Medical ethicists must often
weigh these four principles against one another. For example, all four
principles would come into play in the case of a patient who falls into an
irreversible coma without expectation of recovery and who is kept alive by a
mechanical device that artificially maintains basic life functions such as
heartbeat and respiration. The patient�s family members might argue that the
patient, if able to make the decision, would never want to be sustained on a
life-support machine. They would argue from the viewpoint of patient
autonomy�that the patient should be disconnected from the machine and allowed
to die with dignity. Doctors and hospital staff, meanwhile, would likely be
concerned with the principles of beneficence and nonmalificence�the fundamental
desire to help the patient or to refrain from harmful actions, such as terminating
life support. Consulting on such a case, the medical ethicist would help decide
which of these conflicting principles should carry the most weight. An ethicist
using principlism might work toward a solution that addresses both sides of the
conflict. Perhaps the family and medical staff could agree to set a time limit
during which doctors would have the opportunity to exhaust every possibility of
cure or recovery, thus promoting beneficence. But at the end of the designated
period, doctors would agree to terminate life support in ultimate accordance
with the patient�s autonomy.
Although some medical ethicists
follow principlism, others employ a system known as casuistry, a case-based
approach. When faced with a complex bioethical case, casuists attempt to
envision a similar yet clearer case in which virtually anyone could agree on a
solution. By weighing solutions to the hypothetical case, casuists work their
way toward a solution to the real case at hand.
Casuists might confront a case
that involves deciding how much to explain to a gravely ill patient about his
or her condition, given that the truth might be so upsetting as to actually
interfere with treatment. In one such case cited by American ethicist Mark
Kuczewski from the Center for the Study of Bioethics at the Medical College of
Wisconsin in Milwaukee, a 55-year-old man was diagnosed with the same form of
cancer that had killed his father. After a surgical procedure to remove the
tumor, the patient�s family members privately told his doctors that if the
patient knew the full truth about his condition, he would be devastated. In
weighing this matter, a casuist might envision a clear-cut case in which a
patient explicitly instructs doctors or caregivers not to share any negative
information about prospects for cure or survival. The opposite scenario would
be a case in which the patient clearly wishes to know every bit of diagnostic
information, even if the news is bad. The challenge for the casuist is to
determine which scenario, or paradigm, most closely resembles the dilemma at
hand, and, with careful consideration of the case, try to proceed from the
hypothetical to a practical solution. In this particular case, the cancer
patient was informed that his tumor had not been successfully removed and that
more curative measures were called for. His treatments continued. In the end,
however, he died of the disease without ever being told of a terminal
diagnosis.
CURRENT MEDICAL ETHICS ISSUES
Casuistry and principlism are
just two of many bioethical frameworks. Each approach has its proponents, and
volleys of disagreement and debate frequently fly among the various schools of
thought. Yet each approach represents an attempt to deal with thorny,
conflicting issues that commonly arise in the complex and contentious arena of
medicine. These issues can include the rights and needs of the patient, who
may, for example, decide to discontinue treatment for a life-threatening
illness, preferring to die with dignity while still mentally competent to make
that choice. There is the obligation of the doctor, whose duty it is to save
and prolong life. There is the hospital or health-care system, whose
administrators must weigh the obligation to sustain life against the
often-enormous expense of modern medical methods. And there is the law, which
seeks to protect citizens from harm while at the same time respecting autonomy.
The remainder of this article discusses some of the most prominent dilemmas and
decisions faced by modern medical ethicists.
MORTALITY ISSUES
|
 �C��������������������� �C���������������������
|
Man on Life Support
Life support equipment keeps an
elderly man alive at a hospital. Proponents of euthanasia believe that
unnecessarily prolonging life in terminally ill patients causes suffering to
the patients and their family members. Many societies now permit passive
euthanasia, which allows physicians to withhold or withdraw life-sustaining
treatment when directed to do so by the patient or an authorized
representative.
Jan Halaska/Photo Researchers, Inc.
For many centuries death was
clearly indicated by the absence of a pulse or signs of breathing. In the 1960s
advances in life-support technology, such as mechanical respirators and the
heart-lung machine, enabled physicians to artificially maintain function in the
heart and lungs, and the clear signs of death became blurred. The resulting
challenge�to forge a new definition of death�was a major spur to the growth of
medical ethics during the 1960s and 1970s.
An early effort along these lines
was a set of guidelines issued by a committee at the Harvard University Medical
School in Boston, Massachusetts, in 1968. These guidelines introduced the
concept of brain death�defined as an end of all function in the brain and
central nervous system, even in a body sustained by artificial technology. In
1981 a United States federal advisory group on medical ethics, the President�s
Commission for the Study of Ethical Problems in Medicine and Biomedical and
Behavioral Research, created a guideline for defining death that specifies not
only �irreversible cessation of circulatory and respiratory functions,� but
also �irreversible cessation of all functions of the entire brain.� Within a
few years, most states had adopted this definition. Most European nations,
Canada, Australia, and Central and South American nations define death either
as the loss of all independent lung and heart function or the permanent and
irreversible loss of all brain function.
The concept of brain death did
not solve the dilemma of patients being sustained by artificial
means�particularly in cases of permanent vegetative states (when a patient has
some brain function but shows no response to the external environment). Using
medical technology, these patients can be kept alive for years, if not decades.
A landmark bioethical and legal case in this area concerned Karen Ann Quinlan,
a 21-year-old woman in 1975 who fell into a permanent vegetative state as a
result of ingesting a mixture of tranquilizers and alcohol. Her parents,
carrying out what they believed their daughter's wishes would be, requested
that she be disconnected from her life-support system. Hospital officials,
while sympathetic to the parents� wishes, would not agree, and a long court
battle followed. Ultimately a New Jersey court agreed with the parents, and
Quinlan was disconnected from her respirator. (Unexpectedly, she began to
breathe on her own and lived another ten years in a nursing home.)
The Quinlan case brought the
�right to die� issue into the realm of public discussion. As a result, in many
cases, patients can now make advanced directives, also known as living wills,
directing that their lives not be sustained by artificial means. Other aged or
gravely ill patients have used living wills to specify that if they should
suffer heart failure or other crises while in the hospital, medical staff
should make no extraordinary effort to resuscitate them.
Allowing a patient to die raises
one set of ethical issues. Actively helping a patient achieve death, often
referred to as euthanasia, raises still other moral questions. For many years,
medical ethicists have debated whether there is a significant distinction
between the two courses of action. In the United States (with the exception of
Oregon), Canada, and most other nations, euthanasia is illegal. In the
Netherlands, the parliament in 1993 established informal guidelines under which
physicians would not be prosecuted for participating in voluntary euthanasia.
The Dutch parliament formally legalized voluntary euthanasia in 2000, provided
that it involved the full consent of the patient and agreement of all concerned
medical personnel.
�
|
 ����������������������������������������� C ����������������������������������������� C
|
Jack Kevorkian
In 1999 retired physician Jack Kevorkian was convicted of
second-degree murder and delivery of a controlled substance after he injected a
terminally ill man with a lethal dosage of medication. He was sentenced to 10
to 25 years in prison. Kevorkian remains an outspoken advocate of assisted
suicide.
Reuters/Corbis
Still another controversy related
to euthanasia concerns the decision of when, and if, it is ethically permissible
to withhold treatment from a child. This issue came into public focus with the
case of �Baby Doe� in 1982. The newborn infant was diagnosed with Down
Syndrome, a chromosomal disorder that causes moderate to severe developmental
disabilities. The baby also had a hole in the esophagus (the passageway through
the throat) that prevented the baby from feeding. The parents, apparently
unwilling to raise a child with Down Syndrome, refused to consent to the
routine surgery that could have corrected the esophageal defect, and the baby
died after six days. The case outraged many, and officials in the
administration of President Ronald Reagan rushed to pass legislation preventing
future similar scenarios.
An issue related to euthanasia is
assisted suicide, voluntary suicide with the help of another person. In the
United States this matter has been highly publicized through the actions of
American physician Jack Kevorkian, who in recent years assisted in more than
130 suicides. In 1999, after several previous acquittals in other cases,
Kevorkian was convicted of second-degree murder after administering a lethal
injection to a Michigan man suffering from amyotrophic lateral sclerosis, a
progressively debilitating, currently incurable disease. Kevorkian was
sentenced to 10 to 25 years in prison but was released in 2007 after serving 8
years of his sentence.
In Canada, assisted suicide is
illegal. In the United States, the legal situation regarding assisted suicide
has been left largely to the individual states. In the 1997 decision of State
of Washington v. Glucksberg, the Supreme Court of the United States determined
that there is no constitutional right to die with the help of a physician. The
Court has also upheld state laws that ban assisted suicide. However, in 1994
and again in 1997 voters in the state of Oregon approved a measure allowing
physicians to prescribe lethal medications when requested by a mentally
competent adult who is suffering in the final stages of terminal illness. In
2006 the Supreme Court upheld Oregon�s assisted suicide law by a 6-3 vote,
after the administration of President George W. Bush challenged the law�s
legality.
All these issues�determining when
life has ended and deciding what constitutes a reasonable quality of life and
whether the patient, the health-care system, or the courts should have ultimate
authority in life or death�remain unresolved and continue to challenge medical
ethicists.
REPRODUCTIVE MEDICINE
|
�
|
Assisted Reproductive Technologies c
In these methods used to treat infertility, three methods
(IVF, ZIFT, and ICSI) artificially induce the union of sperm and egg in the
laboratory before implanting the fertilized egg inside the female reproductive
system. The fourth method (GIFT) mixes unfertilized eggs and sperm in the laboratory
before transferring them to the fallopian tube, where fertilization takes place
naturally.
� Microsoft Corporation. All Rights Reserved. c
Many new questions of medical
ethics have occurred as a result of developments in reproductive medicine. In
the 1960s the development of the birth-control pill raised ethical issues,
especially for people whose religions forbade the use of artificial birth
control. In 1973 the United States Supreme Court legalized abortion with its
landmark Roe v. Wade decision. In 1988 the Canadian Supreme Court removed
abortion from the Criminal Code of Canada, enabling the decision of abortion to
be made confidentially between a patient and her physician within the confines
of Canadian law. Controversy surrounding these rulings�including discussion of
the origins and meaning of personhood, the rights of the fetus and pregnant
women, and the role the state should play in reproductive decisions�have kept
abortion a volatile political and ethical issue into the 21st century.
Contributing to this heated
debate has been the development of a variety of drugs that either prevent or
end pregnancies. Emergency contraceptive pills, commonly known as morning-after
pills, use high doses of hormones that can prevent or delay ovulation, inhibit
a sperm from fertilizing an egg, or make the uterine lining inhospitable to a
fertilized egg. If taken by a woman within 72 hours after unprotected sexual
intercourse, these drugs can prevent pregnancy. Doctors have long prescribed
high doses of certain oral contraceptives to patients within three days after
unprotected intercourse. More recently, drugs specifically created for the
purpose of emergency contraception have become available. In some states of the
United States, these drugs can be dispensed by a pharmacist without a doctor's
prescription. Abortion rights advocates consider these drugs a welcome addition
to the limited number of effective contraceptive methods, but abortion
opponents strongly disagree. Since there is a small chance that these drugs may
take effect after an egg is fertilized, when abortion opponents believe a human
life has already begun, critics view the drug as just another form of abortion.
Even more controversial is the
drug mifepristone, also known as RU-486. Mifepristone is used to induce
abortion in the first seven weeks of pregnancy�when an embryo is less than 2.5
cm (1 in) in length�without requiring surgery. Developed by a French
pharmaceutical firm, mifepristone was first approved for use in France in 1988;
later it was approved in the United Kingdom, Sweden, and other European
countries. The drug was approved for use in the United States in 2000 under the
brand name Mifeprex.
Mifepristone blocks progesterone,
a hormone required to maintain pregnancy. A woman receives mifepristone in her
physician's office. She then returns to the doctor's office within 48 hours to
take the drug misoprostol, a hormone-like substance that makes the uterus
contract and expel fetal tissue. A woman typically experiences bleeding and
cramping that may last from 9 to 16 days. Two weeks after receiving the second
drug, the woman returns to her physician to make sure the drug treatment was
successful in terminating the pregnancy.
Opponents of abortion contend
that the easy availability of this drug increases the chance that women will
choose this method as a form of belated birth control. Abortion rights
advocates note that, since use of the drug is a private matter between a woman
and her physician and requires no surgery, a woman no longer needs to visit an
abortion clinic, which may be targeted by antiabortion protesters. Proponents
also cite evidence from clinical trials of the drug showing that many women
preferred the less invasive procedure to a surgical abortion because it helped
them feel more in control of their personal health. As with other abortion
procedures, the cost of mifepristone will not be covered by Medicaid, the
federal health insurance program for low-income individuals and families,
unless the pregnancy results from rape or incest or endangers the life of the
mother. Advocates complain that as a result poor women do not have the same
access to reproductive health care that wealthier women have.
�
|
 c c
|
Prenatal Testing
Two types of medical tests may be used early in a woman�s
pregnancy to determine if her fetus has a defective gene or a chromosomal
abnormality. Both procedures remove cells surrounding the developing fetus. The
cells obtained have the same genetic makeup as the fetus and can be tested for
genetic abnormalities. In chorionic villus sampling, a doctor removes tissue
from the chorionic villi, fingerlike projections that are part of the
developing placenta, between 10 and 12 weeks of pregnancy. Using ultrasound
guidance, the doctor inserts either a needle through the woman�s abdominal wall
or a thin, hollow tube called a catheter through her cervix to reach the
chorionic villi. The doctor suctions out cells using a syringe. Amniocentesis
is usually performed between 15 and 17 weeks of pregnancy. In this procedure, a
doctor uses ultrasound guidance to insert a needle through the abdominal wall
into the amniotic fluid surrounding the fetus. Cells from the amniotic fluid
are removed using a syringe. Both procedures pose a slight risk for the
developing fetus, and health professionals recommend these tests only in cases
in which a mother or father has a family history of a genetic disorder or a
known risk for chromosomal abnormalities.
� Microsoft Corporation. All Rights Reserved.
Infertility is also an important
area of medical ethics. Many couples unable to have children turn to
fertility-enhancing technologies for help. Artificial insemination, a method in
which doctors introduce semen into the cervix, raised new ethical issues about
how potential parents should choose sperm or egg donors, on what basis and with
what assurances of privacy donors should be recruited, and whether donors are
entitled to parental rights or financial compensation.
In 1978 the birth of the first
so-called test-tube baby was an important technological breakthrough. Doctors
used in vitro fertilization (IVF), a method in which fertilization of the ovum
with sperm was conducted in a laboratory and the resulting embryo was
subsequently implanted in the mother's uterus. Soon thereafter, a variety of
other IVF techniques were developed. Not surprisingly, these procedures have
raised significant ethical questions, including some about the safety of the
costly technique. To increase the chance for success, doctors may fertilize and
implant more than one embryo into a woman�s uterus. Some experts have raised
concerns about this practice because it increases the incidence of multiple
births, which can create a health risk for the mother and babies and can place
a heavy burden on the parents. When more than one embryo implants in the
uterus, doctors can selectively remove one or more of the embryos to improve
the chances that the others will survive, but this raises additional ethical
issues related to abortion. Questions have also arisen over the fate of the
fertilized eggs that are not implanted and the fate of the human embryos if the
couples who created them die, become incapacitated, or no longer want to have
children.
Advances in prenatal diagnostic
techniques, such as genetic testing, in the 1960s and 1970s made it possible to
test a fetus (and more recently an embryo) for genetic diseases, such as
sickle-cell anemia, and other disorders prior to birth. These techniques,
including chorionic villus sampling and amniocentesis, led to discussions about
the morality of using medicine to end pregnancies based on the predicted
disability and quality of life that the baby might face. An experimental technique
known as preimplantation genetic diagnosis could help couples avoid facing this
difficult decision. This technique enables doctors to analyze the genetic
material of embryos created through IVF before they are implanted in a woman's
uterus. Only healthy embryos are then implanted. A related technique enables
doctors to determine the sex of the baby before the embryos are implanted.
Couples at risk of passing on a genetic disorder that affects males may choose
to have only female embryos implanted. However, these prenatal techniques have
raised additional ethical questions about the rights of parents to design their
descendants.
GENETIC TECHNOLOGY ISSUES
|
��C
|
Genetic Engineering
1. In genetic engineering, scientists use restriction
enzymes to isolate a segment of deoxyribonucleic acid (DNA) that contains a
gene�for example, the gene regulating insulin production. 2. A plasmid removed
from a bacterium and treated with the same restriction enzyme binds with the
DNA fragment to form a hybrid plasmid. 3. The hybrid plasmid is re-inserted
back into the bacterium, where it replicates as part of the cell�s DNA. 4. A
large number of identical daughter cells (clones) can be cultured and their
gene products extracted for human use.
� Microsoft Corporation. All Rights Reserved.
Along with developing new methods
for ending pregnancies or aiding fertility, modern medical science has created
new means of manipulating the very building blocks of life itself. These
techniques, in the fields of genetic engineering and biotechnology, have caused
much public discussion on medical ethics in recent years.
Since the early 1970s, scientists
have refined and improved methods for isolating and manipulating genes�the
basic units of heredity made up of deoxyribonucleic acid (DNA) that hold the
master instructions for the creation of proteins. Proteins act as molecular
laborers, controlling every aspect of cell activity. Specific segments of DNA
can be removed from one organism and inserted into the genes of another
species. In this way the function of selected genes can be deactivated or
amplified, changing the actions of hormones and other proteins and
fundamentally altering the characteristics of life forms.
For some medical ethicists and
other observers, such gene manipulation raises serious ethical and practical
concerns. These doubters have asked the following questions: Just because
scientists can perform such wonders, does it follow that they should do so? Are
there unforeseen dangers in altering life at the biochemical level? Is genetic
diversity threatened by such activity?
�
|
 �C �C
|
Correcting Genetic Diseases
Gene therapy may someday be able to cure hereditary
diseases, such as hemophilia and cystic fibrosis, which are caused by missing
or defective genes. In one type of gene therapy, genetically engineered viruses
are used to insert new, functioning genes into the cells of people who are
unable to produce certain hormones or proteins necessary for the body to
function normally.
� Microsoft Corporation. All Rights Reserved.
Biotechnology and genetic
engineering also raise issues concerning commercial exploitation, such as
attempts to patent human gene sequences. Patents protect inventors and others
by forbidding any imitators from using or profiting from the patent-holder�s
original material. But can life itself be patented? In 1980 the U.S. Supreme
Court suggested in its decision Diamond v. Chakrabarty that life can be
patented. The Court granted patent protection to a scientist who had developed
a new bacterium strain that was capable of serving as a natural cleanup agent
in accidental oil spills (see Bioremediation).
Six years later the Court ruled
that any life form developed through biotechnology�excluding humans�could be
considered a patentable invention. More recently, as work has proceeded on
mapping the human genome (the entire set of genes found in the nucleus of each
human cell), biotechnology companies have scrambled to file patents on
individual genes that they have �discovered��whether the companies know the
function of the gene or not. In 2000, for example, a controversy erupted when a
biotechnology company won a patent for a gene involved in the process by which
the human immunodeficiency virus (HIV), the virus that causes acquired
immunodeficiency syndrome (AIDS), infects cells. The patent was granted even
though other scientists had previously made discoveries regarding the gene�s
function.
To some medical ethicists, the
patenting of genes is troubling. A central argument against patenting is that
competitive ownership of individual genes might prevent scientists from sharing
knowledge. This, of course, would hamper basic biomedical research and the
ongoing search for treatments and cures. President Clinton and British prime
minister Tony Blair addressed this concern early in 2000 when they jointly
called for an agreement for American and British scientists to openly share all
information derived from the sequencing of the human genome (see Human Genome
Project).
CLONING
Perhaps no event in biotechnology
has caused more uproar and bioethical discussion than the cloning of Dolly the
sheep by Scottish scientists. Dolly was created when the scientists removed the
nucleus from a cell taken from the udder of a six-year-old sheep, placed it
into the egg cell of another sheep from which the nucleus had been removed, and
planted the egg cell within a surrogate mother, which carried Dolly to term.
Dolly was born an identical twin to her six-year-old parent.
Dolly�s birth created a sensation
in the press and caused a wave of anxiety over the prospects for cloning
humans. President Clinton announced an immediate ban on federal funding for
research related to human cloning. The U.S. National Bioethics Advisory
Committee recommended that federally funded research that had produced Dolly
not be applied to humans. Several other nations have laws prohibiting human
cloning, including Australia, Austria, Canada, Denmark, France, Germany,
Norway, Slovakia, South Africa, Spain, Sweden, Switzerland, and the United
Kingdom. The debate over the ethics of creating human clones and the
circumstances under which human cloning might be used remains unsettled.
PHYSICIAN-PATIENT ISSUES
Since the time of Hippocrates
more than 2,000 years ago, a central concern of medical ethics has been the relationship
between physician and patient. Aspects of this relationship continue to be the
source of ethical dilemmas. For example, what is the extent of the doctor�s
duty to a patient if treating the patient places the doctor at risk? This issue
was brought to the forefront in recent years by the advent of the AIDS crisis.
HIV, the virus that causes AIDS, can be spread by contact with blood and other
bodily fluids of an infected person. This poses a potential hazard for doctors
and other health-care workers. In the 1980s, during the early days of the AIDS
epidemic, some doctors refused to treat persons in high-risk groups for AIDS,
such as homosexual men and users of intravenous drugs�even though these
patients were not known to be infected with HIV.
Is there an ethical obligation
for doctors to treat patients with communicable and potentially fatal diseases?
In a statement in 1988, the AMA�s Council on Ethical and Judicial Affairs
declared that no patient should suffer discrimination or be denied care because
of infection with HIV. Many states and cities have passed laws barring
health-care discrimination against persons with HIV and AIDS. Nevertheless, the
licensing boards that oversee the practice of medicine in each state have taken
varied approaches. The boards in some states have passed regulations against
any refusal to treat persons with HIV infection; other state boards specify
that doctors may refuse to treat such patients provided that they make a
reasonable effort to secure alternate care. In 1998 the U.S. Supreme Court
ruled that denying care to an HIV-infected person violated the federal
Americans with Disabilities Act. AIDS advocates hope that this ruling will
protect the rights of many people with AIDS.
HUMAN EXPERIMENTATION
|
� �C �C
|
Medical Experiment in Nazi Concentration Camp
A gaping wound on a woman�s arm
is the result of a medical experiment carried out by Nazi physicians on a
female prisoner held at the concentration camp at Ravensbr�ck, Germany. In the
experiment, a mixture of phosphorus and rubber was applied to the skin and
ignited. After 20 seconds the fire was extinguished with water. Three days
later the burn was treated with a liquid form of the herbal remedy echinacea to
observe how fast the burn would heal. This photograph, taken by a camp
physician, was entered as evidence during the Doctors Trial, in which a United
States military tribunal opened criminal proceedings in 1946 against 23 leading
German physicians and administrators for their willing participation in war
crimes and crimes against humanity.
NATIONAL ARCHIVES, COURTESY OF US HOLOCAUST MEMORIAL MUSEUM
PHOTO ARCHIVES
Ethical issues arise not only in
the clinical setting of a hospital or doctor�s office, but in the laboratory as
well. A main concern of medical ethicists is monitoring the design of clinical
trials and other experiments involving human subjects. Medical ethicists are
particularly interested in confirming that all the subjects have voluntarily
given their consent and have been fully informed of the nature of the study and
its potential consequences. In this particular area of medical ethics, one
infamous period in history has echoed loudly for more than half a century: the
experiments conducted by Nazi doctors on captive, unwilling human subjects
during World War II (1939-1945). Under the guise of science, thousands of Jews
and other prisoners were subjected to grotesque and horrifying procedures. Some
were frozen to death, or slowly and fatally deprived of oxygen in experiments
that simulated the effects of high altitude. Others were deliberately infected
with cholera and other infectious agents or subjected to bizarre experiments
involving transfusions of blood or transplants of organs. Many underwent
sterilization, as Nazi doctors investigated the most efficient means of
sterilizing what they considered inferior populations. In all, these inhumane
acts so outraged the world that, after the war, trials were held in N�rnberg,
Germany, and many of the responsible Nazi physicians were convicted and
executed as war criminals.
These trials essentially marked
the beginning of modern medical ethics. The international tribunal that
prosecuted the Nazi doctors at N�rnberg drew up a list of conditions necessary
to ensure ethical experimentation involving humans. This document, which came
to be called the Nuremberg Code, stressed the importance of voluntary, informed
consent of subjects in well-designed experimental procedures that would aid
society without causing undue suffering or injury.
�
|
 �C �C
|
Clinton Apologizes for Tuskegee Study
United States president Bill
Clinton and a survivor of a government-sanctioned experiment on syphilis take
part in a formal ceremony at the White House on May 16, 1997. During the
ceremony, Clinton offered a formal apology to the surviving black men who
participated in the experiment. The study, formally known as the Tuskegee Study
of Untreated Syphilis in the Negro Male, was conducted from 1932 to 1972 and
involved 399 black men from rural Alabama who were infected with syphilis. The
U.S. Public Health Service closely monitored and evaluated the effects of the
disease on the study�s participants. In what Clinton described as a shameful
act, throughout the 40-year study the men were never told that they had
syphilis, and they were never offered penicillin to treat the disease. When
left untreated, syphilis can lead to mental illness, paralysis, and death. By
the time the study was halted, more than 120 men had died of syphilis and
related complications, at least 40 wives had been infected, and 19 children had
contracted the disease at birth.
Paul J. Richards/AFP/Getty Images
Unfortunately, not all scientists
adhered to the Nuremberg Code. In the United States, the decades following
World War II saw several incidents of experiments on unwitting subjects who had
not given informed consent. During the 1940s and 1950s, for example, hundreds
of pregnant women were given a radioactive solution that enabled doctors to
measure the amounts of iron in their blood. In the mid-1950s scientists
infected developmentally disabled children at a New York state hospital with
hepatitis in order to test a vaccine for the disease. In the early 1960s
doctors injected cancer cells into the skin of elderly, debilitated patients in
a hospital in Brooklyn, New York, to study the patients� immune responses.
Perhaps the most shameful episode in American medical history was the federal
government�s Tuskegee syphilis experiment. This 40-year study began in 1932 in
Tuskegee, Alabama, and tracked the health of approximately 600 African-American
men, two-thirds of whom suffered from the sexually transmitted disease
syphilis. Most of the subjects were poor and illiterate, and the researchers
deliberately kept the syphilis victims uninformed of their condition. Worse
yet, the researchers did not treat the disease, even though a cure for syphilis
was readily available during the last 30 years of the study. Instead, the
Public Health Service tracked the men, using them to study the physiological
effects of untreated syphilis. When the press broke the story of the Tuskegee
experiments in 1972, the revelations provided yet another spur to the
development of modern bioethics standards. (In 1997 President Clinton issued a
formal apology to the survivors of the Tuskegee Study and their families.)
Today clinical studies continue
to present bioethical challenges. Designing safe clinical experiments and
balancing the need for scientific objectivity against concern for the human
subjects can be a difficult proposition. An ethical dilemma is often presented
by the standard practice of using a placebo in a trial for a new drug or other
medical innovation. A placebo is an inactive substance that is given to some
subjects in a study in order to help researchers judge the real effects of the
compound being tested. But is it ethical in the trial of an AIDS drug, for
example, to give a useless placebo to persons suffering from a potentially
fatal condition when other persons in the study are receiving what may be a
beneficial drug? That is just one question that medical ethicists weigh in the
design of experiments involving humans.
ORGAN AND TISSUE TRANSPLANTS
|
 �C �C
|
Medical Transplants
For three decades after the first successful organ
transplant was performed in 1954, medical transplants were rare and often
unsuccessful. Thanks to advances in surgical techniques and the development of drugs
that supress organ rejection, organ transplant operations now are common and
generally successful.
� Microsoft Corporation. All Rights Reserved.
Modern techniques of medical
transplantation�surgically removing a diseased or malfunctioning kidney, heart,
or other organ, and replacing it with a healthy organ from a donor�has brought
new life and new hope to patients who, just a few generations ago, would have
died. But the practice has also raised significant ethical questions. One such
question centers on the cold reality of supply versus demand: At any moment,
there are upwards of 150,000 people in the world awaiting transplants. A
scarcity of donor organs usually means a long wait�during which some patients
die. A large supply of organs is available from the roughly 200,000 patients
worldwide who are declared brain-dead each year, but the problem has been to
secure consent from family members and loved ones to remove organs for
transplant.
For many years� medical ethicists
have considered the question of whether ethical means can be found to increase
the supply of donor organs. In the early 1980s, for example, American
bioethicist Arthur Caplan of the University of Pennsylvania discussed the
concept of presumed consent�the idea that, barring strenuous objection from
family members, doctors could presume that a person declared brain-dead would
be willing to donate organs to save others. Some Asian nations, as well as some
European nations, including France, Belgium, Austria, and Spain, have such
policies. The United States and Canada later enforced a concept advanced by
Caplan of required request�a policy whereby hospital personnel would be legally
required to seek permission from family members before harvesting organs. The
adoption of this policy in the United States and Canada increased the supply of
donated tissues, such as corneas and bone marrow, but failed to dramatically
increase the supply of donor organs.
Current United States and
Canadian law bars the sale or purchase of donor organs. The United States does
permit the sale of plasma and other bodily products, such as hair and sperm.
Would financial incentives provide a stimulus for more people to make organs
available? Some ethicists believe so, while others find the idea of marketing
organs ethically objectionable.
Other ethical issues are raised
by the practice of xenotransplantation�the use of animal tissues and organs for
human transplant. In 1984 the case of �Baby Fae� stimulated wide ethical
discussion. Doctors transplanted a baboon heart into a newborn girl to replace
her own fatally flawed heart. She died shortly after. Some critics contend that
xenotransplantation poses a danger to human health because of the risk of
transferring deadly animal viruses to the human population. This risk causes
bioethicists to question if such practices are ethical.
In recent years, one of the most
promising areas related to transplantation will likely trigger ethical debate
well into the future: the experimental use of tissues from aborted human
fetuses. In one particularly active area of this research, scientists have
experimented for more than a decade with grafting nerve cells from human
fetuses into the brains of patients suffering from Parkinson disease. This
disorder, caused by the mysterious death of brain cells that produce a chemical
called dopamine, gradually causes patients to lose control of their muscles. In
early studies some patients who received fetal cells showed improvement in
their symptoms, as the transplanted cells demonstrated the capacity to produce
dopamine. But the treatment also produced unpleasant side effects. This
research, like all research that depends on human fetal cells, has also
provoked debate. Critics question the ethics of using tissues from human
fetuses for any research purposes.
Ethical uncertainty hangs over a
related area of research on human embryonic stem cells. Human embryos contain
stem cells that have the ability to develop into almost any type of cell.
Scientists hope to direct stem cells to produce certain types of human tissue.
It is possible that someday these cells might be used for transplants or for
growing new tissue that can be grafted into the human body. For example,
scientists hope that stem cells might one day be used to replace nerve cells
destroyed by spinal injury, or heart muscle cells damaged during a heart
attack. Interest in this field was heightened considerably when scientists
announced in 1998 that they had learned how to grow human embryonic stem cells
in the laboratory.
At present the U.S. government
has banned federal funding for human-embryo research, although private
biotechnology companies are exempt from this ban and have been vigorously
pursuing research on embryonic cells. In 2000 the federally funded National
Institutes of Health (NIH) ruled that this ban was not necessary for studies
using cells derived from human embryos, since these cells are not embryos. The
NIH established guidelines enabling federal funds to be used in cases where
cells were derived from frozen embryos that were created for the purposes of
fertility treatment but were not going to be used and were therefore slated for
destruction. Other nations currently differ widely in their policies: France,
for example, has forbidden human-embryo research. No laws in Canada regulate
human-embryo research, although scientists or institutions receiving federal
funding must follow strict guidelines governing research on human embryos. The
United Kingdom has laws permitting some forms of human-embryo research, going
so far as to create guidelines allowing scientists to apply cloning technology
to human embryonic cells to create genetically identical cells for a potential
patient.
But the ethical questions remain:
Is it morally acceptable to use tissue taken from human embryos? One recent
development might change the nature of this argument. Scientists discovered in
1999 that stem cells taken from adult mice, and not human embryos, also display
an ability to change their function. Some stem-cell research continued with the
use of adult mouse cells. In 2007 government medical authorities in the United
Kingdom approved the creation of embryos that combine human and animal cells
for use in medical research. British researchers claimed the hybrid embryos
were vital in the fight against disease.
UNRESOLVED ISSUES FOR THE 21ST CENTURY
A variety of issues face medical
ethicists in the 21st century, such as advances in cloning technology, new
knowledge of the human brain, and the wealth of genetic data from the Human
Genome Project. Population changes worldwide will also affect the course of
medicine and will raise issues of medical ethics. By roughly the year 2020, the
number of Americans over the age of 65 is expected to double. This aging of the
population seems certain to increase the demand on the U.S. health-care
system�and to increase health-care costs. Issues concerning equitable access to
medical care will likely come to the fore, as resources for senior citizens
compete with other costs that must be borne by taxpayers. And, with an increase
in the number of elderly citizens, ethical dilemmas surrounding end-of-life
issues seem certain to become more prevalent. Determining the quality of life
for aged patients sustained by artificial means, deciding when treatment has
run its course for the aged�these will be issues that medical ethicists will
need to address. As they have for centuries, medical ethicists will continue to
ponder, debate, and advise on the most basic and profound questions of life and
death.
(back
to content)
7.0
References
1.����������� Dr. B. L.
Dickson, The Black Race; DNA And Why!? u (3-21), 2022
2.����������� Rochelle
Forrester, The History of Medicine e (6-62; 63-72), 2016
3.����������� Wagner,
The Origins and History of Medicine and Medical Practice g (73-101),
2017
4.����������� History
of use of Traditional Herbal Medicines h, 2003 (101-127)
5.����������� H.�
J. O'D.� Burke-Gaffney, The
history of medicine in the African countries k, 23 September
1966
6.����������� Ekeopara, Chike Augustine Ph.D1,
Rev. Ugoha, Azubuike; The Contributions of African Traditional Medicine to
Nigeria�s Health Care Delivery System; Origins of Traditional Medicine
(128-143) j; May 2017
7.����������� WHO,
Traditional and Modern Medicine: Harmonizing the Two Approaches i,
2000 (143-172)
8.����������� Caloriesmix,
Daily Nutrition Fact a, 2022
9.����������� Thomas
Nelson, A History of Medicine b, 1945
10.��������� Microsoft�
Encarta� 2009. � 1993-2008 Microsoft Corporation c,m
11.��������� Dr. Jenny
Scutcliffe and Nanacy Duin, A History of Medcine d, 1992 (2020)
12.��������� Tarik Catic1, Ivona Oborovic2, Edina
Redzic3, Aziz Sukalo4, Armin Skrbo2, Izet Masic5,
Traditional Chinese Medicine - an Overview p, 2018
13.��������� Ravishankar,
B and Shukla, V.J., INDIAN SYSTEMS OF MEDICINE: A BRIEF PROFILE o,
2007
14.��������� Yogacharya
Dr Ananda Balayogi Bhavanani, YOGA THERAPY: AN OVERVIEW �, 2016
15.��������� Toyin Adefolaju, The Dynamics and
Changing Structure of Traditional Healing System in Nigeria n,
2011
16.��������� Paolo Bellavite1, Anita Conforti2,
Valeria Piasere1 and Riccardo Ortolani3, Immunology
and Homeopathy. 1. Historical Background v, 2005
17.��������� Urs
Ha�feli, The History of Magnetism in Medicine t,
18.��������� Florida
Academy, The History of Massage Therapy s, 2019
19.��������� A van
Tubergen, S van der Linden, A brief history of spa therapy r, 2001
20.��������� Jaime
Schultz, A History of Kinesiology q, 2016
21.��������� Abb�
Mermet, Radiesthesia History o
22.��������� Tarik
Catic1, Ivona Oborovic2, Edina Redzic3, Aziz Sukalo4, Armin Skrbo2, Izet
��������������� Masic5,
Traditional Chinese Medicine - an Overview d, 2018
23.��������� Wikipedia,
Asahi Health w, 2022
24.��������� Wikipedia,
Thalassotherapy w, 2022
25.��������� Wikipedia,
Imhotep w, 2022
26.��������� Wikipedia,
History of Acupuncture w, 2022
27.��������� Wikipedia,
Reflexology w, 2022
28.��������� Wikipedia,
Shiatsu w, 2022�����������
29.��������� Wikipedia,
Traditional Tibetan medicine w, 2022
30.��������� Wikipedia,
Traditional Korean medicine w, 2022
31.��������� Wikipedia,
Indian Systems of Medicine: A Brief Profile w, 2022
32.��������� Wikipedia,
Siddha system of medicine w, 2022
33.��������� Wikipedia,
Unani system of medicine w, 2022
34.��������� Wikipedia,
List of forms of alternative medicine w, 2022
35.��������� Wikipedia,
Feng shui w, 2022
36.��������� Wikipedia,
Qigong w, 2022
37.��������� Wikipedia,
History of Use of Traditional Herbal Medicines w, 2022
38.��������� Wikipedia,
Herbal Medicine w, 2022
39.��������� Wikipedia,
Medicinal Plants w, 2022
40.��������� Wikipedia,
Origin of Traditional Medicine w, 2022
41.��������� Wikipedia,
Traditional Medicine w, 2022
42.��������� Wikipedia,
Traditional African Medicine w, 2022
43.��������� Wikipedia,
Alternative Medicine w, 2022
44.��������� Wikipedia,
Health in Nigeria w, 2022
45.��������� Wikipedia,
Healthcare in Nigeria w, 2022
46.��������� Wikipedia,
Siddha medicine w, 2022
47.��������� Wikipedia,
Crystal Healing is Metaphysics w, 2022
48.��������� Wikipedia,
The History of Physical Therapy w, 2022
49.��������� Wikipedia,
Electrohomeopathy w, 2022
50.��������� Wikipedia,
The Autogenic Training Method w, 2022
51.��������� Wikipedia,
Anthroposophy w, 2022
52.��������� Wikipedia,
Apitherapy w, 2022
53.��������� Wikipedia,
Bibliotherapy w, 2022
54.��������� wikipedia,
Chelation therapy w, 2022
55.��������� Wikipedia,
Thai Massage w, 2022
56.��������� Wikipedia,
Japan Kampo w, 2022
57.��������� Wikipedia,
Reiki w, 2022
58.��������� Wikipedia,
Rolfing w, 2022
59.��������� Wikipedia,
Biodanza w, 2022
60.��������� Wikipedia,
Speleotherapy w, 2022
61.��������� Wikipedia,
Arab medicine w, 2022
62.��������� Wikipedia,
Unanai Medicine w, 2022
63.��������� Wikipedia,
Traditional Mongolian medicine w, 2022
64.��������� Wikipedia,
Herbal Medicine w, 2022
65.��������� Wikipedia,
Medicinal Plants w, 2022
66.��������� Wikipedia,
Traditional Medicine w, 2022
67.��������� Wikipedia,
Alternative Medicine w, 2022
68.��������� Wikipedia,
Health in Nigeria w, 2022
69.��������� Wikipedia,
A History of Metaphysics w, 2022
70.��������� Wikipedia,
Spiritual Medicine w, 2022
71.��������� Wikipedia, A Brief History of
Aromatherapy w, 2022
72.��������� Wikipedia,
Osteopathic Philosophy and History w, 2022
73.��������� Wikipedia,
Craniosacral therapy w, 2022
74.��������� Wikipedia,
Origins and History of Chiropractic w, 2022
75.��������� Wikipedia,
Electrohomeopathy w, 2022
76.��������� Wikipedia,
Bioresonance Therapy w, 2022
77.��������� Wikipedia,
Anthroposophic medicine w, 2022
78.��������� Wikipedia,
The Autogenic Training Method w, 2022
79.��������� Wikipedia,
Alexander Technique Science w, 2022
80.��������� Wikipedia,
Apitherapy w, 2022
81.��������� Wikipedia,
Aquatic therapy w, 2022
82.��������� Wikipedia,
Chromotherapy w, 2022
83.��������� Wikipedia,
Energy medicine w, 2022
84.��������� Wikipedia,
Feldenkrais Method w, 2022
85.��������� Wikipedia,
Horticultural therapy w, 2022
86.��������� Wikipedia,
Myofascial release w, 2022
87.��������� Wikipedia,
Hydrotherapy w, 2022
88.��������� Wikipedia,
Numerology w, 2022
89.��������� Wikipedia,
Orthopathy w, 2022
90.��������� Wikipedia,
Radionics w, 2022
91.��������� Wikipedia,
Urine therapy w, 2022
92.��������� Wikipedia,
Paraherbal, w, 2022
93.��������� Wikipedia,
Wellness (alternative medicine) w, 2022
94.��������� Dr. Robert F. Stern and Mitchell Bebel
Stargrove, The History of Naturopathic Medicine ф, 2022
95.��������� Microsoft
Encarta, Circulation of the Blood c, 2009
96.��������� Microsoft
Encarta, Physicians c, 2009
97.��������� Microsoft
Encarta, Medical Ethics c, 2009
98.��������� Peter Whoriskey of Washignton Post,
The U.S. government is poised to withdraw longstanding
warnings about cholesterol - The Washington Post x, 2015
99.��������� Dariush Moza arian and David S.
Ludwig, The 2015 US Dietary Guidelines � Ending the 35% Limit
on Total Dietary Fat y, 2015
100.������� Prof. Oko
Offoboche, Natural Medicine z
101.������� Roy Porter,
The Cambridge Illustrated History of Medicine f, 1996
102.������ Music Therapy in Traditional African
Societies: Origin, Basis and Application in Nigeria Ʊ
Oko Offoboche, PhD,
D.Sc, FIIM, FIMC, FAIM
Professor of
Philosophy of Metaphysics, Doctor of Science of Information Systems
Fellow Institute of
Information Management, Fellow of Information Management Consultants, Fellow of
Association of Integrative Medicine Practitioners